Page 13 of 19
IM5.15-17 | Liver Disease Management — SDL Guide (Part 3)
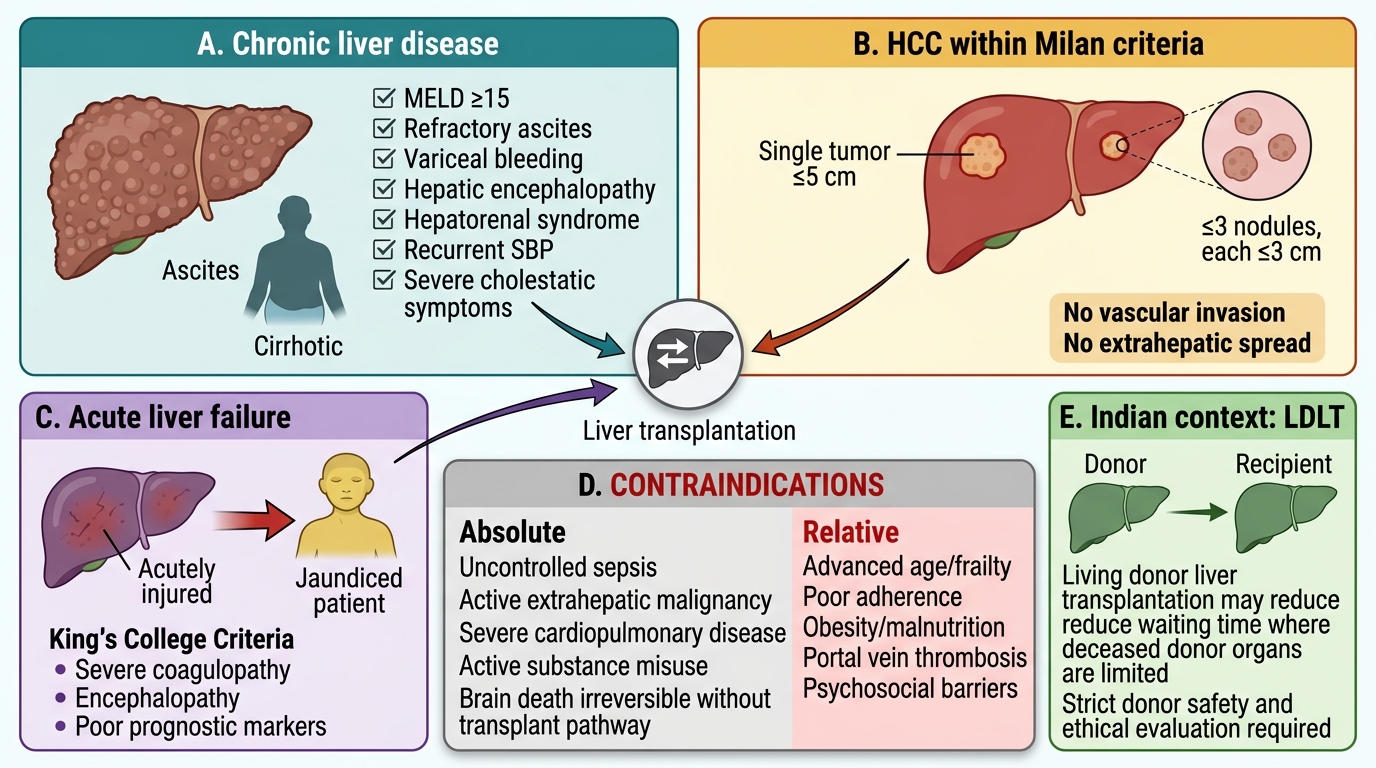
Indications for Liver Transplantation
Liver transplantation is the definitive treatment for end-stage liver disease and selected acute liver conditions. The IM5.17 competency requires the ability to enumerate the indications — meaning the physician must know when to refer a patient for transplant evaluation, not necessarily the technical conduct of the procedure. This is particularly important because the window for transplant referral can close if cirrhosis progresses to an irreversible state, or if HCC grows beyond the transplant criteria before referral. Early referral at the right MELD threshold or BCLC stage can be life-saving.
Indications for liver transplantation — organised by aetiology and urgency:
1. Chronic liver disease / decompensated cirrhosis:
The primary objective criterion is a MELD score ≥15 — this is the threshold at which the 90-day mortality without transplant exceeds the mortality associated with the procedure itself (approximately 3–5% peri-operative mortality at experienced centres). In practice, transplant referral is initiated at MELD ≥15 to allow time for evaluation, listing, and waiting. The indications include: decompensated cirrhosis from any aetiology (viral hepatitis B or C, alcoholic liver disease, NAFLD/NASH, autoimmune hepatitis, primary biliary cholangitis, primary sclerosing cholangitis, Wilson disease, haemochromatosis, alpha-1 antitrypsin deficiency); recurrent or refractory variceal haemorrhage not controlled by endoscopic and pharmacological management; recurrent SBP; diuretic-refractory ascites requiring frequent large-volume paracentesis; persistent hepatic encephalopathy despite medical management; and hepatopulmonary syndrome (pulmonary vasodilatation caused by cirrhosis) and portopulmonary hypertension (elevated pulmonary artery pressure in cirrhosis), both of which have priority listing status given their transplant-responsive nature.
2. Hepatocellular carcinoma (HCC):
The internationally accepted standard for transplant eligibility in HCC is the Milan criteria (Mazzaferro 1996): (a) single tumour ≤5 cm, OR (b) up to 3 tumours each ≤3 cm; in both cases, no macrovascular invasion and no extrahepatic metastases. Within Milan criteria, 5-year post-transplant survival exceeds 70% and HCC recurrence rate is <15% — results equivalent to transplantation for non-malignant cirrhosis. The expanded criteria (UCSF, up-to-7) have been validated in some programmes but are not universally adopted. Patients who are within Milan criteria but whose MELD score is too low for natural organ priority may receive MELD exception points (additional priority) to reflect their cancer-related urgency; however, in India where deceased donor transplantation is limited, most HCC transplants are performed using living donors.
3. Acute liver failure (ALF):
The King's College Criteria are used to identify ALF patients with insufficient chance of spontaneous recovery who require urgent transplantation:
- Paracetamol-induced ALF: pH <7.3 despite resuscitation, OR (all three of): prothrombin time >100 seconds (INR >6.5), creatinine >300 μmol/L (>3.4 mg/dL), and grade III–IV encephalopathy.
- Non-paracetamol ALF: INR >6.5 (PT >100 s), OR (any three of): age <10 or >40 years; non-A/non-B hepatitis, halothane hepatitis, or idiosyncratic drug reaction as aetiology; jaundice-to-encephalopathy interval >7 days; bilirubin >300 μmol/L; INR >3.5.
Other causes of ALF needing transplant consideration: Wilson disease presenting as ALF (most require transplant), autoimmune hepatitis ALF, Budd-Chiari syndrome, acute fatty liver of pregnancy (usually resolves post-delivery but may require transplant).
4. Metabolic and hereditary liver diseases:
Even before overt liver failure: Wilson disease with neurological disease unresponsive to chelation, hereditary oxalosis (liver-kidney combined transplant), familial amyloidotic polyneuropathy (FAP — domino transplantation), Crigler-Najjar syndrome type I (UGT1A1 complete absence — liver transplant cures neonatal jaundice before kernicterus).
Contraindications to liver transplantation:
- Absolute: active, untreated extrahepatic malignancy; AIDS (not HIV+ alone); active, uncontrolled systemic infection; active alcohol or substance misuse (most centres require 6 months of documented abstinence for ALD patients — though this threshold is debated); severe, irreversible cardiopulmonary disease precluding surgery; HCC outside accepted criteria (beyond Milan or equivalent) with documented extrahepatic spread.
- Relative: age >70 years (centre-dependent); severe obesity (BMI >40); prior non-hepatic malignancy with inadequate disease-free interval; severe frailty; poor psychosocial support.
Living-donor liver transplantation (LDLT): Particularly relevant in India where deceased donor transplantation is severely limited by low organ donation rates. LDLT uses the right lobe from a living donor (typically a first-degree relative or spouse). The donor undergoes a major hepatectomy with a post-operative mortality risk of approximately 0.1–0.5% at experienced centres. India has among the highest rates of LDLT globally, and understanding the donor selection process (compatible blood group, adequate graft volume, normal donor liver, no steatosis >10%) is relevant to the physician advising a family.
Indications and Contraindications for Liver Transplantation
SELF-CHECK
A 48-year-old man with hepatitis B-related cirrhosis is found on surveillance ultrasound to have a single liver lesion of 4.2 cm showing arterial enhancement and portal-phase washout on CT. His Child-Pugh score is B (8 points). MELD score is 13. HBV DNA is undetectable on TDF. Is this patient within the Milan criteria for liver transplantation?
A. No — Child-Pugh B excludes transplant listing regardless of tumour size
B. No — a lesion of 4.2 cm exceeds the Milan criteria single tumour limit of 3 cm
C. Yes — a single lesion of 4.2 cm (≤5 cm), no vascular invasion mentioned, no extrahepatic spread — meets Milan criteria
D. Yes — but only if MELD increases to ≥15 before listing is considered
Reveal Answer
Answer: C. Yes — a single lesion of 4.2 cm (≤5 cm), no vascular invasion mentioned, no extrahepatic spread — meets Milan criteria
The Milan criteria for HCC transplant eligibility are: (a) single tumour ≤5 cm, OR (b) up to 3 tumours each ≤3 cm; with no macrovascular invasion and no extrahepatic metastases. A single lesion of 4.2 cm is within the ≤5 cm threshold — this patient meets Milan criteria. Child-Pugh B is not an absolute contraindication to transplant listing. The MELD score of 13 is below the standard 90-day threshold for priority listing (MELD ≥15), but patients with HCC within Milan criteria often receive MELD exception points to prioritise them appropriately. The CT pattern (arterial enhancement + portal washout) is diagnostic of HCC in a cirrhotic patient, so biopsy is not needed before transplant evaluation.
Self-Assessment: Integrating Liver Disease Management
The following scenarios integrate management decisions across the full range of IM5.15–IM5.17 competencies. The self-assessment is designed around time-sensitive clinical decisions — the kind that must be executed correctly in the first 30 minutes of a patient's deterioration. Each scenario is anchored to a different complication of liver disease and requires you to identify: the diagnostic threshold that has been crossed, the correct first-line intervention, the pathophysiological rationale behind that intervention, and the monitoring parameter that confirms treatment response. These cases are not recall exercises — they test whether you can integrate diagnostic findings, threshold knowledge, and treatment protocol into a coherent clinical action.
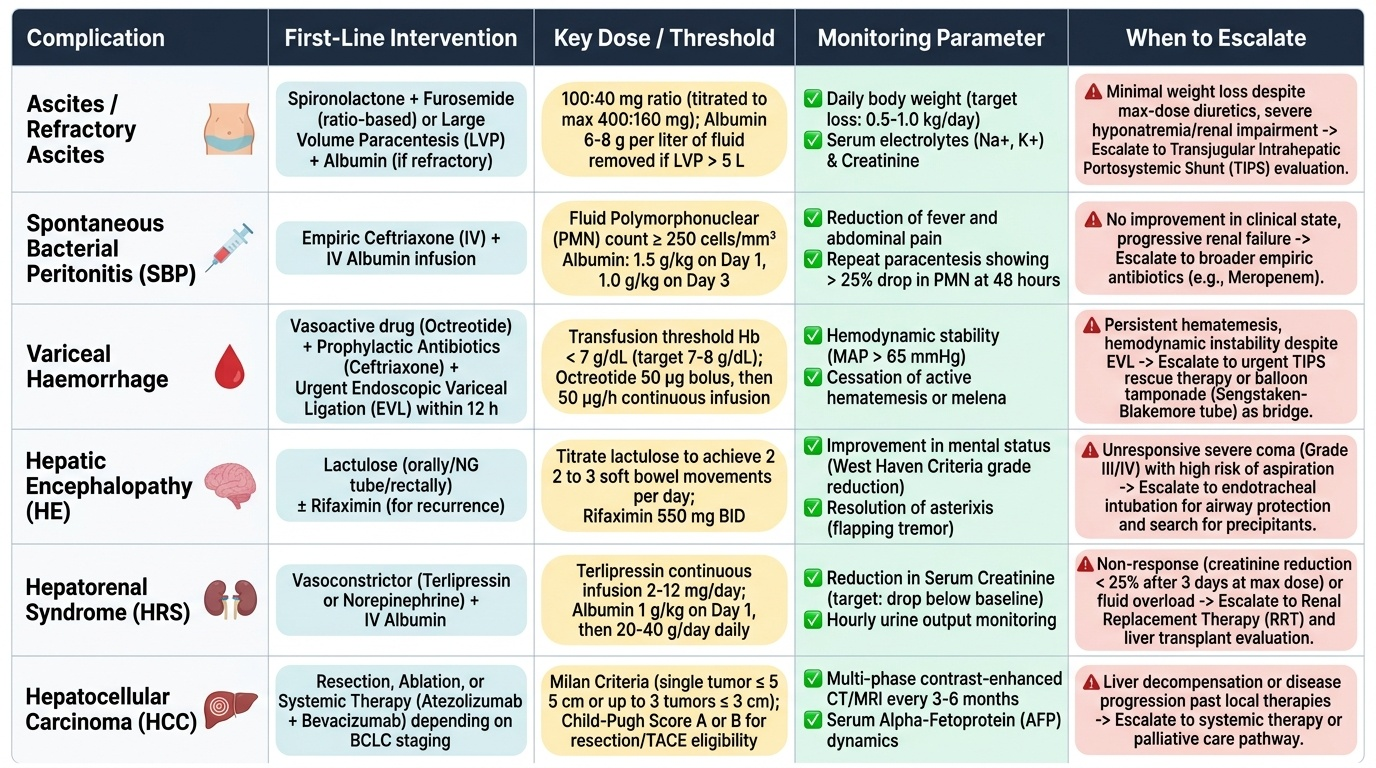
Provided image
Approach each scenario as you would at the bedside: read the case, decide your priority action before reading the analysis, then compare your reasoning to the structured management below. If you find yourself defaulting to the diagnosis rather than the action ('this is SBP' rather than 'ceftriaxone + albumin now'), you have identified a gap to close. Competency in this domain is defined by speed and sequence, not just knowledge of the individual interventions. For each patient in the opening hook — the cirrhotic with haematemesis, the patient with grade III encephalopathy, the cirrhotic with fever and ascites — the management framework you have built across this module should now yield the correct sequence of actions without hesitation.
Scenario A — Acute variceal haemorrhage: 47-year-old man with alcoholic cirrhosis (Child-Pugh C), vomiting fresh blood, BP 88/60, HR 122. Haemoglobin 7.1 g/dL.
Management: (1) Resuscitate: IV access ×2, cross-match, IV Hartmann's to BP ≥90 mmHg; transfuse to target Hb 7–8 g/dL (not higher — overtransfusion worsens portal pressure). (2) Terlipressin 2 mg IV bolus immediately — start BEFORE endoscopy. (3) IV ceftriaxone 1 g immediately — start simultaneously with terlipressin. (4) Airway protection — NG tube after securing airway. (5) Endoscopy within 12 hours — EVL. (6) Continue terlipressin for 3–5 days. Target: cessation of haemorrhage, maintenance of Hb >7 g/dL without further transfusion requirement. If bleeding continues after endoscopy + vasoactive drug: consider TIPS or balloon tamponade as bridge. Secondary prevention: propranolol + repeat EVL.
Scenario B — SBP and HRS: 55-year-old cirrhotic woman with known ascites develops fever 38.6°C and mild confusion. Paracentesis: PMN 380/mm³, total protein 14 g/L. Creatinine is 1.9 mg/dL (from baseline 0.8 mg/dL).
Management: SBP diagnosed (PMN ≥250/mm³). (1) IV ceftriaxone 1 g/day immediately. (2) IV albumin 1.5 g/kg at diagnosis — this patient has a rising creatinine indicating evolving HRS; albumin is both mandatory (Sort trial) and essential for HRS prevention here. (3) IV albumin 1 g/kg on day 3. (4) Withhold diuretics (contribute to AKI in this context). (5) Monitor creatinine daily. If creatinine does not improve after 48 hours of albumin + antibiotics, consider terlipressin (HRS-AKI developing in the context of SBP). (6) After recovery: secondary prophylaxis with norfloxacin 400 mg/day indefinitely. Long-term: this patient's MELD likely >20 — transplant evaluation.
Scenario C — HE management: 62-year-old cirrhotic man with grade III encephalopathy (GCS 12, gross confusion, incoherent). Nurse reports he had a malaena stool 2 days ago. Creatinine 1.1 mg/dL, Na 128 mEq/L, potassium 3.0 mEq/L.
Management: Multiple precipitants identified: GI bleed (malaena) + hyponatraemia + hypokalaemia (likely diuretic-related). (1) Identify and treat precipitants first: check Hb and endoscope if GI bleed active; oral potassium and careful fluid management for hyponatraemia; withhold diuretics. (2) Lactulose 20–30 mL every 2–4 hours until 2–3 soft stools/day; nasogastric administration if patient cannot swallow safely. (3) Airway assessment — grade III HE approaches intubation threshold; position semi-recumbent. (4) Rifaximin 550 mg twice daily to add if inadequate response to lactulose + precipitant treatment. (5) Protein intake 1.2–1.5 g/kg/day via NG tube if required — do NOT restrict protein. (6) Monitor GCS every 4 hours; re-check electrolytes after fluid/K replacement.
CLINICAL PEARL
The most common error in managing acute variceal haemorrhage is waiting to start terlipressin and antibiotics until after endoscopy. Both must start at the time of presentation. Terlipressin reduces portal pressure within minutes, significantly reducing the likelihood of ongoing haemorrhage and allowing endoscopy to be performed on a controlled field. Prophylactic antibiotics reduce the 7-day bacterial infection rate from ~20% to <10% and independently reduce rebleeding risk — the evidence for antibiotics in variceal haemorrhage is as strong as for terlipressin itself.
A second pearl on hepatic encephalopathy: never restrict protein in HE. The practice of protein restriction in HE is based on the theory that dietary protein provides ammonia substrate — but clinical trials show that protein restriction worsens sarcopenia and actually increases HE recurrence and mortality. The current recommendation is 1.2–1.5 g/kg/day, preferring vegetable and branched-chain amino acid sources. The ammonia load from a 2-litre GI haemorrhage far exceeds the daily dietary protein contribution — fix the bleed, fix the constipation, fix the infection first.