Page 13 of 23
IM6.13-17 | HIV Treatment and Prophylaxis — SDL Guide
Learning Objectives
- Describe the indications and side effects of drugs used for bacterial, viral, and other types of diarrhoea in HIV/AIDS
- Discuss the principles of HAART, the classes of antiretroviral drugs, and their mechanisms of action
- Describe the pathogenesis of immune reconstitution inflammatory syndrome (IRIS) and its management
- Discuss the principles and regimens used in post-exposure prophylaxis (PEP)
- Enumerate the indications for and discuss prophylactic drugs used to prevent HIV-related opportunistic infections
INSTRUCTIONS
HIV treatment has been transformed from managing a fatal illness to achieving near-normal life expectancy with effective antiretroviral therapy. This module covers the mechanistic basis of antiretroviral drug classes, the NACO first-line TLD regimen, principles of OI prophylaxis, PEP/PrEP regimens, and the management of IRIS — all at the KH level required by NMC competencies IM6.13–IM6.17.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 197 — Treatment of HIV Infection (textbook)
- API Textbook of Medicine, 10th ed., Section 13 — Antiretroviral Therapy (textbook)
- NACO Operational Guidelines for ART Programmes, 2022 — First, Second, and Third Line ART (guideline)
- WHO Consolidated Guidelines on HIV Prevention and Treatment, 2021 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Three clinical encounters in the same morning clinic at an ART centre. First: a 35-year-old man, newly diagnosed HIV, CD4 count 180 cells/µL, feels well, no active OI — his wife asks when he should start medicines. Second: a 27-year-old nurse who had a needlestick injury from an HIV-positive patient six hours ago — she wants to know if she needs to take tablets and for how long. Third: a 40-year-old woman who started ART four weeks ago for tuberculosis co-infection — she has deteriorating chest X-ray and worsening fever since starting ART, and the registrar is worried the ART is 'not working.' These three encounters span the breadth of HIV treatment decision-making: treatment initiation, post-exposure prophylaxis, and immune reconstitution inflammatory syndrome. Mastering the treatment principles in this module equips you to handle all three correctly.
WHY THIS MATTERS
Antiretroviral therapy (ART) has transformed HIV from a near-universally fatal illness to a manageable chronic condition with a life expectancy approaching that of the general population, provided treatment is initiated early and adhered to consistently. Under NACO's 'Treat All' policy, every diagnosed PLHIV in India is entitled to free ART regardless of CD4 count — this makes treatment initiation decision-making universal, not selective. For the final-year MBBS graduate, the KH-level competencies IM6.13–IM6.17 require: knowing the drug classes and mechanisms of action, understanding first-line NACO regimen (TLD), recognising and managing IRIS, applying PEP and PrEP principles, and prescribing OI prophylaxis at the correct CD4 thresholds. These are core competencies tested in exit examinations and essential for practice in any district hospital or primary care setting in India.
RECALL
Recall the HIV replication cycle, which is the mechanistic basis for all antiretroviral drug classes. HIV enters the host cell via gp120-CD4 binding and co-receptor engagement (CCR5 or CXCR4). After fusion, the RNA genome is reverse-transcribed into DNA by reverse transcriptase — the first drug target. The viral DNA is integrated into the host chromosome by integrase — the second drug target. The integrated provirus is transcribed; viral proteins are produced as polyprotein precursors, which are cleaved into functional proteins by protease — the third drug target. Newly assembled virions bud from the cell surface. Each antiretroviral drug class targets one or more of these steps. Recall also that NACO's current first-line regimen changed from efavirenz-based (EFV) to dolutegravir-based (DTG) — reflecting superior efficacy, resistance barrier, and tolerability of DTG.
Clinical Presentation: Indications and Urgency of ART Initiation
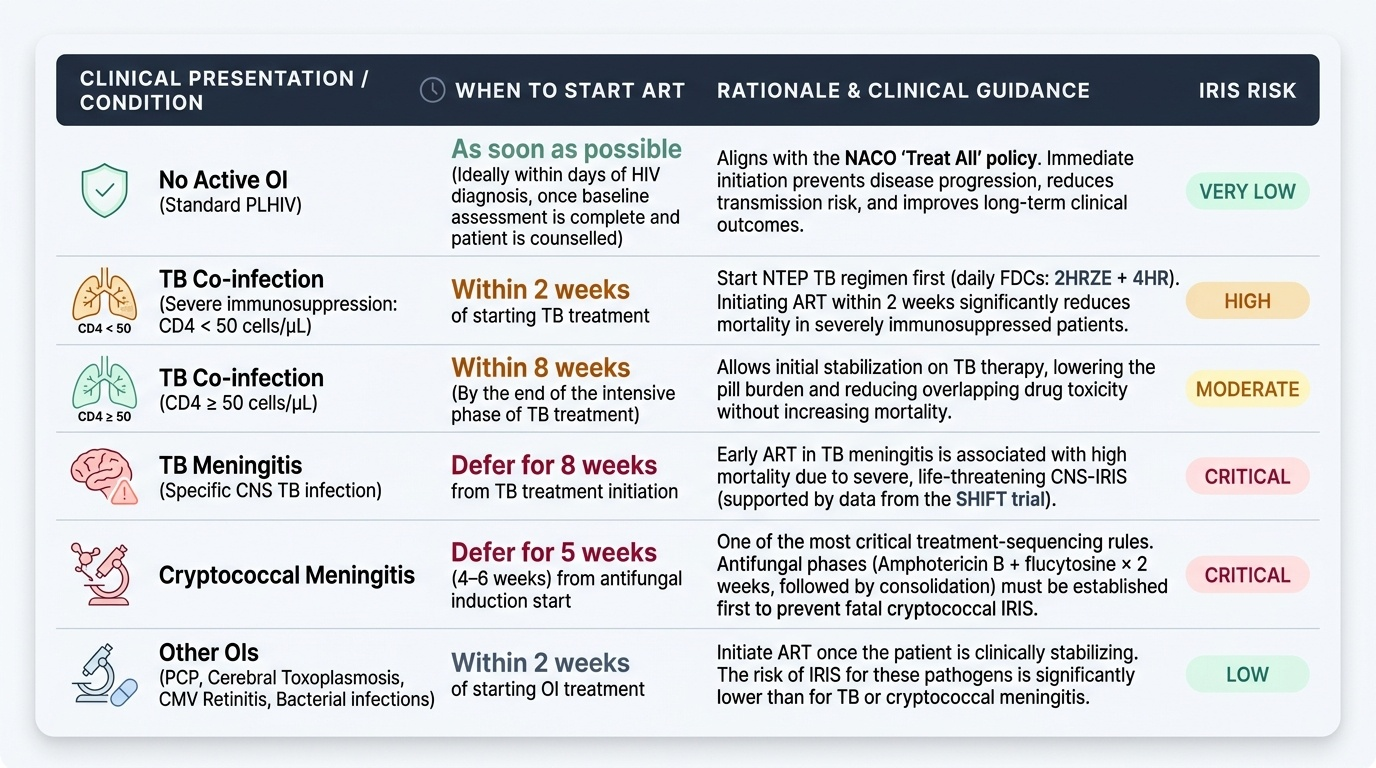
Under the NACO 'Treat All' policy, ART is indicated for all PLHIV regardless of CD4 count, WHO clinical stage, or symptoms. However, the timing and urgency of ART initiation vary based on the clinical context, particularly the presence of active opportunistic infections. Understanding these nuances is clinically essential — initiating ART too early in specific OIs (particularly cryptococcal meningitis) carries a serious risk of immune reconstitution inflammatory syndrome (IRIS), while delaying ART in others (TB co-infection) increases the risk of disease progression and death.
Provided image
General rule: ART should be initiated as soon as possible after HIV diagnosis in all patients — ideally within days of diagnosis, once the baseline assessment is complete and the patient is counselled.
TB-HIV co-infection: Initiate TB treatment first (NTEP regimen: 2HRZE + 4HR, weight-band based, daily FDCs). Start ART within 2 weeks of TB treatment initiation if CD4 <50 cells/µL; start within 8 weeks (by the end of the intensive phase) if CD4 ≥50 cells/µL. Earlier ART in patients with CD4 <50 reduces mortality. The exception is TB meningitis — in this specific case, ART is deferred for 8 weeks from TB treatment start, as early ART initiation in TB meningitis is associated with increased mortality (data from the SHIFT trial and its predecessor studies), likely due to IRIS in the CNS.
Cryptococcal meningitis: ART is deferred for 5 weeks (4–6 weeks) from the start of antifungal induction therapy. This is one of the most important treatment-sequencing rules in HIV medicine — initiating ART early in cryptococcal meningitis significantly increases the risk of cryptococcal IRIS, which is associated with high mortality in this setting. The antifungal induction phase (Amphotericin B + flucytosine × 2 weeks), consolidation (fluconazole 400 mg × 8 weeks), and the first weeks of maintenance (fluconazole 200 mg daily) should be established before ART is started.
Other OIs: For PCP, cerebral toxoplasmosis, CMV retinitis, and bacterial infections — initiate ART within 2 weeks of OI treatment, once the patient is clinically stabilising. IRIS risk in these OIs is lower than with cryptococcal meningitis and TB.
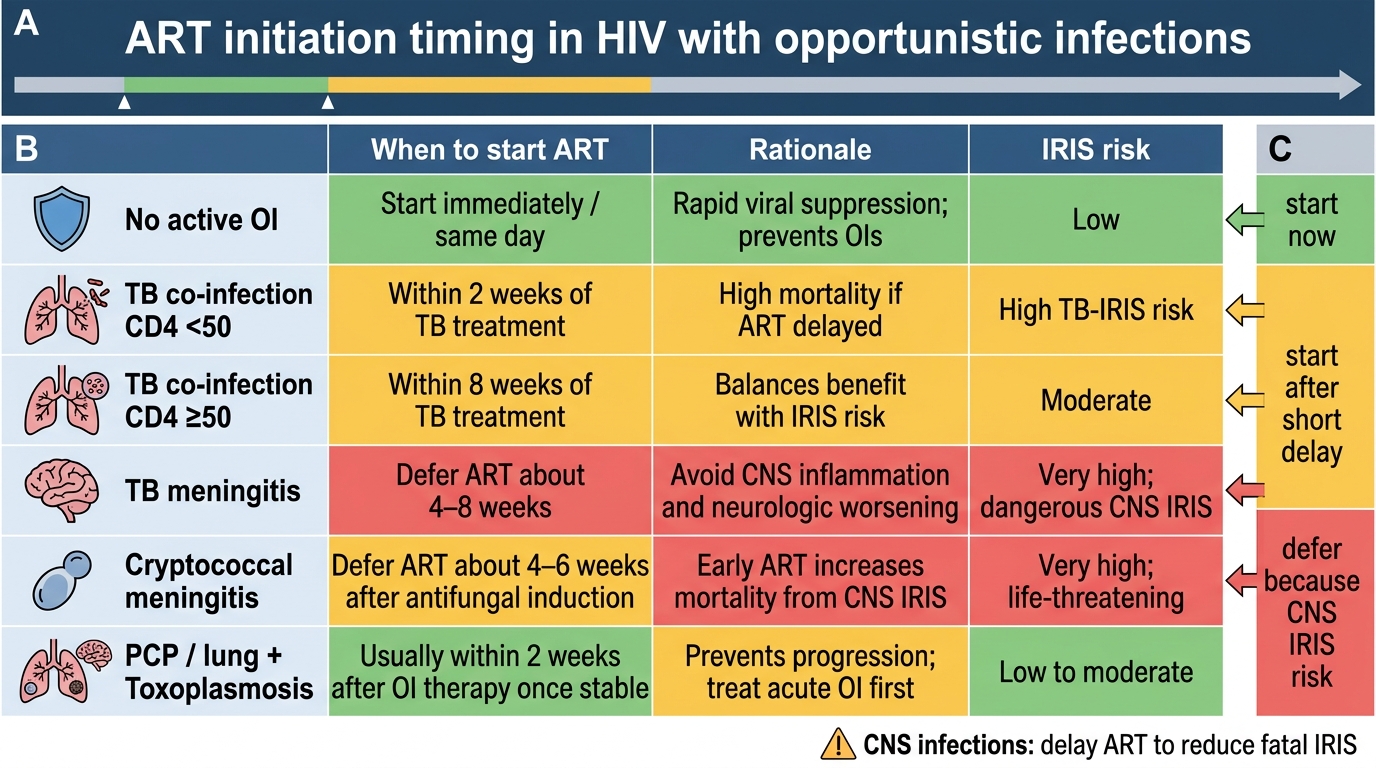
ART Initiation Timing in HIV with Opportunistic Infections
Principles of HAART: Drug Classes and Mechanisms
Highly Active Antiretroviral Therapy (HAART) — now simply called antiretroviral therapy (ART) or combination ART (cART) — refers to the use of at least three antiretroviral drugs from two or more drug classes to achieve complete viral suppression (undetectable viral load). The rationale for combination therapy is mathematical: HIV reverse transcriptase makes approximately one error per genome replication cycle, and with 10⁹–10¹⁰ virions produced daily, resistance mutations arise spontaneously and constantly. A single-drug regimen allows resistant mutants to be selected; triple therapy reduces the probability of pre-existing triple-resistant mutants to effectively zero for current drugs, preventing resistance emergence. The goal of ART is to suppress the plasma viral load to below the detection threshold of the assay (<50 copies/mL), which: halts CD4 cell depletion, allows immune reconstitution, prevents OIs, prevents HIV transmission (Undetectable = Untransmittable, U=U), and reduces the reservoir of infected cells over time.
The antiretroviral drug classes and their mechanisms:
1. Nucleoside/Nucleotide Reverse Transcriptase Inhibitors (NRTIs/NtRTIs): Act as chain terminators — incorporated into the growing viral DNA chain as nucleoside/nucleotide analogues, they lack the 3'-hydroxyl group needed for further chain elongation, terminating reverse transcription. Examples: Tenofovir disoproxil fumarate (TDF) — a nucleotide analogue (NtRTI), active against both HIV and HBV; renal toxicity (Fanconi syndrome, reduced eGFR) and bone density loss with long-term use; preferred over zidovudine in NACO first-line. Lamivudine (3TC) — NRTI, minimal toxicity, active against HBV. Zidovudine (AZT/ZDV) — NRTI, used in PPTCT regimens; causes bone marrow suppression (macrocytic anaemia, neutropaenia). Abacavir (ABC) — NRTI, hypersensitivity reaction (HLA-B*57:01 associated; test before use). Emtricitabine (FTC) — similar to 3TC, active against HBV.
2. Non-Nucleoside Reverse Transcriptase Inhibitors (NNRTIs): Bind to an allosteric site on reverse transcriptase (not the catalytic site), causing conformational change that inhibits polymerase activity. A single point mutation (K103N, Y181C) can confer high-level resistance to most NNRTIs — the low genetic barrier to resistance. Examples: Efavirenz (EFV) — first-line NNRTI in many settings; CNS side effects (vivid dreams, dizziness, depression — usually transient, resolving in 2–4 weeks; take at bedtime); teratogenic (neural tube defects) — avoid in first trimester. Nevirapine (NVP) — used in PPTCT infant prophylaxis; hepatotoxicity and Stevens-Johnson syndrome risk. Rilpivirine (RPV) — newer NNRTI, fewer CNS effects than EFV; must be taken with food; not for viral load >100,000 copies/mL.
3. Integrase Strand Transfer Inhibitors (INSTIs): Block the integrase enzyme that catalyses the insertion (integration) of viral DNA into the host chromosome. High genetic barrier to resistance (multiple mutations needed). Examples: Dolutegravir (DTG) — the integrase inhibitor in NACO's current first-line regimen; superior resistance barrier vs raltegravir and elvitegravir; excellent tolerability; avoid in first trimester (neural tube defect risk, though small — updated guidance allows DTG throughout pregnancy when benefits outweigh risks). Raltegravir (RAL), Bictegravir (BIC).
4. Protease Inhibitors (PIs): Block HIV protease, which cleaves polyprotein precursors into functional viral proteins; virions are produced but non-infectious. High genetic barrier to resistance (multiple mutations required). All PIs are pharmacologically boosted: ritonavir (RTV) or cobicistat are added at low doses to inhibit CYP3A4, increasing the plasma concentration of the primary PI. Examples: Lopinavir/ritonavir (LPV/r) — second-line PI in NACO regimen; GI side effects (nausea, diarrhoea), metabolic effects (dyslipidaemia, hyperglycaemia), pancreatitis risk. Atazanavir/ritonavir (ATV/r) — indirect hyperbilirubinaemia (benign jaundice from UGT1A1 inhibition). Darunavir/ritonavir (DRV/r) — third-line, highest resistance barrier among PIs.
5. Entry Inhibitors: Block viral entry into the host cell. Fusion inhibitors (enfuvirtide — subcutaneous, injection site reactions; rarely used). CCR5 antagonists (maraviroc — requires tropism testing to confirm CCR5 co-receptor use; not for CXCR4 or dual-tropic virus).
NACO first-line ART regimen (2022): TLD = Tenofovir (TDF 300 mg) + Lamivudine (3TC 300 mg) + Dolutegravir (DTG 50 mg) — once-daily single tablet, replacing the previous TLE (TDF + 3TC + EFV) regimen. TLD has superior virological efficacy, higher resistance barrier (DTG vs EFV), better tolerability (fewer CNS side effects vs EFV), and lower pill burden. Contraindications: TDF requires monitoring of renal function (eGFR <50 mL/min = switch to AZT). DTG is the preferred INSTI in most settings; use with caution in pregnancy (first trimester) — NACO now permits TLD in pregnancy when benefits outweigh risks.
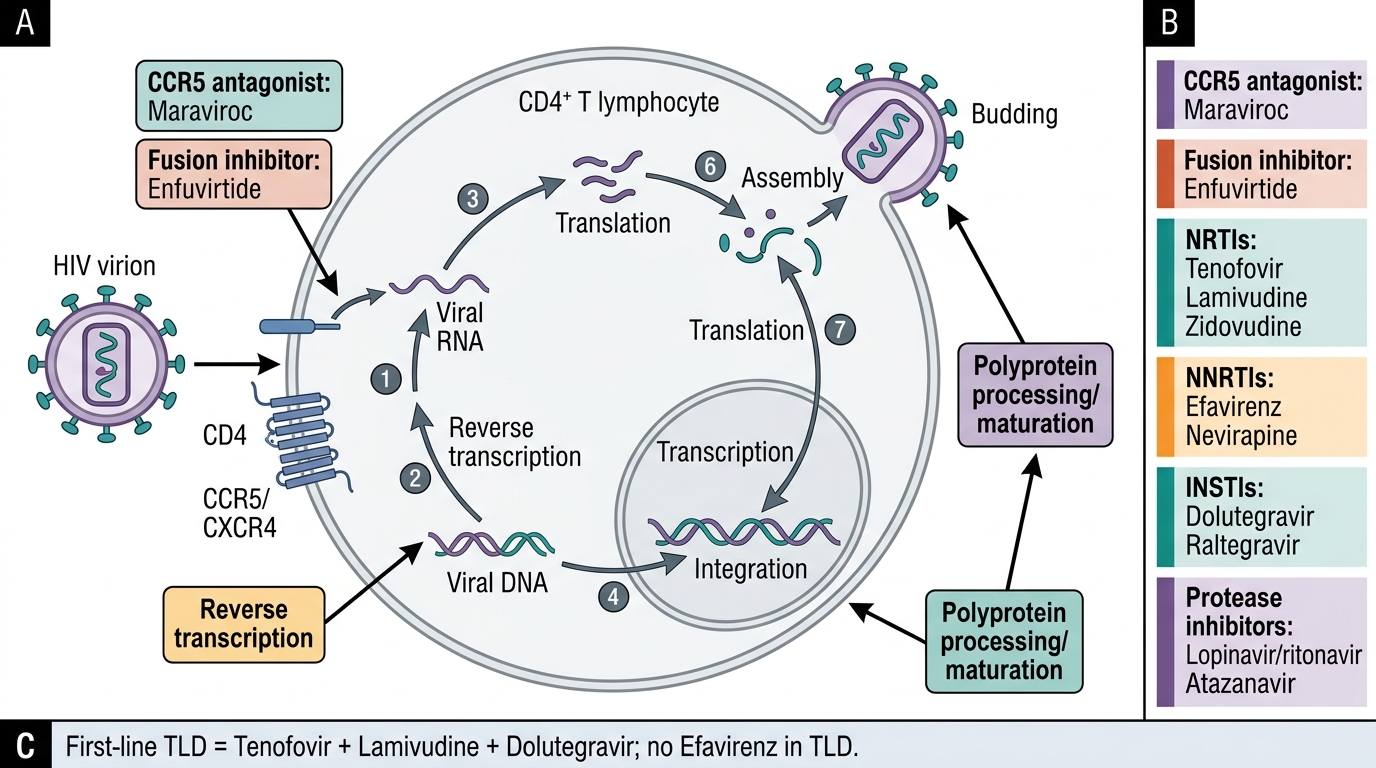
HIV Replication Cycle and Antiretroviral Drug Targets
SELF-CHECK
A 32-year-old HIV-positive woman (CD4 count 240 cells/µL) is started on the NACO first-line regimen TLD (TDF + 3TC + DTG). Two weeks after starting ART, she reports vivid, disturbing dreams and early-morning dizziness. What is the MOST likely cause, and what is the appropriate management?
A. Dolutegravir (DTG) neurotoxicity — switch to lopinavir/ritonavir (LPV/r)
B. This is the efavirenz (EFV)-related CNS side effect in TLD — reassure, take at bedtime, resolves in 4–6 weeks
C. Lamivudine (3TC) hepatotoxicity — check liver function tests urgently
D. The TLD regimen does not contain EFV — these symptoms may represent HIV encephalopathy requiring an MRI
Reveal Answer
Answer: D. The TLD regimen does not contain EFV — these symptoms may represent HIV encephalopathy requiring an MRI
The NACO first-line regimen TLD contains Tenofovir + Lamivudine + Dolutegravir — it does NOT contain efavirenz (EFV). The CNS side effects of vivid dreams and dizziness are characteristic of efavirenz (the prior TLE regimen). Dolutegravir is not known to cause these CNS effects. The correct response is option D: recognise that TLD does not contain EFV, so these CNS symptoms are not an expected side effect of TLD. An alternative explanation (insomnia, psychological adjustment to diagnosis) should be explored; if the symptoms are genuinely distressing and drug-related, clinical review is warranted. This question tests knowledge of the current NACO first-line regimen composition.
Immune Reconstitution Inflammatory Syndrome (IRIS)
Immune reconstitution inflammatory syndrome (IRIS) is a paradoxical clinical deterioration that occurs when a recovering immune system mounts an exaggerated inflammatory response against existing pathogens — either previously treated (paradoxical IRIS) or previously unrecognised (unmasking IRIS). It is a direct consequence of ART restoring immune competence: as CD4 cells recover and pathogen-specific immune responses return, they target residual antigens from OIs with an intensity disproportionate to the clinical benefit, causing tissue inflammation and clinical worsening.
Pathogenesis of IRIS: When ART suppresses viral replication, CD4 counts begin rising within 2–4 weeks. This immune restoration is rapid in the first 3–6 months and initially reflects redistribution of pre-existing memory CD4 cells from lymphoid tissue into the peripheral blood. As these recovering cells encounter residual pathogen antigens (from incompletely treated or subclinical OIs), they mount an inflammatory response characterised by CD4-driven delayed-type hypersensitivity, cytokine release, and tissue oedema. The key features of IRIS that distinguish it from OI treatment failure are: onset typically 2–12 weeks after ART initiation (though it can occur later), clinical deterioration despite ART that is virologically effective, and the absence of a new pathogen (paradoxical IRIS) or the unmasking of a previously subclinical infection (unmasking IRIS).
IRIS is most common with:
- TB-IRIS: The most common form. Paradoxical TB-IRIS presents as worsening respiratory symptoms, enlarging lymph nodes, new fever, or worsening infiltrates after starting ART in a TB-treated patient. TB is the most antigenic organism known to trigger IRIS. Unmasking TB-IRIS can present as new TB features in a patient who had subclinical TB when ART was started.
- Cryptococcal IRIS: Paradoxical cryptococcal IRIS after ART initiation in treated cryptococcal meningitis is associated with high mortality. Presents as recurrent meningitis, increased CSF pressure, or new CNS lesions. This is why ART is deferred 4–6 weeks in cryptococcal meningitis — to allow antifungal therapy to reduce the antigen burden before immune restoration begins.
- CMV IRIS: New or worsening CMV retinitis or vitritis after ART initiation in CMV-treated patients.
- MAC IRIS, KS IRIS: Less common but documented.
- Herpes zoster IRIS: A new or unusually severe zoster eruption in the first weeks of ART.
Diagnosis of IRIS: IRIS is a clinical diagnosis based on three criteria: (1) a consistent clinical deterioration pattern (worsening of a known OI or appearance of new inflammatory features); (2) occurring within the expected time window (typically 2–12 weeks after ART start); (3) evidence of an immunological response (rising CD4 count, falling viral load on ART). Importantly, before diagnosing paradoxical IRIS, the clinician must exclude: (a) ART failure (viral load should be falling, CD4 rising); (b) new OI (new pathogen not previously treated); (c) inadequate treatment of the OI (e.g., drug-resistant TB).
Management of IRIS: The cornerstone is to continue ART — ART should almost never be stopped for IRIS, as it would allow viral rebound and further immunosuppression. Management depends on severity:
- Mild-moderate IRIS (worsening lymphadenopathy, fever, local inflammation without organ-threatening complications): Continue ART and OI treatment; NSAIDs for symptom relief.
- Severe IRIS (respiratory failure, CNS IRIS, cryptococcal IRIS, sight-threatening CMV IRIS): Continue ART; add prednisolone 1 mg/kg/day for 4 weeks, then taper. Corticosteroids are highly effective at reducing IRIS-related inflammation; the Prednisone for the Prevention of Paradoxical Tuberculosis–IRIS (PREVENT-IRIS) trial showed corticosteroids reduced the severity and duration of TB-IRIS.
- Cryptococcal IRIS specifically: In addition to continuing antifungals and ART, therapeutic LP to relieve raised intracranial pressure is essential.
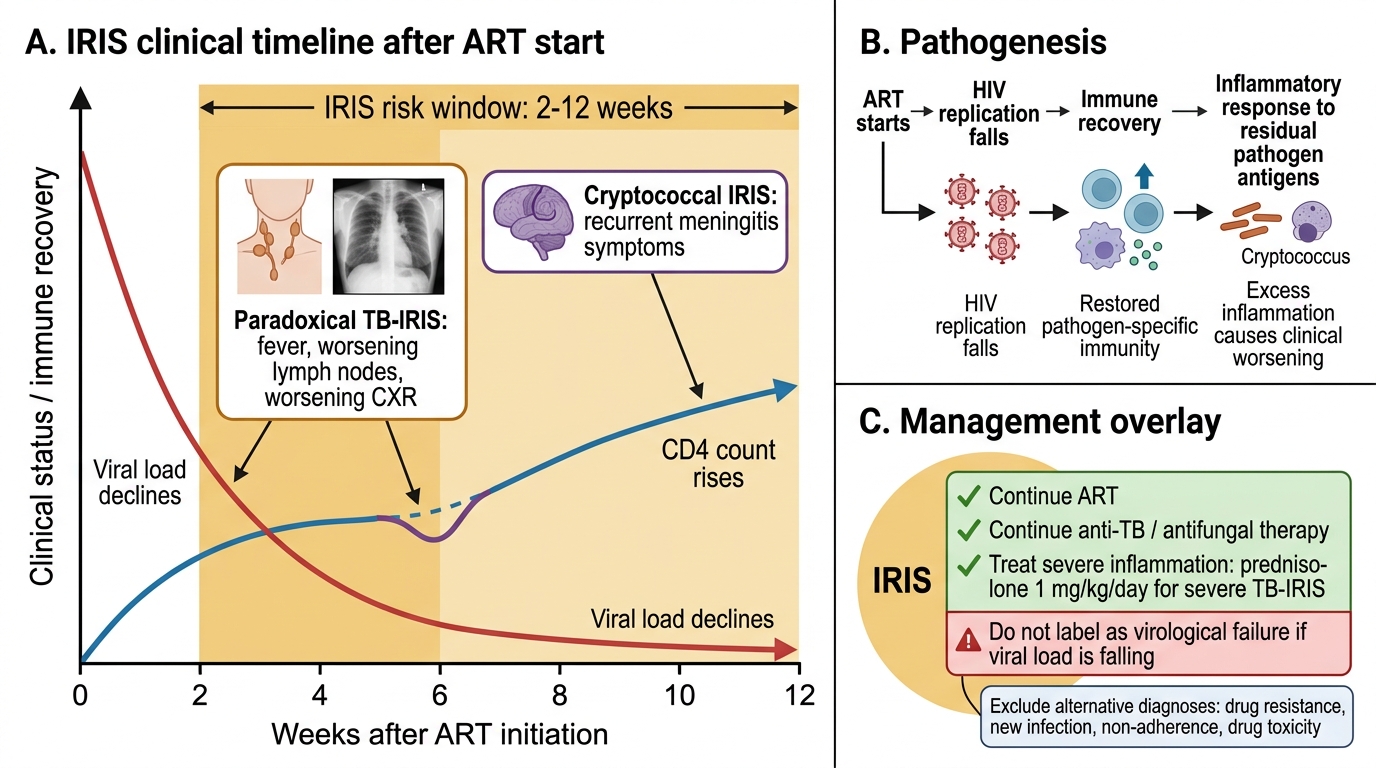
IRIS Pathogenesis and Clinical Timeline After ART
SELF-CHECK
A 38-year-old man with HIV and pulmonary TB started anti-TB treatment 4 weeks ago and ART (TLD) 2 weeks ago. His CD4 count has risen from 95 to 165 cells/µL and his viral load is falling. He now presents with worsening respiratory symptoms, enlarging cervical lymph nodes, and new fever. Chest X-ray shows increasing mediastinal lymphadenopathy. What is the MOST appropriate management?
A. Stop ART immediately — this indicates ART-induced TB drug interaction
B. Switch to second-line ART — this indicates virological failure
C. Continue both ART and anti-TB therapy; add prednisolone 1 mg/kg/day for severe IRIS
D. Stop anti-TB therapy and treat as a new bacterial infection
Reveal Answer
Answer: C. Continue both ART and anti-TB therapy; add prednisolone 1 mg/kg/day for severe IRIS
This is paradoxical TB-IRIS: clinical worsening of TB features (lymphadenopathy, respiratory symptoms, fever) occurring 2–6 weeks after ART initiation, with evidence of virological suppression (falling viral load) and immune recovery (rising CD4 from 95→165). The diagnosis is clinical deterioration in the context of ART-induced immune reconstitution with a known TB infection. Management: CONTINUE BOTH ART and anti-TB therapy (do not stop either). For severe IRIS (worsening CXR + lymphadenopathy + fever), add prednisolone 1 mg/kg/day for 4 weeks. Stopping ART would allow viral rebound. Switching ART is inappropriate when viral load is falling. Anti-TB therapy must continue.