Page 9 of 23
IM6.9-12 | HIV Diagnostic Testing — SDL Guide
Learning Objectives
- Choose and interpret appropriate diagnostic tests to diagnose and classify the severity of HIV/AIDS including specific tests of HIV and CDC classification
- Choose and interpret appropriate diagnostic tests to diagnose opportunistic infections including CBC, sputum examination, cultures, blood cultures, stool analysis, and CSF analysis
- Enumerate the indications for and describe findings on CT chest, CT brain, and MRI brain in patients with HIV-related opportunistic infections
- Enumerate indications for and interpret pulse oximetry, ABG, and chest radiograph in patients with opportunistic infections
INSTRUCTIONS
Accurate and timely laboratory diagnosis underpins every clinical decision in HIV medicine — from confirming infection and staging severity, to identifying the causative organism in a life-threatening OI, to monitoring ART efficacy. This module covers HIV-specific diagnostic tests, laboratory workup of common OIs, and imaging interpretation, at the SH level as required by NMC competencies IM6.9–IM6.12.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 197 — Diagnosis and Laboratory Monitoring of HIV (textbook)
- API Textbook of Medicine, 10th ed., Section 13 — Investigations in HIV/AIDS (textbook)
- NACO Technical Guidelines for HIV Testing, 2018 (guideline)
- WHO Consolidated Guidelines on HIV Testing Services, 2019 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
The night shift nurse asks you to review the blood results for two patients. Patient A has been admitted with a two-week history of progressive dyspnoea and a CXR that the admitting team called 'bilateral haziness.' His SpO₂ is 84% on room air; his LDH is 890 IU/L. The HIV test result is pending. Patient B has just been diagnosed HIV-positive in the outpatient clinic; he feels well, but the nurse asks you which blood tests to order to complete the workup. Two different clinical scenarios, both requiring you to choose the right investigations, in the right order, and interpret the results correctly. Choosing the wrong test — or misinterpreting the result — leads to delayed diagnosis, inappropriate treatment, and preventable death. This module teaches you to think like a diagnostician in HIV medicine.
WHY THIS MATTERS
Laboratory diagnosis in HIV is a two-layer problem. The first layer is confirming HIV infection itself — using the correct testing algorithm to avoid false positives and false negatives. The second layer is diagnosing the opportunistic infections that develop as immune function collapses — each OI has a characteristic laboratory and imaging signature that the clinician must recognise. For the NMC IM6.9–IM6.12 competencies, tested at the SH (interpret and choose investigations) level, you must: select the right HIV test for the clinical context (screening vs confirmation vs acute infection); interpret CD4 count and viral load in terms of disease stage and ART monitoring; order the OI-specific investigations appropriate for the clinical presentation; interpret CXR and imaging findings; and read a chest X-ray and ABG in a patient with respiratory compromise. These are practical, high-stakes competencies assessed in final-year OSCEs and exit examinations.
RECALL
Recall that HIV diagnosis depends on detecting either antibodies (anti-HIV IgG), viral antigen (p24 antigen), or viral nucleic acid (HIV RNA or DNA). Antibodies require 3–12 weeks to appear after infection (the window period); p24 antigen is detectable earlier (2–4 weeks); HIV RNA is the earliest marker (10–12 days). The generation of HIV tests reflects which markers they detect: first and second generation detect IgG antibodies only; third generation detects IgG + IgM; fourth generation (current standard) detects p24 antigen AND antibodies, significantly closing the window period. Recall that CD4 count is a measure of immune competence (normal 500–1500 cells/µL; AIDS-defining <200 cells/µL) and viral load is the plasma HIV RNA concentration, measured in copies/mL, which reflects active viral replication and the efficacy of ART.
Clinical Indication: When to Test for HIV
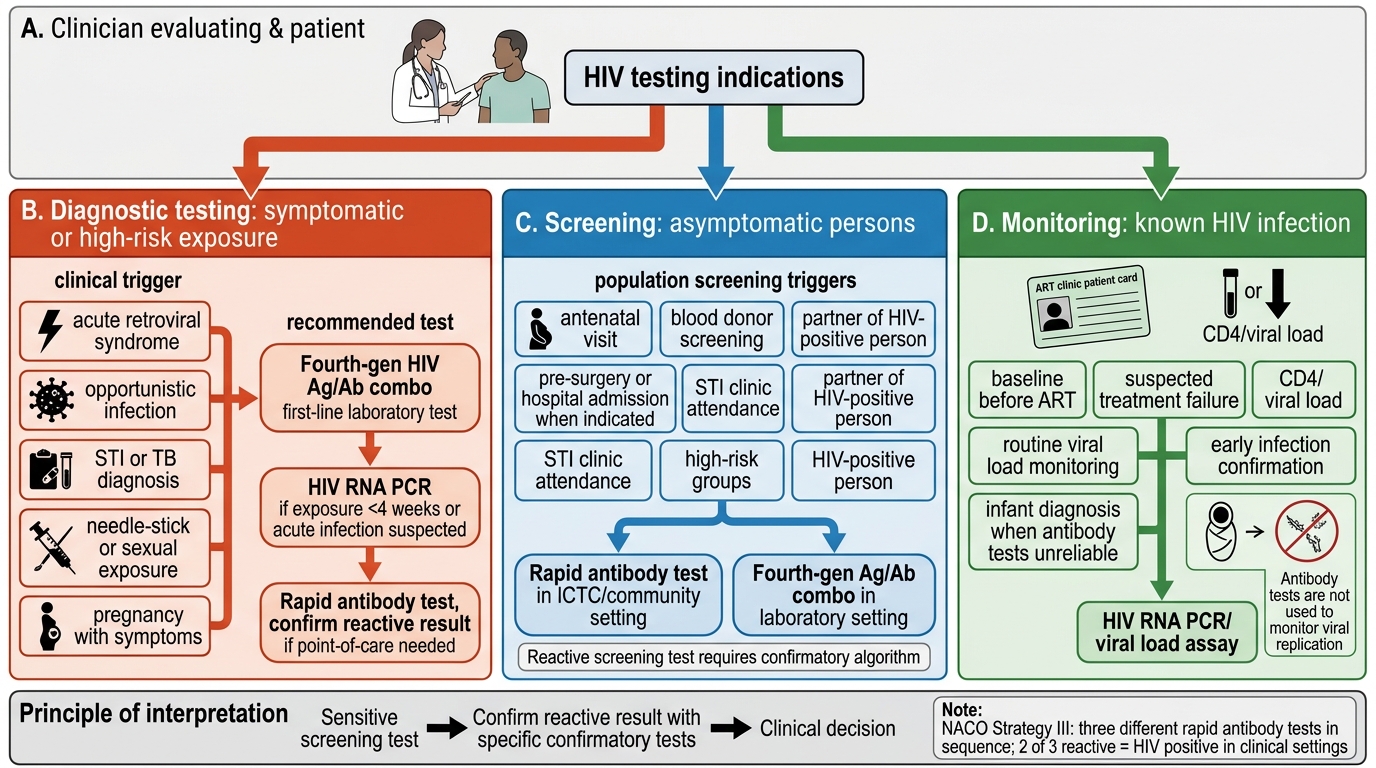
The indications for HIV testing span a wide clinical spectrum and form the entry point for all HIV-specific diagnostic decision-making. Recognising when to test — and which test to order — is itself a clinical skill that prevents both under-diagnosis (missed HIV in a patient presenting with an OI) and inappropriate testing (ordering a point-of-care antibody test in a patient with suspected acute seroconversion, when the test will be falsely negative). The clinical indications for HIV testing can be grouped into three categories: diagnostic testing for a patient with HIV-associated symptoms, screening in asymptomatic individuals at risk, and monitoring in a known PLHIV.
Diagnostic testing indications: Any patient presenting with: unexplained prolonged fever (>1 month), unexplained weight loss (>10%), recurrent bacterial infections, oral candidiasis, oral hairy leucoplakia, unexplained lymphadenopathy, herpes zoster in a young adult (<50 years), unexplained cytopenias, TB (both pulmonary and extrapulmonary), any sexually transmitted infection (STI), unexplained neurological symptoms (meningitis, encephalopathy, focal neurology), PCP-pattern respiratory failure, or diarrhoea lasting >1 month. In India, NACO's Provider-Initiated Testing and Counselling (PITC) guidelines recommend offering HIV testing to all patients attending STI clinics, TB clinics, antenatal clinics, and any patient with symptoms or conditions associated with HIV.
Screening indications: All pregnant women (antenatal HIV testing as part of PPTCT programme); individuals with known HIV-positive partners; history of unprotected sexual intercourse with multiple partners; injecting drug users; men who have sex with men (MSM); commercial sex workers; persons with history of blood transfusion before universal blood screening; healthcare workers post-needlestick.
Monitoring indications: Known PLHIV on ART — CD4 count and viral load are ordered at baseline, 6 months after ART initiation, and then every 6–12 months to monitor treatment response and detect virological failure.
HIV Testing Indications and Test Selection
HIV-Specific Diagnostic Tests: Principles and Interpretation
The HIV diagnostic algorithm follows a hierarchical sequence: a highly sensitive screening test is used first, and any reactive result must be confirmed by a more specific confirmatory test. The NACO HIV testing strategy (Strategy III) for India uses a three-test algorithm in clinical settings: three different HIV rapid antibody tests in sequence, with the result defined by a majority rule (2/3 reactive = HIV positive). Fourth-generation laboratory assays and molecular tests are available at referral centres and ART centres.
Fourth-generation HIV Ag/Ab combination assay (ELISA/CLIA): This is the recommended screening test for HIV in laboratory settings. It simultaneously detects p24 antigen and anti-HIV-1/2 IgG and IgM antibodies. Advantages: closes the window period to as little as 18–45 days post-exposure (vs 45–90 days for antibody-only assays); automated and high-throughput. A reactive fourth-generation assay is followed by a confirmatory test. If the fourth-generation assay is reactive and the patient reports a recent high-risk exposure (<4 weeks ago), the p24 antigen component provides the early positive signal even before antibodies appear.
HIV Western blot / Line immunoassay: Historically used as the gold standard confirmatory test; detects antibodies to individual HIV proteins (p24, gp41, gp120/160). A positive Western blot requires bands for ≥2 of: p24, gp41, gp120/gp160. However, Western blot has been largely replaced by the HIV-1/HIV-2 antibody differentiation assay in the current WHO/CDC testing algorithm (2014 recommended algorithm), which uses a supplemental immunoassay to differentiate HIV-1 from HIV-2 antibodies in reactive samples.
HIV RNA quantitative PCR (viral load): Detects and quantifies HIV RNA in plasma. Uses: (1) diagnosis in the window period (detectable from day 10–12 post-infection, weeks before antibodies appear); (2) diagnosis of HIV in infants born to HIV-positive mothers (maternal antibodies cross the placenta and persist for up to 18 months, making antibody tests unreliable — infant diagnosis requires HIV DNA PCR or HIV RNA from dried blood spot at 6 weeks and 9 months); (3) monitoring ART efficacy — viral load should be undetectable (<50 copies/mL or <20 copies/mL depending on the assay) by 6 months of ART; a detectable viral load at 6 months signals virological failure.
CD4 count (CD4+ T lymphocyte count): Measured by flow cytometry; reported as absolute count (cells/µL) and/or CD4 percentage. Clinical uses: staging HIV disease, determining urgency of ART initiation (before 'Treat All' era), guiding prophylaxis thresholds (co-trimoxazole at CD4 <250 per NACO; CrAg screen at CD4 <100), monitoring immune reconstitution on ART. A normal CD4 count of ≥500 cells/µL on ART for ≥6 months indicates good immune reconstitution. CD4 count alone is not used to diagnose HIV — it confirms staging.
HIV resistance testing: Genotypic or phenotypic testing for antiretroviral drug resistance mutations. Indicated at virological failure (viral load >1000 copies/mL on two consecutive measurements on ART). NACO guidelines at second-line and third-line ART switch points.
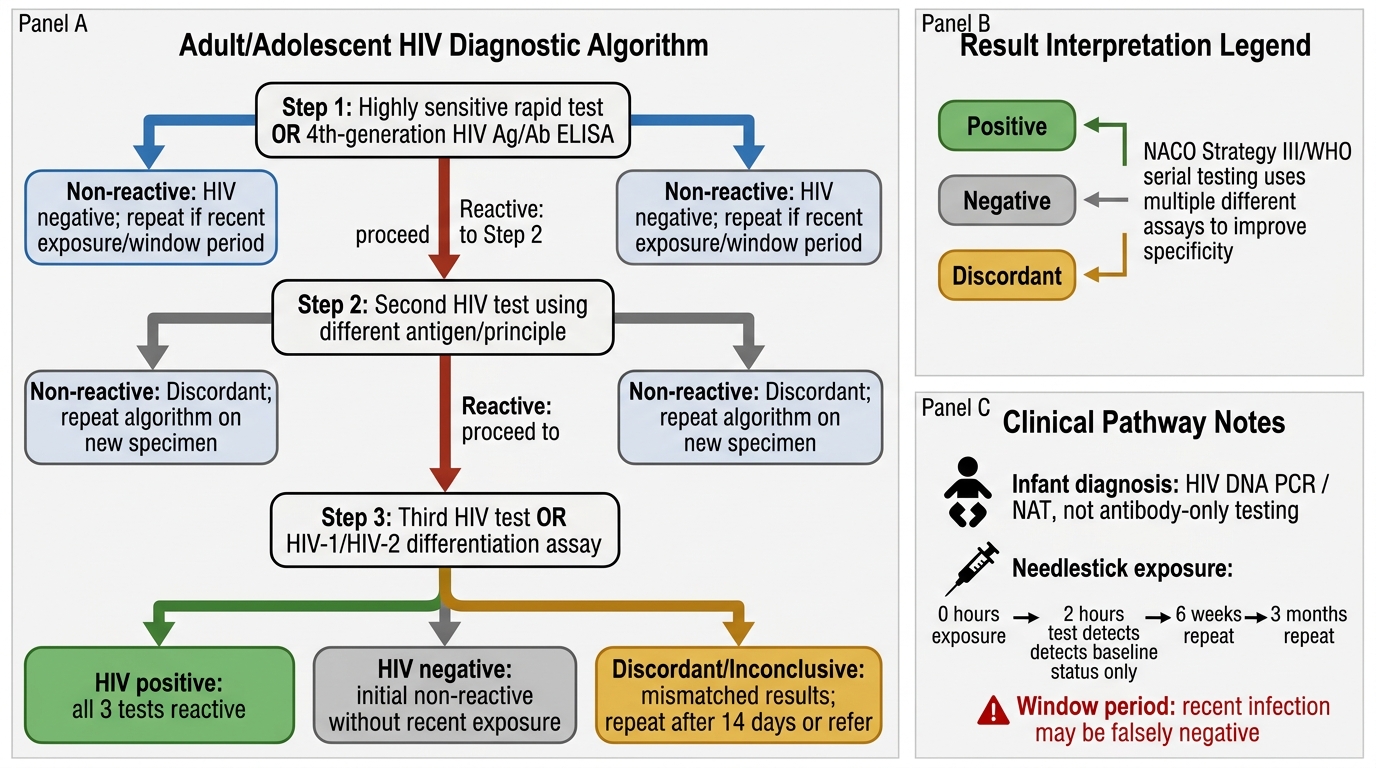
HIV Diagnostic Algorithm: NACO Strategy III / WHO Serial Testing
SELF-CHECK
A 27-year-old healthcare worker sustains a needlestick injury from a known HIV-positive patient. She presents to the casualty 2 hours later. She is started on post-exposure prophylaxis (PEP). HIV testing is performed: the fourth-generation Ag/Ab combination ELISA is negative. What is the CORRECT interpretation of this result?
A. She is not HIV-infected; no further testing is needed
B. The result is indeterminate; she needs a Western blot immediately
C. The result may be falsely negative due to the window period; repeat testing at 6 weeks and 3 months is mandatory
D. A negative fourth-generation test 2 hours post-exposure confirms no infection has occurred
Reveal Answer
Answer: C. The result may be falsely negative due to the window period; repeat testing at 6 weeks and 3 months is mandatory
HIV testing immediately after a needlestick injury detects the pre-existing HIV status, not recent infection — a negative result at 2 hours simply means she had no prior HIV infection before this injury. The window period for the fourth-generation Ag/Ab assay is 18–45 days; any new infection from this exposure would not be detectable for at least 2–4 weeks (RNA) to 18–45 days (Ag/Ab). Repeat testing at 6 weeks and 3 months (and optionally 6 months) is mandatory to rule out new infection from the exposure. PEP, if started within 72 hours, is highly effective and should be completed for 28 days.
Laboratory Diagnosis of Opportunistic Infections
Each opportunistic infection has a specific combination of laboratory tests that confirm the diagnosis, assess severity, and guide treatment. The choice of investigations is driven by the presenting symptom complex, the CD4 count context, and the anatomical site of infection. Selecting the correct test requires knowing three properties of each diagnostic test: its sensitivity (will it detect the infection if present?), its specificity (will it be positive only for that infection?), and its availability at the level of care where you are working. In a district hospital, the available tests are different from those in a tertiary referral centre — and the clinician who can work with India ink stain, modified acid-fast stain, and a serum LDH is more practically equipped than one who defaults to tests unavailable outside specialist centres. What follows is a systematic guide to OI-specific laboratory investigations organised by anatomical site, with explicit notes on test sensitivity, the gold standard, and practical district-hospital alternatives.
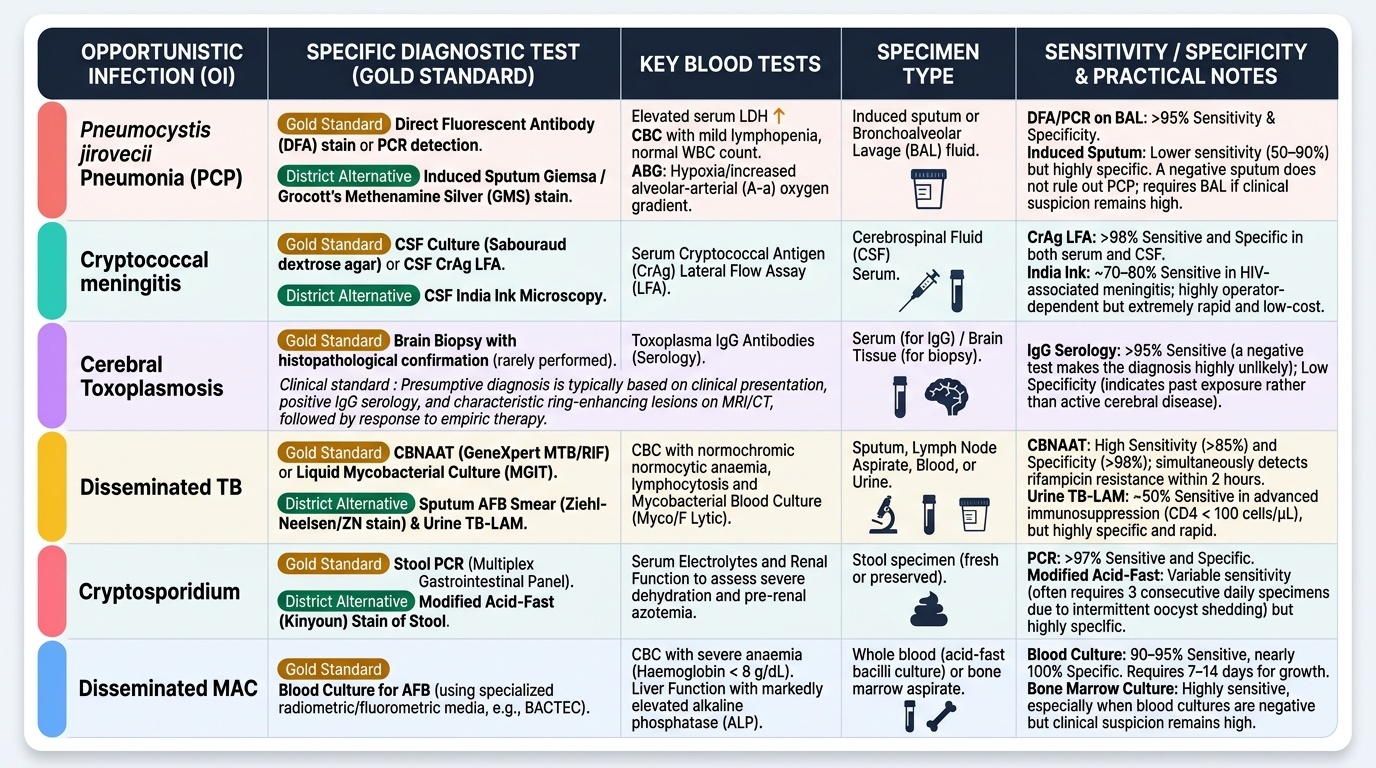
Provided image
Respiratory OIs — CBC, sputum, CXR, ABG:
- Complete blood count (CBC): In PCP, CBC is often near-normal (mild lymphopaenia); in TB, there may be normochromic normocytic anaemia, lymphocytosis; in MAC, severe anaemia (haemoglobin <8 g/dL) with elevated alkaline phosphatase is characteristic. Neutropaenia suggests drug toxicity (zidovudine) or CMV bone marrow infiltration.
- Sputum examination: For TB, the NTEP algorithm uses CBNAAT (cartridge-based nucleic acid amplification test — Xpert MTB/RIF) as the preferred initial test for HIV-positive patients with respiratory symptoms; it simultaneously detects Mycobacterium tuberculosis AND rifampicin resistance (a surrogate for MDR-TB) within 2 hours. Sputum AFB smear (ZN stain) is less sensitive in HIV (atypical presentations, lower bacillary load). For PCP diagnosis, induced sputum with silver stain (Grocott's methenamine silver — GMS) or immunofluorescence detects Pneumocystis cysts; sensitivity ~60% (BAL: ~90%).
- Serum LDH: In PCP, LDH is markedly elevated (typically >500 IU/L, often 700–1000 IU/L) due to alveolar damage; LDH >500 with bilateral ground-glass infiltrates in an HIV patient is highly suggestive of PCP. It also correlates with severity and prognosis.
- Serum (1→3)-β-D-glucan: Elevated in PCP (specificity ~90% in HIV respiratory presentations); a useful adjunct when BAL is not available.
- Bronchoalveolar lavage (BAL): Gold standard for PCP diagnosis (GMS stain sensitivity ~90%); also used for culture of atypical mycobacteria and fungi.
CSF analysis for neurological OIs:
- India ink stain: Simple, cheap, rapid; detects the cryptococcal capsule as a clear halo around yeast cells on dark background; sensitivity ~70% in cryptococcal meningitis.
- Cryptococcal antigen (CrAg) detection: The most sensitive test for cryptococcal meningitis; lateral flow assay (LFA) or ELISA in CSF — sensitivity >95%. Serum CrAg is also highly sensitive and can detect disseminated cryptococcal disease before CNS involvement (used in NACO screening programme at CD4 <100).
- CSF cytology and chemistry: In cryptococcal meningitis: elevated opening pressure (often >25 cm H₂O, sometimes extremely elevated >40 cm H₂O); mildly elevated protein (unlike bacterial meningitis, which is markedly elevated); mildly reduced glucose (mild hypoglycorrhachia); pleocytosis is mild or absent (lymphocytes) — the minimal cellularity at very low CD4 counts reflects the blunted immune response. In TB meningitis: elevated protein (>100 mg/dL), reduced glucose (<45% of simultaneous blood glucose), lymphocytic pleocytosis (100–500 cells), fibrin web on standing; CSF culture/Xpert for MTB.
- CSF Toxoplasma PCR: Available in referral labs; limited sensitivity (~50%) but high specificity; useful when the empirical toxoplasmosis treatment trial has failed and brain biopsy is being considered.
- CSF EBV PCR: Highly sensitive and specific for primary CNS lymphoma in HIV — a positive CSF EBV PCR in the appropriate clinical setting (single ring-enhancing lesion, failure to respond to toxoplasmosis treatment) strongly supports PCNSL.
Stool analysis for GI OIs:
- Stool microscopy: Modified acid-fast stain (MAFS) detects Cryptosporidium oocysts (4–6 µm, pink spheres on blue background) and Isospora belli (larger, oval, 10–19 µm) and Cyclospora. Routine stool cultures (bacterial) will be negative in Cryptosporidium/Isospora — the modified acid-fast stain must be specifically requested.
- Stool PCR/ELISA: More sensitive for Cryptosporidium and Microsporidiosis (microsporidia detected by trichrome stain on electron microscopy — spores 1–3 µm; standard light microscopy misses them).
- Blood culture: Salmonella bacteraemia (recurrent Salmonella septicaemia is AIDS-defining) — use aerobic blood culture; sensitivity ~70%. Disseminated MAC — lysis-centrifugation blood culture (Isolator system) is the gold standard; routine blood cultures are inadequate for mycobacterial recovery.
Blood tests for MAC and CMV:
- Alkaline phosphatase: Markedly elevated in disseminated MAC (enzyme from hepatic MAC involvement); often >5× upper limit of normal.
- CMV pp65 antigenaemia or CMV DNA PCR (plasma): For diagnosis of CMV disease; CMV DNA PCR is the preferred quantitative test (result in copies/mL or IU/mL); elevated in CMV retinitis, CMV encephalitis, CMV colitis.
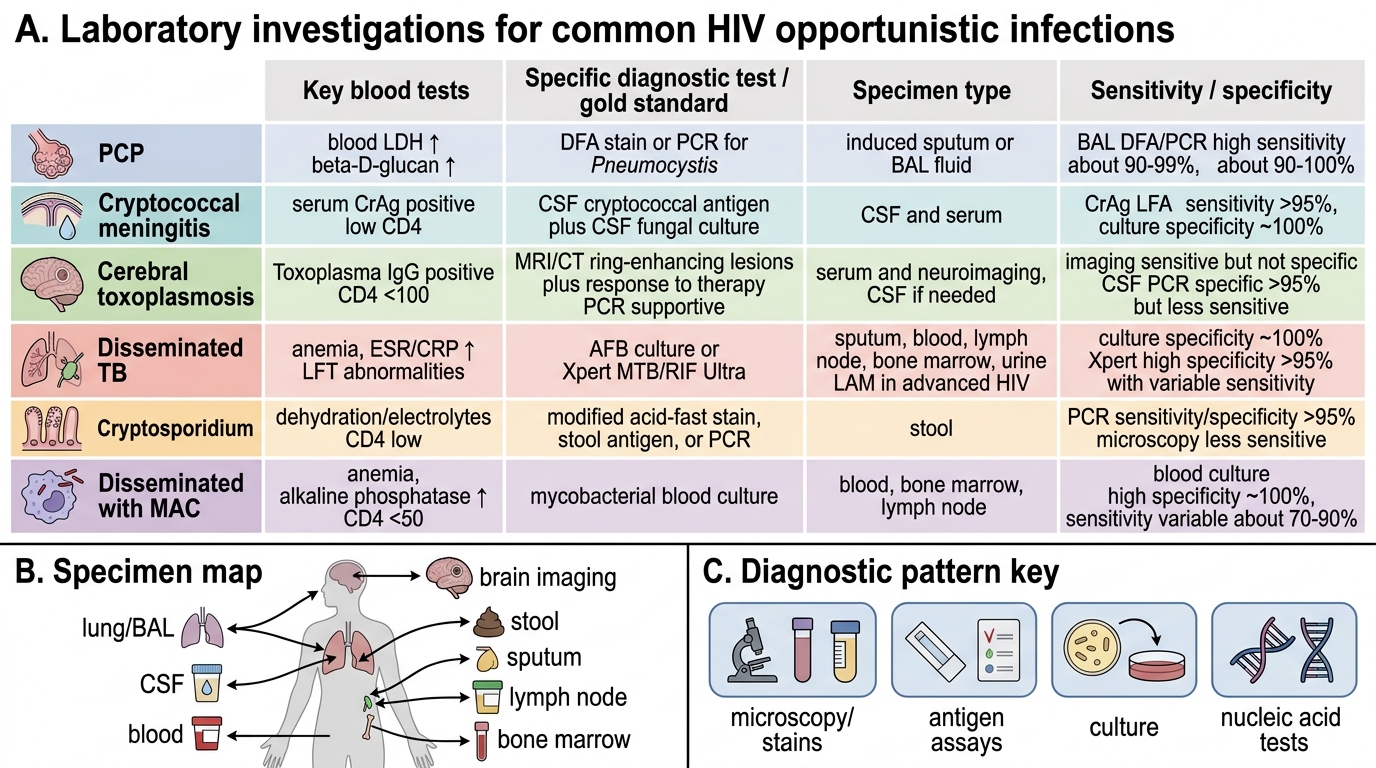
Laboratory Diagnosis of Common HIV Opportunistic Infections