Page 5 of 19
IM9.3-5 | Anaemia Clinical Evaluation — SDL Guide
Learning Objectives
- Elicit, document, and present a structured anaemia history covering all seven domains: symptoms, dietary history, GI bleeding, menstrual/obstetric history, medications and family history, occupational/travel history, and systems review
- Perform a systematic physical examination for anaemia: assess pallor at four sites, identify the hyperdynamic circulation signs, and recognise aetiology-specific signs (koilonychia, glossitis, jaundice, splenomegaly, neurological signs)
- Construct a prioritised differential diagnosis from the history and examination, ranked by probability with mandatory safety-netting of dangerous diagnoses
- Identify the indications for specialist referral in a patient presenting with anaemia
INSTRUCTIONS
This module focuses on the clinical skills of anaemia evaluation: structured history-taking across seven high-yield domains, systematic physical examination with recognition of aetiology-specific signs, and construction of a prioritised differential diagnosis. These are SH (Skill and History) competencies — you must demonstrate them in practice, not merely describe them. Work through each case scenario actively before reading the analysis.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 91 — Clinical Approach to Anaemia (textbook)
- API Textbook of Medicine, 10th ed., Section on Haematology — History and Examination (textbook)
- Davidson's Principles and Practice of Medicine, 23rd ed., Ch. 25 — Clinical Approach to Anaemia (textbook)
- NMC Competency-Based Curriculum for MBBS 2024 — IM9.3, IM9.4, IM9.5 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are seeing Meena, a 30-year-old housewife from a village in Bihar. She has been brought to the medicine OPD by her husband after she fainted while drawing water from the well. She says she has been tired for 'many months' and climbs stairs 'with difficulty'. She appears thin, her sclera are yellowish-pale, and her lips look washed out. Her pulse is 108/min and her palms are pale. In the next cubicle, your senior colleague is examining Ramesh, a 52-year-old government officer who presents with 3 weeks of progressive fatigue and two episodes of black tarry stools. His haemoglobin at a private lab yesterday was 7.4 g/dL. Both patients are anaemic — but the history they will give you, the examination findings you will uncover, and the differential diagnosis you will build are entirely different. The clinical evaluation of anaemia is a structured, purposeful exercise: eliciting a focused history that screens for cause, performing a systematic examination that quantifies severity and detects aetiology-specific signs, and then constructing a prioritised differential diagnosis from the clinical evidence. This module builds exactly those skills.
WHY THIS MATTERS
The NMC competencies IM9.3 (medical history), IM9.4 (systematic examination), and IM9.5 (differential diagnosis) are Skill and History (SH) competencies — meaning you are expected to demonstrate these skills in supervised clinical practice, not merely describe them. In the Indian context, history-taking for anaemia carries special weight because many patients present late (after months of symptoms), have multiple concurrent risk factors (dietary, obstetric, infective), belong to high-risk groups (women of reproductive age, children, tribal communities with haemoglobinopathies), and may have limited health literacy requiring clear, non-technical communication. The clinical evaluation is also the most resource-efficient step: a well-taken history narrows the differential diagnosis before any investigation is ordered, reducing unnecessary tests and focusing resources on the most likely cause.
RECALL
Before applying these skills, recall the major anaemia categories from the foundations module. Anaemia is classified morphologically by MCV (microcytic <80 fL, normocytic 80–100 fL, macrocytic >100 fL) and kinetically by reticulocyte index (hyperproliferative >2.5 = haemolysis/bleeding; hypoproliferative <2.0 = deficiency/marrow failure). Each category has a characteristic clinical story: microcytic hypochromic = iron deficiency (dietary, bleeding, malabsorption) or thalassaemia (ethnic background, family history); macrocytic = B12 or folate deficiency (vegetarian diet, pregnancy, alcohol, drugs) or liver disease/hypothyroidism; normocytic = chronic disease, haemolysis, acute blood loss, renal failure. These patterns anchor the clinical history: the history should actively seek evidence supporting or refuting each major category in this differential.
Clinical Indication: When to Evaluate for Anaemia
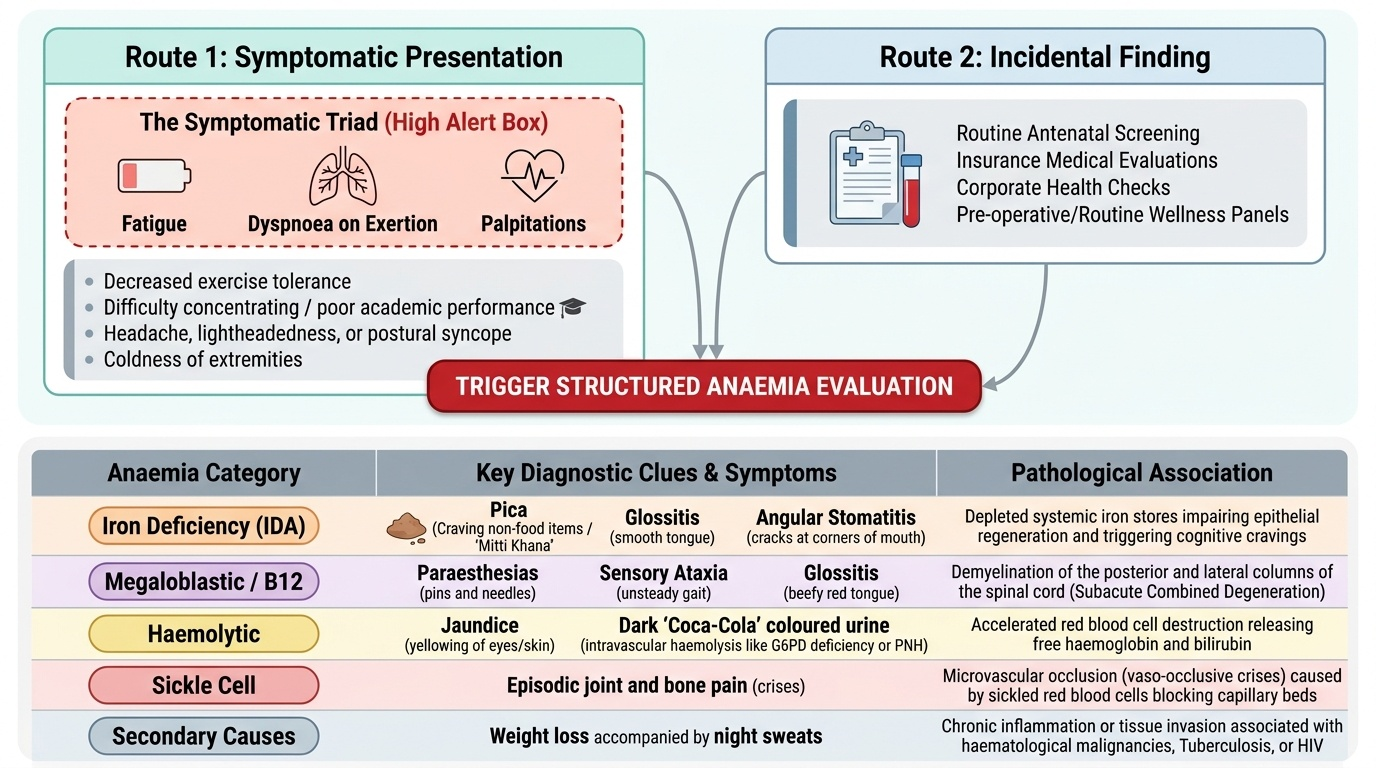
The clinical indication for a structured anaemia evaluation arises from two routes: a symptomatic presentation or an incidental laboratory finding. Understanding both presentations is essential because the threshold for symptoms depends on the rate of onset, severity, age, cardiovascular reserve, and the patient's own perception and health-seeking behaviour — factors that vary enormously in the Indian clinical context.
Provided image
The symptomatic triad of anaemia comprises fatigue (the most universal and earliest symptom — present even in mild anaemia, reflecting reduced oxygen delivery to muscles and brain), dyspnoea on exertion (reflecting the respiratory compensatory response to hypoxia), and palpitations (reflecting the hyperdynamic circulation — increased cardiac output driven by compensatory mechanisms). These three symptoms together, in a reproductive-age woman or child presenting to a primary health centre or district hospital in India, should immediately trigger a structured anaemia evaluation. Additional presenting symptoms that raise the probability of anaemia include: decreased exercise tolerance, difficulty concentrating and poor academic performance (especially in children), headache, lightheadedness or syncope (particularly postural — from low cardiac output on standing), and coldness of extremities.
Beyond these general symptoms, aetiology-specific symptoms provide the critical clinical clues that direct the differential: pica (craving and eating of non-food substances — clay, mud, soil, chalk, ice — is pathognomonic of iron deficiency and is culturally well-recognised in India as 'mitti khana'), glossitis and angular stomatitis (IDA and B12 deficiency), paraesthesias and sensory ataxia (B12 deficiency — subacute combined degeneration), jaundice (haemolytic anaemia), dark or 'Coca-Cola' coloured urine (intravascular haemolysis — G6PD, PNH), episodic joint and bone pain (sickle cell disease vaso-occlusive crises), and weight loss with night sweats (haematological malignancy, tuberculosis, or HIV-associated anaemia).
The incidental finding route — an unexpected low haemoglobin on a routine blood test — is increasingly common as haemogram testing is incorporated into antenatal screening, insurance medicals, and corporate health checks. Even asymptomatic patients with haemoglobin below the WHO threshold require a full aetiology evaluation, because the absence of symptoms reflects either mild severity, chronic adaptation, or limited insight — not the absence of treatable disease.
Medical History: Eliciting the Structured Anaemia History
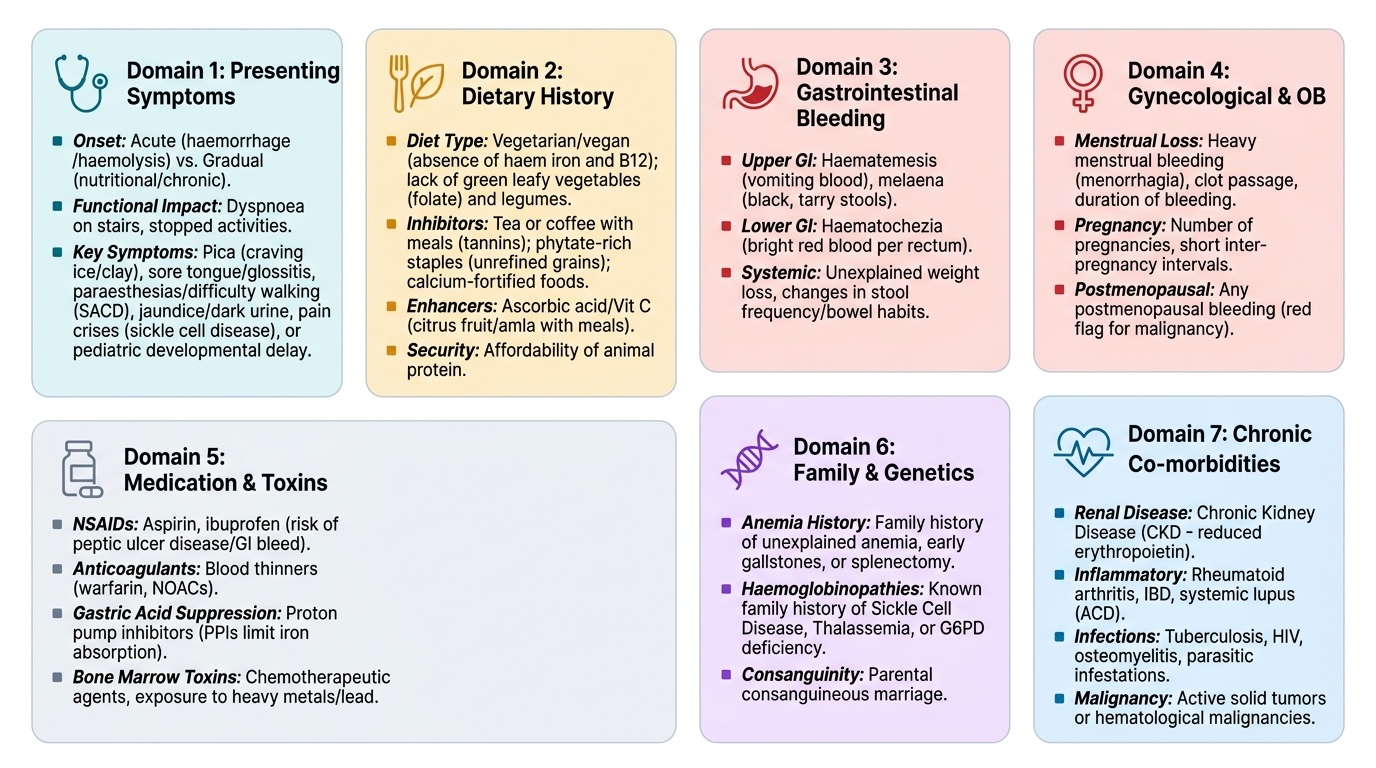
A focused anaemia history is organised into seven domains. Each domain maps directly onto a pathophysiological mechanism or aetiology group, transforming the history from a passive listing of complaints into an active hypothesis-testing exercise.
Provided image
Domain 1 — Presenting symptoms (onset, duration, severity): Establish whether the onset was gradual (chronic anaemia — favours nutritional deficiency, chronic disease, haemoglobinopathy) or acute (favours haemorrhage or acute haemolysis). Quantify functional impact: how many flights of stairs before dyspnoea? Has the patient stopped activities she previously managed? Ask specifically about pica (a reliable indicator of iron deficiency in Indian patients, often not volunteered unless specifically asked), sore tongue or mouth (IDA: glossitis; B12: tender glossitis with a beef-red tongue), paraesthesias in hands or feet (B12 deficiency peripheral neuropathy), difficulty walking or balance problems (B12-related SACD), dark urine or jaundice (haemolysis), and pain crises (sickle cell disease). In children, ask about developmental milestones and school performance.
Domain 2 — Dietary history: This is paramount in India given the high prevalence of nutritional anaemia. Ask about: (a) vegetarian or vegan diet — absence of haem iron (meat, fish) and B12 (animal products exclusively); (b) frequency of green leafy vegetable consumption (folate source) and legumes; (c) tea or coffee consumed with meals (tannins inhibit non-haem iron absorption — a common practice that significantly reduces iron bioavailability); (d) phytate-rich staple diet (unrefined cereal — wheat, rice, millet — contains phytates that chelate iron); (e) calcium-fortified foods consumed with meals (calcium inhibits iron absorption); (f) ascorbic acid (vitamin C) with meals (enhances non-haem iron absorption — eating citrus fruit or amla with iron-rich foods improves bioavailability). Ask about food insecurity and affordability of animal protein.
Domain 3 — Gastrointestinal bleeding history: In any adult, especially males and postmenopausal women, this is the most critical domain for IDA. Ask about: haematemesis (upper GI bleeding), melaena (black tarry stools — altered blood from upper GI), haematochezia (bright red rectal bleeding — lower GI or vigorous upper GI bleed), and change in stool frequency or calibre (colorectal cancer). Ask about heartburn and NSAID use (peptic ulcer disease). Use a direct question: 'Have you noticed any blood in your stools, even just once?'. The patient's perception of 'blood in stools' may be limited; ask about dark black tarry stools as a separate question.
Domain 4 — Menstrual and obstetric history (women of reproductive age): Menorrhagia is the leading cause of IDA in premenopausal women. Quantify menstrual blood loss using the pictorial blood assessment chart (PBAC) conceptually: ask about duration (days), number of pads or cloths per day, and passage of clots. A woman using more than 5 pads per day or passing large clots has heavy menstrual bleeding (HMB). Ask about cycle regularity, dysmenorrhoea, and intermenstrual bleeding. Record all pregnancies (gravidity, parity), number of deliveries within 2 years of each other (short inter-pregnancy interval depletes iron stores), breastfeeding duration, and postpartum haemorrhage (PPH — severe PPH causes Sheehan syndrome affecting the pituitary, not anaemia directly, but anaemia from blood loss). Multiple pregnancies at short intervals is one of the most powerful predictors of IDA in Indian women.
Domain 5 — Prior illness, medications, and family history: Ask about known chronic diseases: tuberculosis (ACD, and anti-TB drugs rarely cause haemolysis), HIV (ACD, opportunistic infections, zidovudine — macrocytic anaemia), chronic kidney disease (erythropoietin deficiency — normocytic hypoproliferative), liver disease (multifactorial), hypothyroidism (macrocytic or normocytic), inflammatory bowel disease (iron malabsorption, ACD, B12 if terminal ileal disease). Drug history is essential: NSAIDs (GI bleeding → IDA), methotrexate/hydroxyurea/trimethoprim (folate antagonism → macrocytosis), proton-pump inhibitors (reduce gastric acidity → impair iron and B12 absorption), phenytoin/phenobarbitone (folate malabsorption), primaquine/dapsone/nitrofurantoin (acute haemolysis in G6PD deficiency). Family history of anaemia, jaundice, splenectomy, or gallstones (jaundice + gallstones in a young person with anaemia = haemolytic anaemia — bilirubin gallstones are common in chronic haemolysis). Ethnic background: thalassaemia (Gujarat, Maharashtra, Tamil Nadu, West Bengal — higher prevalence), sickle cell disease (Chhattisgarh, Odisha, Maharashtra tribal belt), G6PD deficiency (South India, Eastern India, tribal communities).
Domain 6 — Travel and occupational history: Hookworm infestation (Ancylostoma duodenale) is a major cause of IDA in rural India, particularly in agricultural workers who walk barefoot on soil contaminated with faeces (percutaneous penetration). Ask about residence in or travel to endemic areas and the practice of wearing footwear. Also ask about TB exposure (a leading cause of ACD in India), alcohol use (macrocytic anaemia — direct toxic marrow effect + folate deficiency), and occupational chemical exposure (benzene, lead — aplastic anaemia; lead poisoning — sideroblastic microcytic anaemia).
Domain 7 — Systems review: A brief, targeted review: jaundice (haemolysis, liver disease, B12 deficiency), weight loss (malignancy, HIV, TB), recurrent infections (aplastic anaemia — pancytopenia), bleeding from other sites (thrombocytopenia — aplastic anaemia, ITP, DIC), bone pain (multiple myeloma, leukaemia), lymph node enlargement (lymphoma, leukaemia, HIV).
SELF-CHECK
A 28-year-old vegetarian woman from Gujarat presents with fatigue and a sore tongue. She drinks three cups of tea with every meal. Which dietary factor most significantly REDUCES her iron absorption, and what change would most IMPROVE it?
A. Phytates in her vegetable diet reduce absorption; switching to haem iron would improve it
B. Tannins in tea consumed with meals chelate non-haem iron and reduce absorption; consuming tea between rather than with meals would improve iron bioavailability
C. Absence of calcium from her vegetarian diet reduces absorption; adding dairy with meals would help
D. Lack of B12 in her diet impairs iron absorption; B12 supplementation would restore it
Reveal Answer
Answer: B. Tannins in tea consumed with meals chelate non-haem iron and reduce absorption; consuming tea between rather than with meals would improve iron bioavailability
Tannins in tea and coffee form insoluble complexes with non-haem iron in the gut lumen, reducing its absorption by up to 60–75% when consumed with iron-rich meals. This is a major, modifiable cause of iron deficiency in India where tea with every meal is culturally universal. The practical advice: avoid tea and coffee for at least 1 hour before and after meals when trying to maximise iron absorption. Ascorbic acid (vitamin C) from amla, lemon juice, or citrus fruit consumed WITH meals is the most effective single dietary enhancer of non-haem iron absorption. Phytates (in cereals) also inhibit iron absorption, but the question asks specifically about the most significant factor in this patient given her tea-with-every-meal habit. B12 deficiency does not impair iron absorption.
Systematic Physical Examination for Anaemia
The physical examination of a patient with anaemia serves four purposes: (1) confirm and quantify the severity of anaemia through signs of pallor and hyperdynamic circulation; (2) detect aetiology-specific signs that point toward a particular diagnosis; (3) identify signs of the complications of anaemia (high-output cardiac failure, shock); and (4) detect signs of the underlying disease causing anaemia (organomegaly, lymphadenopathy, jaundice, skin changes). A systematic approach ensures no aetiology-specific sign is missed.
General examination:
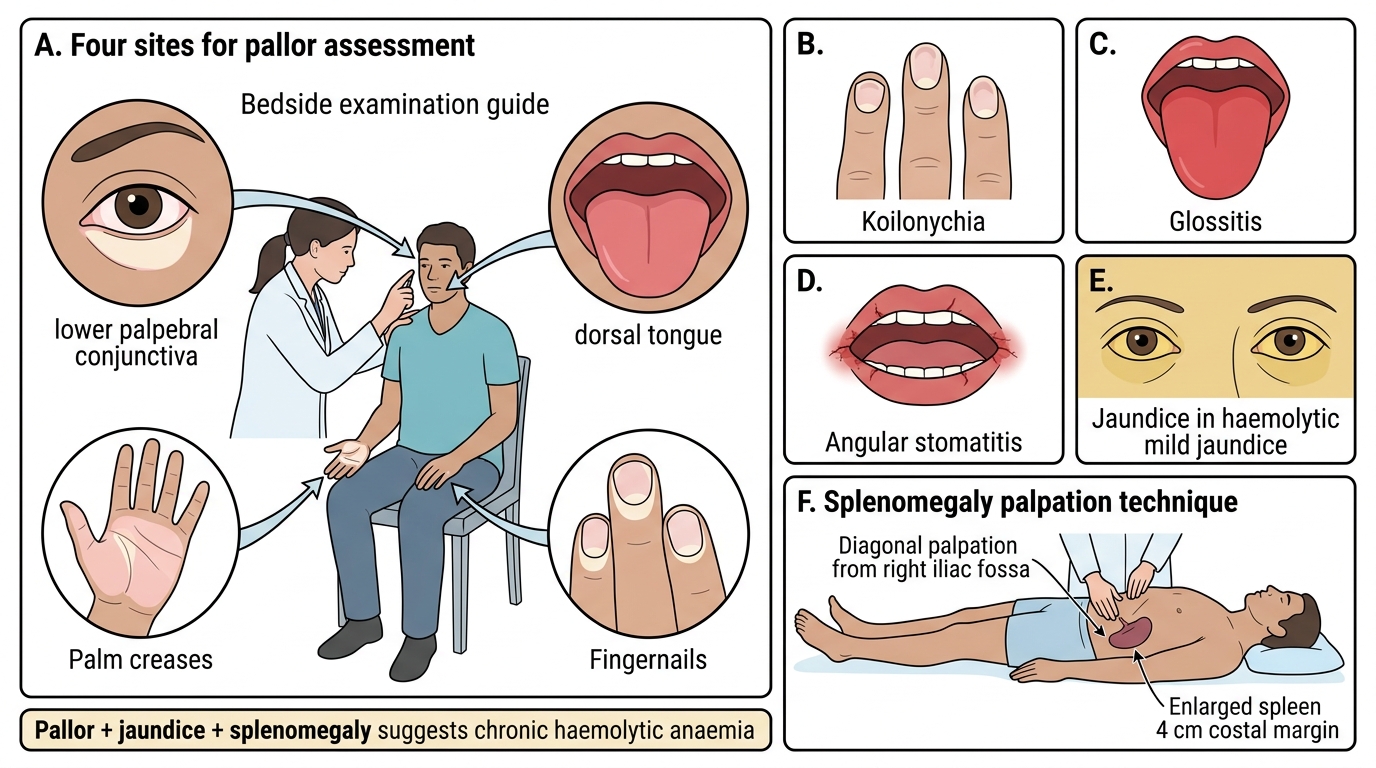
Begin with a general impression: is the patient comfortable at rest, or visibly breathless even lying down? Note nutritional status (body habitus, wasting). Assess the pallor at multiple sites — the standard four examination sites for pallor are: (1) conjunctival pallor — lower eyelid everted, assessed on the palpebral conjunctiva (the most sensitive and reliable sign — pallor of conjunctivae correlates best with haemoglobin level; sensitivity ~90% for Hb <9 g/dL); (2) palmar pallor — skin creases of the palm; (3) tongue — pale or atrophic; and (4) nail beds — pallor with pressure release. Also inspect the buccal mucosa and lips. Remember that pallor alone is not anaemia — it reflects reduced haemoglobin in the peripheral microcirculation and can be confounded by peripheral vasoconstriction, oedema, or dark skin pigmentation. Haemoglobin measurement is essential to confirm.
Assess for jaundice (scleral icterus — yellow colouration of the sclerae, best assessed in natural light): jaundice in the context of anaemia immediately raises the possibility of haemolysis, because haemolysis liberates haem which is catabolised to unconjugated bilirubin. Pallor with jaundice is the haemolytic combination. In contrast, pallor without jaundice favours nutritional deficiency, aplasia, or chronic disease.
Assess body temperature: fever in the context of anaemia suggests infective aetiology (malaria, TB, infective endocarditis — all important in India) or haematological malignancy. Blood pressure and pulse should be recorded: tachycardia is an early compensatory sign; postural hypotension (drop ≥20 mmHg systolic on standing) suggests significant volume depletion (acute blood loss) or severe anaemia with impaired vasomotor compensation.
Specific examination signs by aetiology:
Iron deficiency anaemia:
- Glossitis: smooth, red, atrophic tongue — loss of filiform papillae, giving a characteristic smooth 'bald' appearance; tongue may be tender
- Angular stomatitis (angular cheilitis): cracking and erythema at the corners of the mouth
- Koilonychia (spoon-shaped nails): concave, spoon-shaped deformity of the fingernails, most prominent in the index and ring fingers; a sign of chronic severe IDA
- Pallor without jaundice (unless concurrent haemolysis)
- Pica may be apparent from the history (not a physical sign)
- Plummer-Vinson syndrome (Patterson-Brown-Kelly): dysphagia (from a post-cricoid oesophageal web) + IDA + glossitis — a triad seen in middle-aged women; rare but important because of association with hypopharyngeal carcinoma
B12 and folate deficiency:
- Glossitis: smooth, beef-red tongue (more prominently red than in IDA)
- Angular stomatitis
- Neurological signs (B12 only): dorsal column loss — impaired vibration sense (tuning fork at bony prominences) and impaired joint position sense (proprioception), positive Romberg sign; lateral column involvement — hyperreflexia, upgoing plantar response (extensor plantar); peripheral neuropathy — glove-and-stocking sensory loss, reduced deep tendon reflexes
- Mild jaundice (from intramedullary haemolysis of megaloblasts — 'ineffective erythropoiesis')
- Skin hyperpigmentation (classically on dorsum of hands and face — distinctive of B12 deficiency in darker-skinned patients)
Haemolytic anaemia:
- Pallor + jaundice (the haemolytic combination) — unconjugated hyperbilirubinaemia
- Splenomegaly: the spleen is enlarged in chronic haemolysis (extravascular haemolysis) due to hyperplasia of the macrophage-rich red pulp; hepatomegaly may co-exist in severe cases
- Leg ulcers (over malleoli): characteristic of sickle cell disease and hereditary spherocytosis — caused by vascular occlusion and tissue hypoxia in the skin
- Sickle cell facies: not present in the adult with stable SCD, but bossing of the skull and chipmunk facies are seen in β-thalassaemia major from extramedullary haematopoiesis
- Gallstones on examination: tender right hypochondrium in a young patient with chronic haemolysis (bilirubin gallstones)
- Haemoglobinuria: Coca-Cola coloured urine — ask patient to provide a urine sample and inspect it
Aplastic anaemia / marrow failure:
- Pancytopenia signs: pallor (anaemia) + petechiae and purpura (thrombocytopenia) + recurrent infections (neutropenia)
- Absent organomegaly (contrast with haematological malignancy where splenomegaly and lymphadenopathy are common)
General hyperdynamic circulation signs (in moderate-to-severe anaemia of any cause):
- Tachycardia, bounding pulse, wide pulse pressure
- Apical systolic flow murmur (a soft mid-systolic murmur heard at the apex due to turbulent high-flow-velocity blood through the mitral orifice — not a structural valve lesion; a common and important examination finding in significant anaemia)
- Cardiomegaly in longstanding severe anaemia (high-output cardiac failure)
- Pedal oedema in severe or decompensated anaemia
Clinical Examination Signs in Anaemia
SELF-CHECK
A 22-year-old woman from Tamil Nadu presents with pallor and mild jaundice. She has splenomegaly extending 4 cm below the costal margin. Her haemoglobin is 8.2 g/dL, MCV 68 fL, reticulocyte count 9%, bilirubin 42 µmol/L (predominantly unconjugated), and LDH is elevated. Her family history reveals that her younger brother had a splenectomy for 'blood disease'. Which examination finding MOST directly supports a haemolytic rather than nutritional cause?
A. Conjunctival pallor
B. Koilonychia of the fingernails
C. Pallor combined with jaundice and splenomegaly
D. Angular stomatitis at the corners of the mouth
Reveal Answer
Answer: C. Pallor combined with jaundice and splenomegaly
The triad of pallor + jaundice + splenomegaly is the pathognomonic examination combination of chronic haemolytic anaemia. Pallor reflects reduced haemoglobin; jaundice (scleral icterus) reflects elevated unconjugated bilirubin from haemolysis; splenomegaly reflects hyperplasia of splenic macrophages (red pulp) due to increased red cell destruction. This combination, combined with the elevated reticulocyte count, elevated LDH, and elevated unconjugated bilirubin, identifies haemolysis. Koilonychia and angular stomatitis are signs of IDA (nutritional, hypoproliferative). Conjunctival pallor is present in any anaemia regardless of cause and does not discriminate haemolytic from nutritional. The family history of splenectomy further supports a hereditary haemolytic condition (hereditary spherocytosis is a strong possibility here).