Page 14 of 23
IM7.{14-20,22} | Rheumatologic Disease Management — SDL Guide (Part 2)
Patient Preferences, Follow-Up, Monitoring, and Referral
Effective rheumatologic management extends beyond the initial prescription to encompass three interconnected processes: incorporating patient preferences (IM7.19), establishing a follow-up and monitoring plan (IM7.20), and determining when specialist referral is indicated (IM7.22). These are SH-level competencies requiring communication skill and clinical judgement, not merely factual knowledge. They represent the transition from 'prescribing the right drug' to 'partnering with the patient to achieve the best outcome over a lifelong condition.'
Incorporating patient preferences (IM7.19): Rheumatologic diseases are chronic, and treatment decisions made without patient engagement have a high failure rate due to non-adherence. Shared decision-making in rheumatology addresses the following tension: the clinician knows that early DMARD therapy prevents irreversible damage; the patient knows what they can afford, tolerate, and take reliably. The key areas for preference incorporation are: (1) Route of administration — some patients cannot manage weekly SC injections but can take oral therapy reliably; others prefer the assurance of supervised IV infusions; (2) Side-effect profile — a woman planning pregnancy in the next year cannot take methotrexate (teratogenic); a patient with recurrent chest infections may be reluctant to accept biologics that increase infection risk; (3) Monitoring burden — monthly blood tests for methotrexate monitoring may be a significant economic and logistical barrier for rural patients; (4) Cost — biologics (anti-TNF, IL-6 blockers) cost ₹15,000–₹50,000 per month; a treatment plan that the patient cannot afford is not a plan but an unfulfilled prescription. Explore availability under PMJAY/Ayushman Bharat, hospital formularies, and manufacturer patient support programmes.
When there is a discrepancy between the clinician's preferred treatment and the patient's preference, the discussion must acknowledge the consequences of the alternative — specifically, the risk of irreversible joint damage or organ involvement if effective therapy is delayed — while respecting the patient's autonomy. Document the discussion and the patient's informed choice in the medical record.
Follow-up and monitoring (IM7.20): Every rheumatologic condition requires a disease-specific monitoring plan that covers disease activity assessment, drug toxicity surveillance, complication screening, and immunisation status. The following monitoring principles apply:
- RA on methotrexate: CBC (FBC) and liver function tests at baseline, then every 4–8 weeks for the first 3 months, then every 3 months when stable. Renal function (MTX excreted renally — dose reduction needed in CKD). Clinically: DAS28 score at every visit to assess disease activity and guide treat-to-target decisions.
- SLE: At every visit — BP measurement, urine dipstick (proteinuria screen for active nephritis), CBC (cytopenias), renal function, anti-dsDNA titre + complement C3/C4 (rising titre + falling complement = impending flare). Annual review — DEXA scan (corticosteroid-induced osteoporosis), ophthalmology for HCQ retinopathy (after 5 years), lipid profile (SLE and corticosteroids increase cardiovascular risk).
- Gout on allopurinol: Serum uric acid every 3–6 months until target (<6 mg/dL) is achieved, then annually. Renal function (allopurinol accumulates in CKD — dose adjustments needed). Monitor for allopurinol hypersensitivity syndrome (rare but potentially fatal — fever, rash, hepatitis, eosinophilia — highest risk in HLA-B5801 carriers, more prevalent in Han Chinese and Korean populations; consider HLA-B5801 testing before starting allopurinol in these ethnic groups).
- AS on biologics: CBC, CRP, ALT at baseline and regular intervals. Monitor for infection, including TB reactivation (fever, weight loss, cough).
When to refer to specialist rheumatology (IM7.22): General medicine practitioners should initiate the diagnostic workup and early management but should refer to rheumatology in the following circumstances: (1) Diagnostic uncertainty — suspected SLE with renal involvement, suspected systemic vasculitis, inflammatory arthritis not responding to first-line DMARD; (2) Planned biologic initiation — for TB screening co-ordination, biologic selection, and monitoring protocol; (3) Severe or rapidly progressive RA with DAS28 >5.1 (high disease activity) despite methotrexate; (4) Lupus nephritis (class III/IV on biopsy) — requires nephrology co-management; (5) Complications of treatment — methotrexate-related interstitial lung disease (progressive breathlessness + new bilateral infiltrates), severe cytopenias; (6) Fertility or pregnancy counselling in women with RA or SLE.
⚑ AI image — pending faculty review (auto-QA score 7/10; best of 3 attempts)
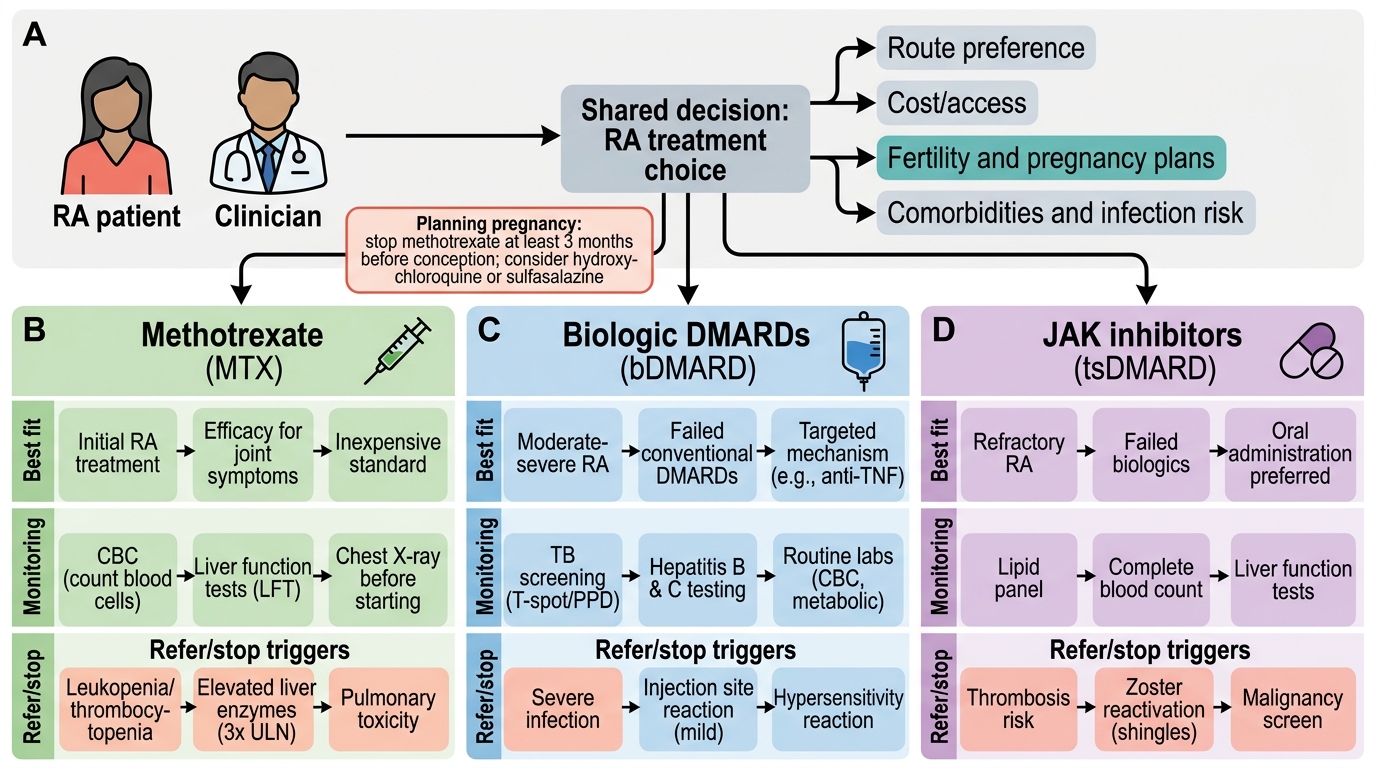
Shared Decision Pathway for RA Treatment
SELF-CHECK
A 30-year-old woman with RA is currently taking methotrexate 15 mg/week. She informs you that she would like to try for a pregnancy in the next 6 months. Which of the following actions is MOST appropriate?
A. Continue methotrexate throughout pregnancy as the benefits outweigh the teratogenic risk
B. Switch to hydroxychloroquine and/or sulfasalazine and discontinue methotrexate at least 3 months before attempting conception
C. Stop methotrexate immediately and start prednisone as the sole therapy
D. Reduce methotrexate dose to 7.5 mg/week to minimise teratogenicity during early pregnancy
Reveal Answer
Answer: B. Switch to hydroxychloroquine and/or sulfasalazine and discontinue methotrexate at least 3 months before attempting conception
Methotrexate is absolutely contraindicated in pregnancy — it is a known human teratogen and abortifacient (it inhibits dihydrofolate reductase, disrupting fetal DNA synthesis and causing neural tube defects, cleft palate, and fetal death). It must be stopped at least 3 months (some guidelines recommend 6 months) before attempting conception. The transition plan for a woman with RA who wishes to conceive should switch to pregnancy-compatible DMARDs: hydroxychloroquine and sulfasalazine are considered relatively safe in pregnancy (compatible with conception and pregnancy, though sulfasalazine should be combined with high-dose folic acid 5 mg/day). Continuing at any dose of MTX in a patient who may become pregnant is not safe. TNF inhibitors (with the exception of certolizumab, which does not cross the placenta significantly) are generally discontinued in the third trimester.
Self-Assessment: Management Decision-Making in Rheumatologic Disease
This self-assessment section integrates the management competencies (IM7.14–IM7.22) into three clinical vignettes that require you to develop, communicate, and monitor a treatment plan while incorporating patient preferences. For each case, identify the diagnosis, propose the appropriate treatment plan with specific drugs and doses, outline the monitoring schedule, flag the relevant patient preference considerations, and state when you would refer. These are SH-level competencies — practice constructing the answer as you would present it in a supervised ward round or clinic consultation.
Case A — Early seropositive RA, disease-modifying therapy initiation:
A 35-year-old woman presents with 4 months of bilateral MCP and wrist joint swelling, morning stiffness 90 minutes, DAS28 = 4.8 (moderate disease activity), anti-CCP positive at 5× ULN, ESR 72 mm/h, CRP 48 mg/L, CBC and liver function normal. X-rays show periarticular osteopenia but no erosions yet. She is a nurse and has googled 'methotrexate side effects' and is concerned.
- Treatment plan: Initiate methotrexate 7.5 mg/week orally, escalating to 15–20 mg/week over 6–8 weeks if tolerated. Prescribe folic acid 5 mg once weekly on a different day from MTX. Short-course bridging prednisolone 10 mg/day tapering over 8–10 weeks to suppress active inflammation while MTX takes effect (MTX has a delayed onset of 6–12 weeks). Review at 6 weeks with CBC and LFT.
- Communication: Explain the treat-to-target strategy — the goal is DAS28 <2.6. Use the 'window of opportunity' concept: 'The first 6–12 months of RA is when we can most effectively prevent joint damage — the medicines are not as scary as they seem online; we will monitor you carefully.' Address her specific concern about fertility if she raises it (advise reliable contraception on methotrexate).
- Monitoring: DAS28 at every visit. CBC + LFT every 6–8 weeks for the first 3 months, then every 3 months. Refer to rheumatology if DAS28 remains >3.2 at 6 months despite maximum-tolerated MTX dose.
Case B — Acute gout with CKD, prescribing challenge:
A 68-year-old man with CKD stage 3 (eGFR 32 mL/min) presents with an acute gout attack in the right first MTP joint. He is on hydrochlorothiazide for hypertension. He has had 4 attacks in the past year.
- Acute treatment: Avoid NSAIDs in CKD stage 3 (risk of further renal impairment). Use colchicine with caution — dose-reduce to 0.5 mg once or twice daily (NOT standard doses, as colchicine accumulates in renal failure and causes neuromyopathy). Prednisolone 30 mg/day tapering over 5 days is the safest option in this patient with CKD.
- Prevention: Switch hydrochlorothiazide to an alternative antihypertensive (e.g., amlodipine — calcium channel blockers are uricosuric and do not raise uric acid; losartan also mildly lowers uric acid). Start allopurinol at low dose (50 mg/day in CKD stage 3, titrate cautiously) 2–4 weeks after the acute attack resolves, with prophylactic colchicine 0.5 mg/day. Target uric acid <6 mg/dL. Avoid febuxostat in CKD stage 4–5.
- Patient preference: Dietary advice (reduce alcohol, organ meats, shellfish); counsel that medication is still needed even with dietary modification in most patients with recurrent gout and CKD.
Case C — SLE with suspected lupus nephritis, communication and referral:
A 27-year-old woman with known SLE (on hydroxychloroquine 200 mg/day) presents with a 3-week history of increasing ankle oedema and frothy urine. BP 148/92 mmHg. Urine dipstick: 3+ protein, 2+ blood. Serum creatinine 118 μmol/L (baseline 72). Anti-dsDNA is elevated from last result. C3 is low.
- Immediate management: Admit for urgent evaluation. Urinalysis with microscopy (look for red cell casts confirming active nephritis). 24-hour urine protein or spot PCR ratio. Renal biopsy to classify the nephritis (WHO class III/IV = proliferative → high-dose induction therapy; class V = membranous → different approach).
- Communication: 'Your lupus appears to be affecting your kidneys — this is a serious but treatable complication. We need to admit you today to confirm the extent and start treatment promptly. The treatment involves strong anti-inflammatory medicines, but we will monitor you very carefully throughout.'
- Referral: Urgent dual referral to rheumatology and nephrology. Start high-dose prednisolone (1 mg/kg/day) while awaiting biopsy result if clinically active nephritis is confirmed by urinalysis.
⚑ AI image — pending faculty review (auto-QA score 7/10; best of 3 attempts)
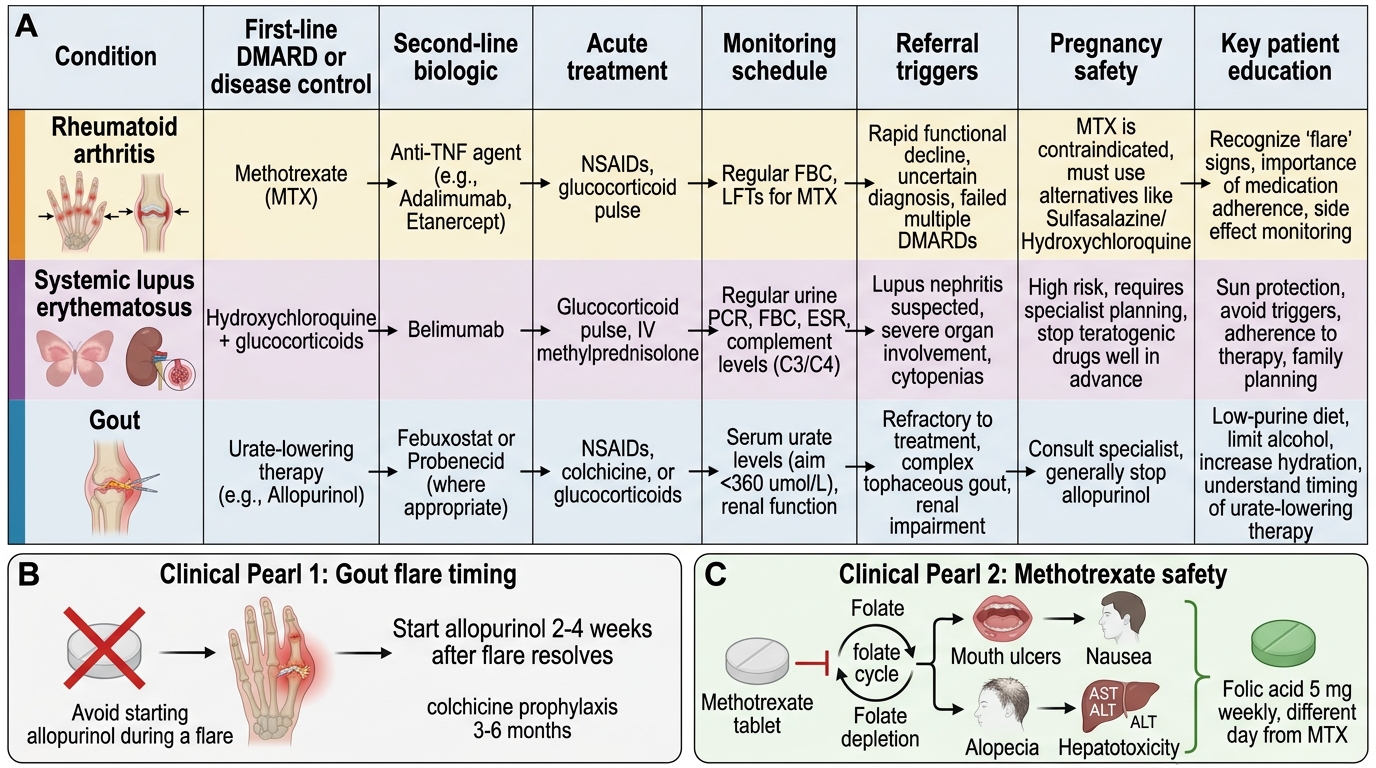
Management Summary of Major Rheumatologic Conditions
CLINICAL PEARL
Two of the most common and consequential prescribing errors in rheumatologic management:
- Starting allopurinol during an acute gout attack. Initiating urate-lowering therapy during an acute gout attack mobilises urate crystals as serum urate levels fall rapidly, triggering further shedding of crystals into the joint space and prolonging or worsening the attack. Always wait 2–4 weeks until the acute attack has fully resolved before starting allopurinol. When starting ULT, always co-prescribe prophylactic colchicine 0.5 mg twice daily for the first 3–6 months to suppress mobilisation flares.
- Failing to prescribe folic acid with methotrexate. Methotrexate inhibits dihydrofolate reductase and depletes folate-dependent pathways. Without supplemental folic acid, patients experience dose-limiting mucositis (mouth ulcers), nausea, alopecia, and hepatotoxicity that lead to discontinuation of an otherwise highly effective DMARD. Folic acid 5 mg once weekly (on a different day from the MTX dose) reduces these side effects by 79% without reducing the anti-inflammatory efficacy of methotrexate. Always prescribe it — the omission of folic acid when prescribing methotrexate is a medication safety error.