Page 17 of 23
IM7.21 | Rheumatologic Disease Quality of Life — SDL Guide (Part 2)
Interpreting QoL Findings and Their Impact on Work, Well-Being, and Family
The clinical interpretation of quality of life findings in rheumatologic disease requires the clinician to translate PROM scores and patient narratives into actionable clinical decisions. This interpretive process addresses four specific domains of impact that are explicitly named in competency IM7.21: quality of life, well-being, work, and family. Each domain has its own trajectory in rheumatologic disease and its own set of targeted interventions when impaired.
Quality of life interpretation: A change in HAQ-DI of ≥0.22 (the minimum clinically important difference, MCID) from the previous assessment indicates a meaningful change in functional status. A HAQ-DI ≥1.0 flags significant disability. A rising HAQ-DI in a patient with stable or improving DAS28 suggests that factors beyond disease activity are driving disability — commonly: central sensitisation, depression, deconditioning, poorly fitted assistive devices, or unmet social care needs. These require assessment beyond the standard clinical review. The SF-36 Physical Component Summary (PCS) and PROMIS Physical Function scores provide context for how the patient's functioning compares with age-matched population norms — a 35-year-old woman scoring 2 standard deviations below the age norm on the SF-36 PCS despite clinical remission warrants investigation of contributing factors.
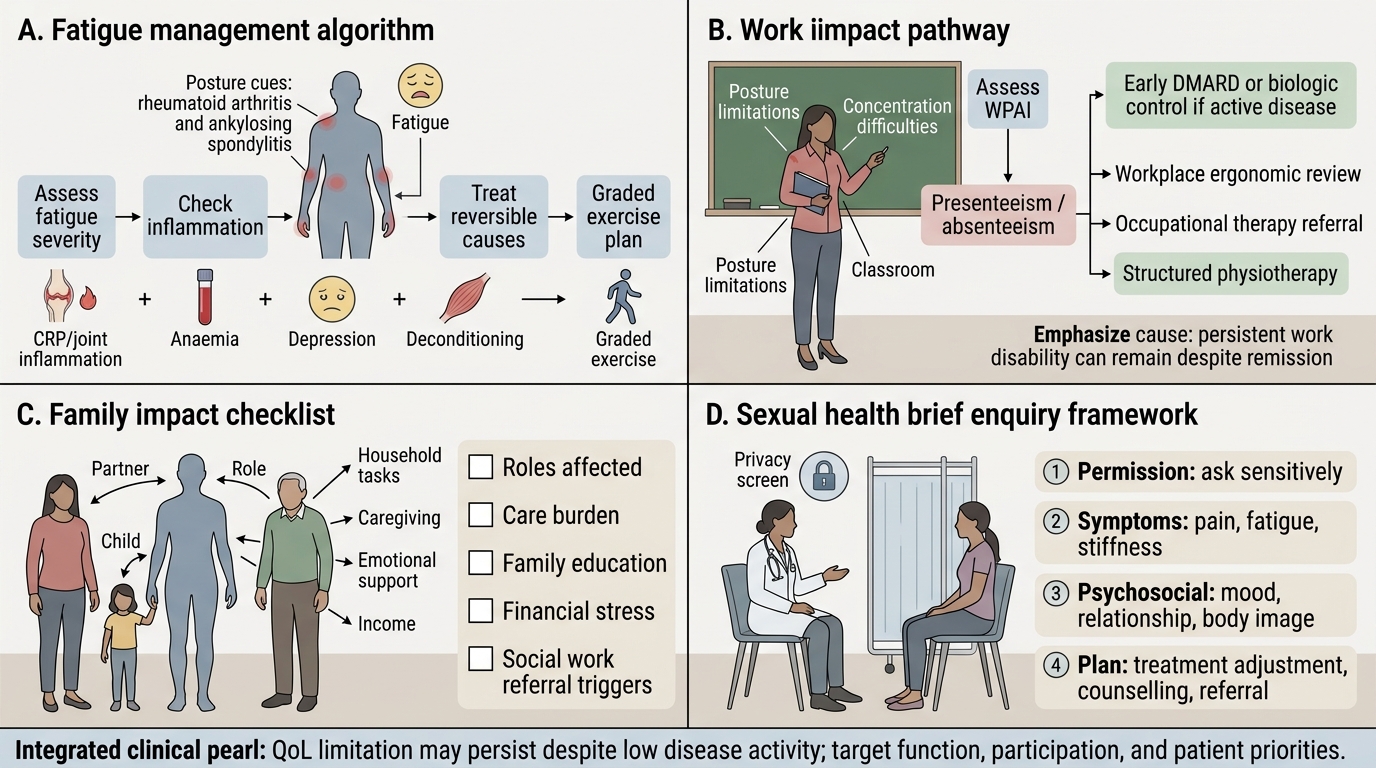
Well-being interpretation: Fatigue is reported by 70–80% of RA patients and 80–90% of SLE patients as one of their most disabling symptoms. FACIT-Fatigue ≤30 indicates clinically significant fatigue. The mechanism of fatigue in rheumatologic disease is multifactorial — active inflammation (cytokines IL-1, IL-6, TNF drive central fatigue), anaemia, sleep disturbance (from pain or from direct CNS manifestations in SLE), depression, and physical deconditioning all contribute. Management is therefore multimodal: treat active inflammation; correct anaemia; screen for and treat depression; prescribe graded aerobic exercise (counter-intuitively, exercise — not rest — is the most evidence-based intervention for inflammatory arthritis fatigue); refer to a psychologist for CBT where fatigue cognitions (catastrophising, activity avoidance) contribute.
Work impact interpretation: A WPAI-RA presenteeism subscale score ≥40% (i.e., 40% of work productivity lost while at work) or absenteeism >20% (days absent from work due to RA in the past 7 days) indicates significant occupational impairment. Work disability in rheumatic disease is not inevitable — vocational assessment and targeted workplace adjustments can preserve employment in the majority of patients who receive timely intervention. The following factors protect work participation and should be addressed proactively: (1) early DMARD therapy (treat-to-target reduces work disability by ~50% versus delayed treatment); (2) workplace adjustments — ergonomic assessment, reduced hours, modified duties, remote working options where available; (3) orthotics and assistive devices — wrist splints in RA reduce pain during work activities; (4) referral to occupational therapist for joint protection advice and adaptive equipment; (5) liaison with employers and disability benefits advisors where needed. Under India's Rights of Persons with Disabilities Act 2016 (RPwD Act), RA, SLE, and ankylosing spondylitis are classified as disabilities when they meet severity criteria — patients may be entitled to employment accommodations and benefit schemes.
Family impact interpretation: In the Indian family context, rheumatologic disease disrupts defined gender and household roles — women with RA and SLE frequently experience guilt, shame, and family tension around their inability to perform domestic duties; men with ankylosing spondylitis may be seen as failing their breadwinner role when work capacity declines. A brief structured assessment of family impact should include: 'Has your arthritis changed how much you can contribute to your household? Has this caused any tension with family members? Do you feel your family understands your condition?' A positive response warrants family education (explaining the disease, its management, and that fatigue and pain are not signs of laziness) and, in cases of significant conflict, referral to a medical social worker or rheumatology patient support group.
Sexual health interpretation: Sexual dysfunction — reduced libido, pain during intercourse (hip and spine limitation in AS; hand and wrist pain in RA), body image concerns (skin rashes, weight gain from corticosteroids, joint deformities) — affects 50–70% of patients with RA or SLE in studies, yet is discussed in fewer than 15% of clinic consultations. A non-judgemental brief enquiry ('Many patients with arthritis find that it affects their intimate relationships — is this something you would like to discuss?') opens the conversation without assuming. Management includes DMARD optimisation (reducing pain and fatigue), referral to a psychosexual therapist where indicated, and positional advice from the physiotherapist.
Quality-of-Life Interpretation in Rheumatologic Disease
SELF-CHECK
A 42-year-old male teacher with ankylosing spondylitis is in clinical remission on a TNF inhibitor (BASDAI score 1.8). However, he scores 45% on the WPAI presenteeism subscale — he says he is present at work but is unable to concentrate or stand for extended periods. Which intervention is MOST likely to reduce his work disability?
A. Increase the TNF inhibitor dose as the BASDAI remission is not complete
B. Prescribe prednisolone 10 mg/day to further suppress residual inflammation
C. Refer for occupational therapy assessment, workplace ergonomic review, and structured physiotherapy focusing on posture and endurance
D. Recommend sick leave until the BASDAI score reaches zero
Reveal Answer
Answer: C. Refer for occupational therapy assessment, workplace ergonomic review, and structured physiotherapy focusing on posture and endurance
This patient is already in clinical remission on biologic therapy (BASDAI 1.8 = well below the 4.0 threshold for high disease activity in AS). His work disability is not being driven by poorly controlled inflammation — it is being driven by functional impairment (postural fatigue from reduced spinal mobility, reduced endurance) that responds to rehabilitative rather than pharmacological escalation. Referral for occupational therapy (joint protection, workplace adaptation) and physiotherapy (targeted postural exercises, spinal mobility, cardiovascular conditioning) are the appropriate interventions. Increasing biologic dose or adding steroids to a patient in remission is not indicated. Sick leave without rehabilitation is counter-productive — it accelerates deconditioning and reinforces avoidance behaviour.
Applied Practice: Demonstrating QoL Understanding in a Clinical Encounter
Demonstrating an understanding of rheumatologic QoL impact in a supervised clinical encounter (as required by the SH-level IM7.21 competency) involves five practical skills: (1) initiating a QoL conversation without waiting for the patient to raise it, (2) administering and interpreting a PROM in context, (3) integrating the QoL findings with the clinical assessment to generate a holistic management plan, (4) making appropriate multidisciplinary referrals, and (5) documenting the QoL assessment and plan in the clinical record. These are skills that can only be developed through supervised practice but can be prepared through structured knowledge of what to ask, when to refer, and how to document.
Provided image
Initiating the QoL conversation: A simple structured opening integrates QoL into the standard clinic encounter: 'Before we look at your blood results, can we check in on a few things that often matter as much as the test results? How has your arthritis been affecting your day-to-day activities? Your sleep? Your work? How have you been feeling in yourself?' This three-part question (function, sleep, mood) is a non-stigmatising opening that covers the three most impactful QoL domains in inflammatory arthritis. It signals to the patient that the clinician is interested in their whole life experience, not just their synovial fluid.
Multidisciplinary referral for QoL management: The following referral thresholds apply:
- Physiotherapist: HAQ ≥1.0 or report of significant exercise avoidance or deconditioning — for graded aerobic exercise programme, joint mobilisation, and postural advice
- Occupational therapist: HAQ ≥1.0 with work impact or difficulty with self-care activities — for joint protection programme, adaptive equipment (jar openers, pen grips, large-handled cutlery), workplace ergonomic assessment, driving assessment if needed
- Psychologist/psychiatry: PHQ-9 ≥10 or GAD-7 ≥10 or significant pain catastrophising — for CBT (most evidence-based psychological intervention in chronic pain), or antidepressant therapy (duloxetine has a dual indication for chronic pain and depression; SNRIs preferred over tricyclics in this context)
- Medical social worker: Significant financial burden (unable to afford medications or monitoring), work disability, carer stress — for benefits navigation, PMJAY/Ayushman Bharat access, community support
- Rheumatology nurse specialist/patient educator: Newly diagnosed patients — for disease education, medication counselling, monitoring instruction, and signposting to patient support groups (Indian Rheumatology Association patient information resources, Arthritis Foundation India)
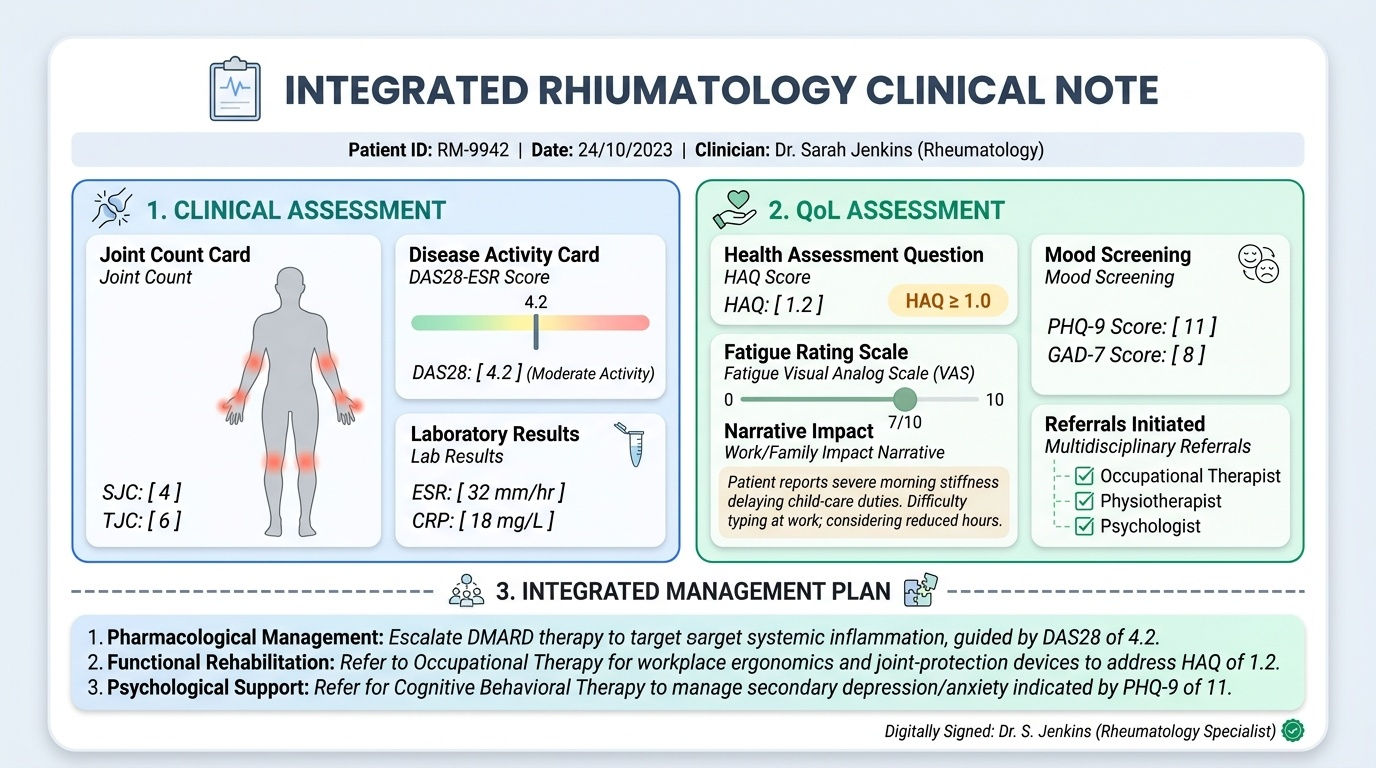
Documentation of QoL assessment: Every clinic encounter for a patient with a chronic rheumatologic condition should include a structured note covering: DAS28 (or equivalent disease activity score), HAQ-DI score, PHQ-9 score (if depression screening indicated), brief record of work and family impact ('Patient reports no change in work capacity; states family is supportive'), and any referrals made. This structured documentation enables serial comparison at subsequent visits — a rising HAQ despite stable DAS28 should trigger a management review.
SELF-CHECK
A 36-year-old woman with SLE reports persistent fatigue despite well-controlled serological disease (normal anti-dsDNA, normal complement, ESR 14 mm/h, no proteinuria). Her FACIT-Fatigue score is 22 (out of 52, where lower scores indicate more fatigue). Her PHQ-9 is 14. Which of the following best explains her fatigue and guides the management?
A. Her SLE is more active than the laboratory tests suggest — escalate immunosuppression
B. Her fatigue is psychological and does not require specific intervention
C. Multifactorial fatigue in serologically quiescent SLE — depression (PHQ-9 14) requires management; graded aerobic exercise and CBT are also indicated
D. Fatigue in SLE is irreversible — manage with rest and activity limitation
Reveal Answer
Answer: C. Multifactorial fatigue in serologically quiescent SLE — depression (PHQ-9 14) requires management; graded aerobic exercise and CBT are also indicated
Fatigue in SLE (and RA) is frequently multifactorial even when serological markers are quiescent. In this patient, the PHQ-9 of 14 indicates moderate depression, which is a major driver of fatigue independent of disease activity. CBT is the most evidence-based psychological intervention for fatigue and depression in chronic inflammatory disease. Graded aerobic exercise (not rest — exercise paradoxically reduces inflammatory arthritis fatigue) should be prescribed. The FACIT-Fatigue score of 22 (below the 30 threshold for clinically significant fatigue) confirms the severity. Escalating immunosuppression without evidence of active SLE (normal serology, normal urine, normal complement) is not indicated and exposes the patient to unnecessary drug toxicity. Fatigue in SLE is not irreversible — it responds to multimodal management targeting inflammation, anaemia, sleep, mood, and deconditioning.
Self-Assessment: Applying QoL Understanding in Rheumatologic Practice
This self-assessment section tests your ability to apply QoL principles to clinical scenarios — identifying the relevant QoL domains affected, selecting the appropriate PROM, interpreting the results, and generating a holistic management plan that extends beyond pharmacological disease control. For each case, work through the QoL assessment before reading the analysis. The IM7.21 competency at the SH level requires you to demonstrate this integration in a supervised patient encounter — the self-assessment cases prepare you for that demonstration.
Self-Assessment A: A 28-year-old male software engineer with newly diagnosed ankylosing spondylitis (BASDAI 4.2 on NSAIDs) attends his second clinic visit. He is taking his naproxen regularly and reports some improvement in morning stiffness (now 45 minutes, down from 90). However, he mentions in passing that he has 'been missing a lot of deadlines at work' and 'feels down most of the time.' His wife is pregnant and he is worried about whether he will be able to care for the baby with his limited spine mobility.
- QoL domains to assess: Work impact (WPAI), psychological well-being (PHQ-9 and GAD-7), family/role anticipation, and fatigue.
- PROM to administer: PHQ-9 (screening for depression — 'feeling down most of the time' is a positive screen), GAD-7 (anxiety about parenting), WPAI-AS (work productivity), BASDAI for disease activity.
- Management plan: If PHQ-9 ≥10, initiate psychological support referral (CBT); if GAD-7 ≥10, address anxieties specifically around parenting and demonstrate joint protection strategies for baby care. Refer to physiotherapy for spinal mobility and postural exercises that will enable safe baby-lifting technique. Review NSAID adequacy — if BASDAI >4.0 at 3-month review, initiate biologic. Provide written information about AS and parenting from Arthritis Foundation resources.
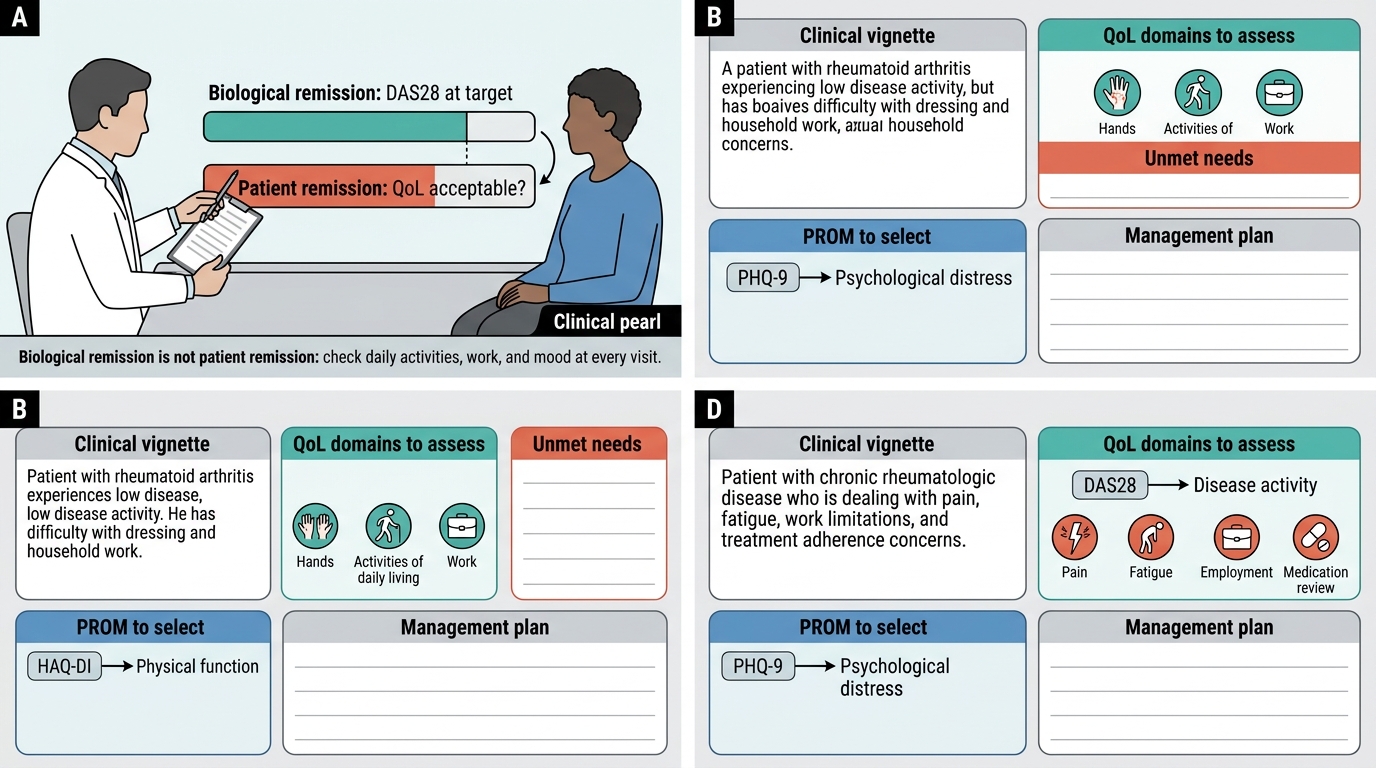
Self-Assessment B: A 44-year-old woman with RA has been on methotrexate 20 mg/week for 3 years. Her DAS28 is 2.3 (remission). She hands you a completed HAQ-DI during the clinic visit — her score is 1.8. She has left her job as a teacher because she can no longer write on the blackboard for more than 20 minutes without severe hand pain. She lives alone.
- Interpretation: This is the 'biological remission ≠ patient remission' scenario. HAQ 1.8 in the presence of DAS28 remission suggests that pain and functional impairment are not fully explained by active inflammation — central sensitisation, psychological factors, or deconditioning may be contributing.
- Management plan: Administer PHQ-9 (screen for depression, which may be amplifying the pain and disability). Refer to occupational therapist for pen/grip adaptations and ergonomic assessment for classroom work. Refer to physiotherapist for hand exercise programme. Assess for central sensitisation (widespread pain, poor sleep, multiple tender points beyond the joints — fibromyalgia overlap is common in RA). If PHQ-9 ≥10, refer to psychology for CBT. If she meets the criteria, advise about RPwD Act 2016 disability accommodation rights and employment support. Explore whether returning to work with reasonable adjustments is feasible.
Self-Assessment C: A 32-year-old woman with SLE has had stable disease for 18 months on hydroxychloroquine 200 mg/day. At today's visit, she mentions — somewhat hesitantly after you ask directly — that her relationship with her partner has been very strained because they have not had sex for over a year. She says she is 'too tired and it hurts.' She is embarrassed to discuss it further.
- QoL domain: Sexual health — a domain documented to be affected in 50–70% of SLE patients but discussed in fewer than 15% of encounters.
- Opening technique: 'Thank you for telling me — this is actually very common in lupus, and I'm glad you mentioned it. Can you tell me more about what makes it uncomfortable — is it the joint pain, or the fatigue, or something else?' This normalising, non-judgemental response opens a structured assessment.
- Management plan: Assess pain location (hip, sacroiliac involvement? Vulvar dryness from hydroxychloroquine or vaginal SLE involvement?). Address fatigue (PHQ-9, FACIT-Fatigue). If fatigue is driving the problem, treat the depression if present and prescribe graded exercise. If pain is the primary issue, physiotherapy (hip and lumbar mobility, positional advice). Refer to psychosexual therapy if the couple relationship requires a specialist intervention. Provide information about SLE and intimate relationships from Lupus UK/LUPUS India resources.
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
Rheumatology QoL Case Card Worksheet
CLINICAL PEARL
The most important clinical pearl for rheumatologic quality of life practice is: biological remission is not patient remission. A DAS28 in the target range does not mean the patient's quality of life is acceptable. Every clinic encounter for a patient with chronic rheumatologic disease should include a brief structured QoL check — at minimum: 'How has your arthritis been affecting your daily activities, your work, and your mood?' The HAQ-DI and PHQ-9 are the two highest-yield, shortest-to-administer PROMs that together capture the physical function and psychological dimensions most likely to be impaired beyond what disease activity scores detect. A patient who is in remission by DAS28 but has a PHQ-9 ≥10 and an HAQ ≥1.0 needs more intervention — the treatment plan is incomplete until these are addressed. Documenting QoL at every visit also creates the longitudinal record that allows the clinician to detect a deteriorating trajectory before a crisis occurs.