Page 3 of 19
IM9.1-2 | Anaemia Foundations — SDL Guide (Part 3)
Anaemia of Chronic Disease and Other Normocytic Causes
Anaemia of chronic disease (ACD), now more precisely termed anaemia of inflammation, is the commonest cause of anaemia in hospitalised patients and the second most common overall after IDA. It occurs in the context of chronic infections (tuberculosis — a critically important cause in India; HIV; osteomyelitis; infective endocarditis), inflammatory diseases (rheumatoid arthritis, SLE, inflammatory bowel disease), and malignancies. The pathophysiology is driven by inflammatory cytokines — particularly interleukin-6 (IL-6) — that induce hepatic synthesis of hepcidin, a 25-amino-acid peptide hormone that is the master regulator of iron homeostasis. Hepcidin binds to and causes degradation of ferroportin, the sole iron export channel on enterocytes and macrophages, blocking both intestinal iron absorption and release of stored iron from macrophages. The result is 'iron sequestration' — iron is trapped inside macrophages, unavailable for erythropoiesis, producing functional iron deficiency even when body iron stores are adequate or elevated.
Provided image
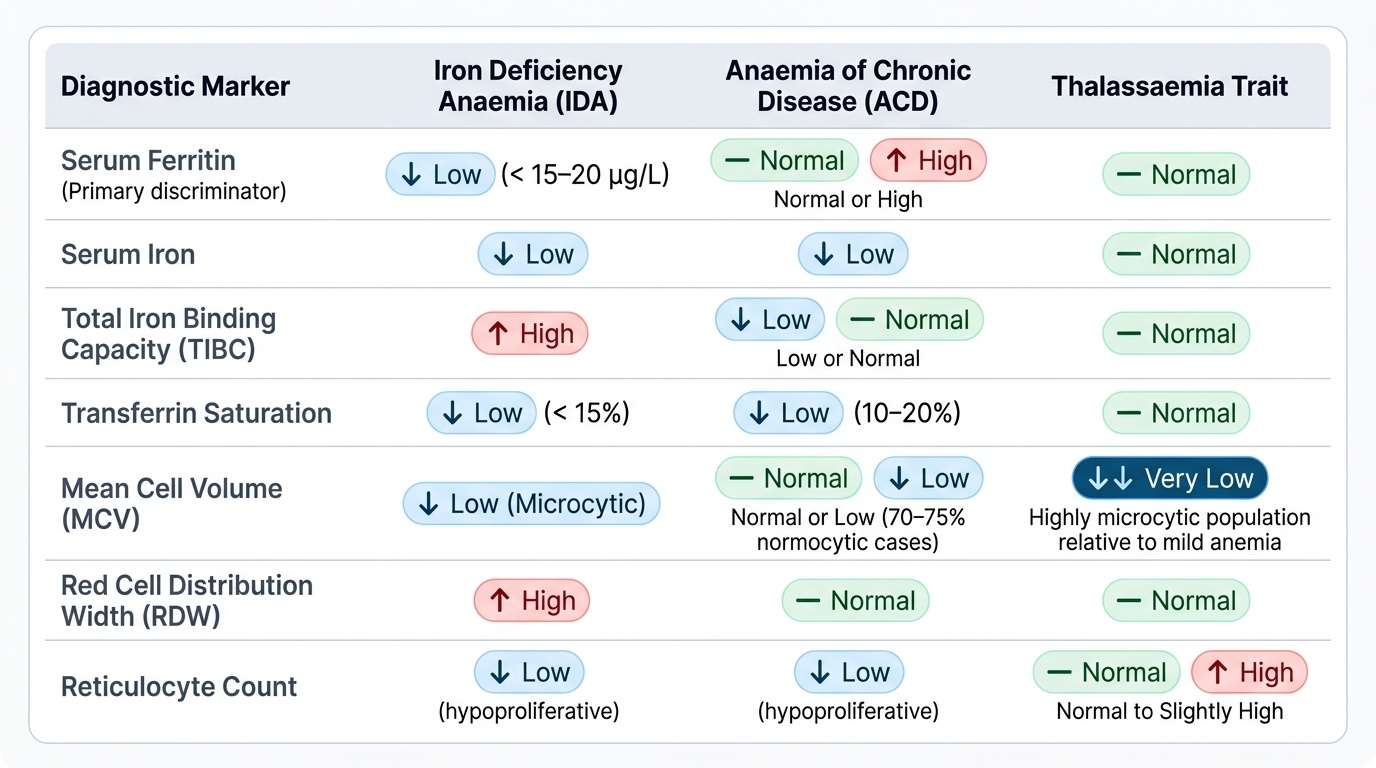
The haematological picture of ACD: typically mild-to-moderate anaemia; normocytic normochromic (MCV 80–95 fL) in approximately 70–75% of cases; microcytic hypochromic (MCV <80) in 25–30% (particularly in TB and malignancy); serum ferritin normal or elevated (ferritin is an acute-phase reactant — rises in inflammation regardless of iron stores); serum iron low; TIBC low or normal (in contrast to IDA where TIBC is elevated); transferrin saturation low (typically 10–20%); reticulocyte count low (hypoproliferative). The key discriminating test between IDA and ACD: serum ferritin — low in IDA (<15–20 µg/L; <30 µg/L is more sensitive), normal or high in ACD. Soluble transferrin receptor (sTfR) is elevated in IDA but not in ACD and can further discriminate, particularly when both conditions coexist (sTfR/log ferritin index).
Treatment of ACD targets the underlying disease. In patients with symptomatic anaemia (e.g., renal failure-associated anaemia), erythropoiesis-stimulating agents (ESAs) such as epoetin alpha or darbepoetin are used alongside intravenous iron if functional iron deficiency is confirmed.
Aplastic anaemia represents the extreme of hypoproliferative anaemia — pancytopenia from bone marrow failure. The marrow is hypocellular (replaced by fat) on biopsy. Most cases are acquired autoimmune (T-cell-mediated destruction of haematopoietic stem cells), triggered by drugs, viruses (hepatitis — seronegative hepatitis-associated aplastic anaemia), toxins, or idiopathic. Rare congenital forms include Fanconi anaemia and dyskeratosis congenita. Diagnosis requires bone marrow biopsy. Treatment: allogeneic haematopoietic stem cell transplantation (curative, preferred under 40 years with a matched sibling donor) or immunosuppressive therapy (anti-thymocyte globulin + cyclosporine + eltrombopag for those not transplantable).
Investigations in Anaemia: A Systematic Diagnostic Approach
Investigating anaemia begins with the full blood count (FBC) / complete blood count (CBC) — the haemogram — which provides the primary morphological data: haemoglobin, haematocrit, RBC count, MCV, MCH, MCHC, and RDW. The peripheral blood film (PBS) is the single most informative investigation after the CBC, providing direct visual information about RBC shape (poikilocytes — pencil cells in IDA, sickle cells, spherocytes, schistocytes, target cells, macro-ovalocytes), size (microcytes, macrocytes), colour (hypochromia), and the appearance of white cells (hypersegmented neutrophils in megaloblastic anaemia) and platelets. Every patient with unexplained anaemia should have a blood film reviewed by an experienced observer — automated analysers cannot replace morphological interpretation.
The reticulocyte count (automated ARC or corrected reticulocyte index) classifies the kinetic response: hyperproliferative (haemolysis/bleeding) vs hypoproliferative (deficiency/marrow failure). It must be ordered alongside the haemogram in every new anaemia presentation.
Targeted investigations by morphological category:
Microcytic anaemia:
- Serum ferritin: the most specific single test for IDA (low <15–20 µg/L); elevated in ACD and thalassaemia
- Serum iron, TIBC (total iron-binding capacity), transferrin saturation: low iron + high TIBC + low Tsat (<16%) = IDA; low iron + normal/low TIBC + low Tsat = ACD
- Haemoglobin electrophoresis / HPLC: HbA2 >3.5% confirms β-thalassaemia trait; HbS band confirms sickle cell haemoglobin
- Stool for occult blood / ova & parasites (if hookworm suspected)
Macrocytic anaemia:
- Serum B12 (cobalamin): <200 pg/mL confirms deficiency; borderline 200–300 pg/mL requires MMA testing
- Serum and RBC folate: serum folate <3 ng/mL; RBC folate more reliable in recent dietary change
- Serum MMA: elevated specifically in B12 deficiency; normal in folate deficiency
- Serum homocysteine: elevated in both B12 and folate deficiency
- Serum TSH: hypothyroidism causes macrocytosis; LFTs for liver disease; reticulocyte count for non-megaloblastic causes
- Anti-parietal cell antibodies, anti-intrinsic factor antibodies: if pernicious anaemia suspected
Normocytic anaemia / haemolytic workup:
- Serum LDH, unconjugated bilirubin, serum haptoglobin: the triad of haemolysis markers; LDH elevated, haptoglobin reduced, unconjugated bilirubin elevated
- Direct Coombs test (DAT): positive in AIHA; negative in intrinsic RBC defects (SCD, G6PD, hereditary spherocytosis)
- G6PD enzyme assay: note — false normal if tested during acute haemolytic episode (when G6PD-deficient cells have been lysed preferentially, leaving the least-deficient cells; test after recovery)
- Osmotic fragility test / EMA binding test: for hereditary spherocytosis
- HPLC for haemoglobinopathies
- Urine for haemoglobinuria (intravascular haemolysis — Coca-Cola coloured urine)
Bone marrow examination (aspiration ± trephine biopsy) is indicated when peripheral blood findings are insufficient: unexplained pancytopenia (aplastic anaemia vs infiltration), suspected myelodysplasia, leuco-erythroblastic blood film (marrow infiltration), refractory anaemia not responding to specific therapy, or when multiple cell lines are affected. The marrow biopsy is mandatory for aplastic anaemia diagnosis.
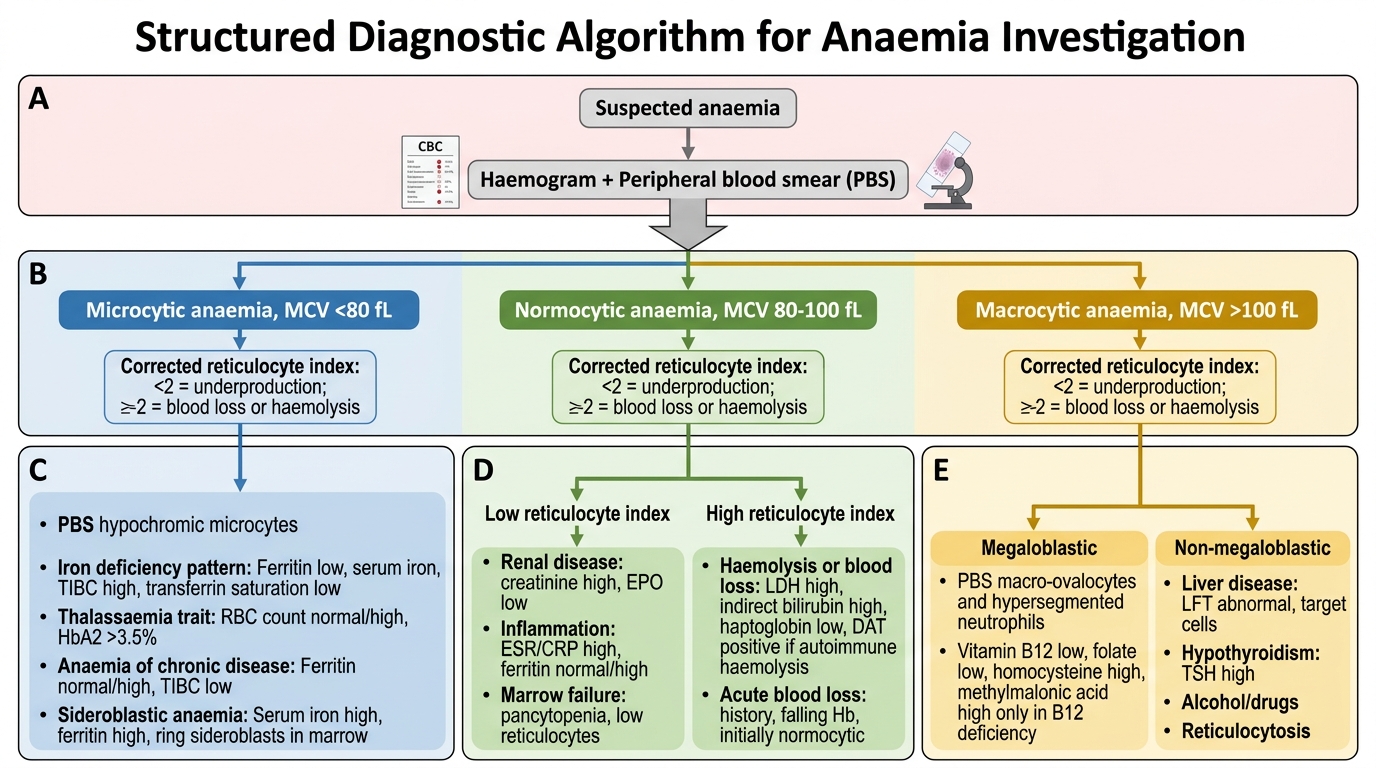
Diagnostic Algorithm for Anaemia Investigation
Principles of Management: An Overview by Aetiology
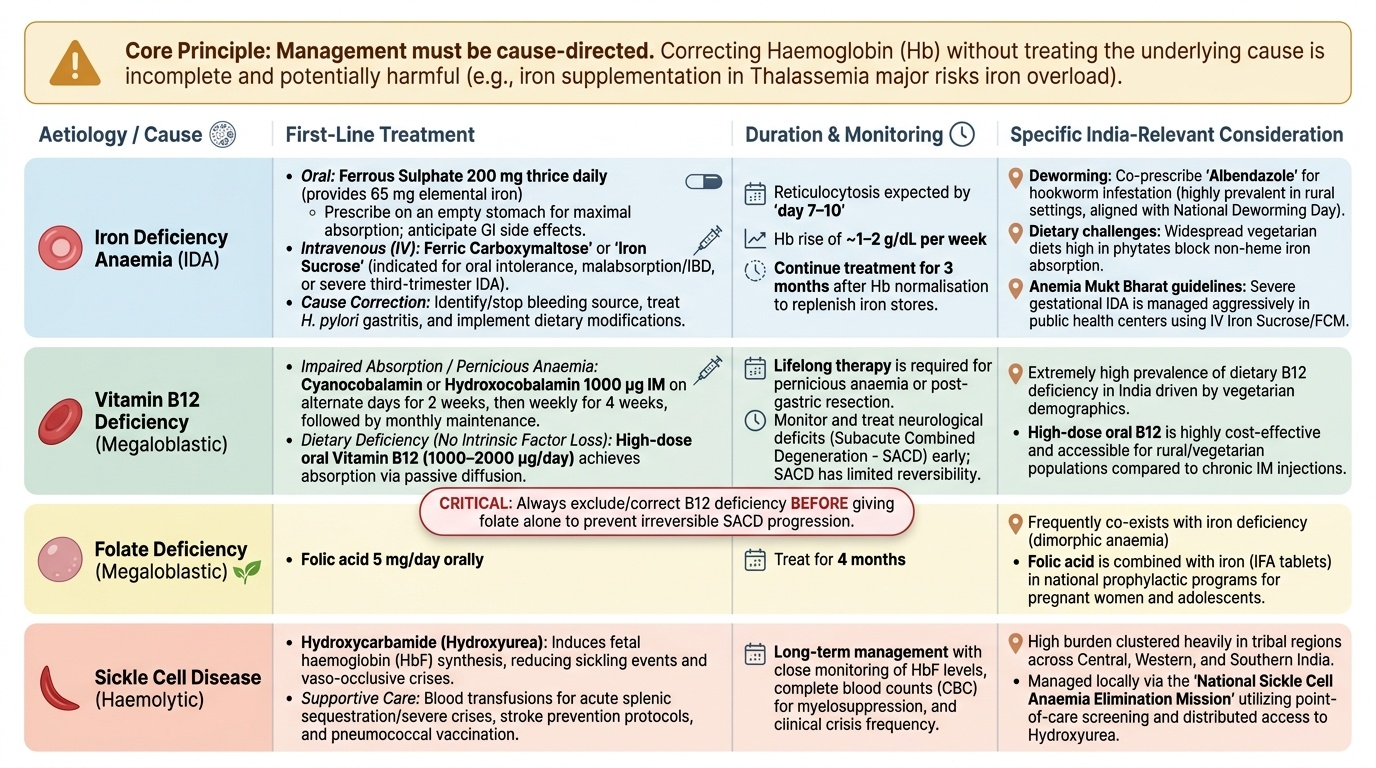
Management of anaemia is fundamentally cause-directed — there is no single treatment for 'anaemia' just as there is no single treatment for 'fever'. Correcting the haemoglobin without identifying and treating the underlying cause is not only incomplete but potentially harmful (e.g., iron supplementation in thalassaemia major risks iron overload; blood transfusion without addressing haemolysis only provides temporary relief). The following overview maps each major aetiology to its primary management principle, providing the conceptual framework that will be elaborated in the Anaemia Treatment module (SDL 4).
Provided image
Iron deficiency anaemia: Treat the cause (identify and stop the bleeding source; deworm if hookworm; modify diet; treat H. pylori-associated gastritis). Replace iron: oral ferrous sulphate 200 mg thrice daily (each 200 mg tablet = 65 mg elemental iron; prescribe on empty stomach for maximal absorption; anticipate GI side effects); expect reticulocytosis by day 7–10 and Hb rise of ~1–2 g/dL per week; treat for 3 months after Hb normalisation to replenish stores. Intravenous iron (ferric carboxymaltose or iron sucrose) when oral iron is not tolerated or absorbed (IBD, post-bariatric surgery, severe IDA in pregnancy).
Megaloblastic anaemia:
- B12 deficiency (dietary): cyanocobalamin or hydroxocobalamin intramuscular injection (1000 µg IM alternate day × 2 weeks, then weekly × 4 weeks, then monthly lifelong if pernicious anaemia — since absorption cannot be restored). High-dose oral B12 (1000–2000 µg/day) achieves adequate absorption by passive diffusion if intrinsic factor deficiency is NOT the cause (effective for dietary deficiency). Neurological deficits (SACD) may be reversible if treated within months; chronic SACD is less responsive.
- Folate deficiency: folic acid 5 mg/day orally for 4 months. CRITICALLY: always exclude and correct B12 deficiency BEFORE giving folate alone — folate supplementation can correct the megaloblastic anaemia but will allow SACD to progress in undiagnosed B12 deficiency ('masking' neurological disease).
Haemolytic anaemias:
- Sickle cell disease: hydroxycarbamide (hydroxyurea) — increases foetal haemoglobin (HbF), reduces sickling and vaso-occlusive crises; blood transfusion for acute severe anaemia; stroke prevention programme; pneumococcal vaccination (due to functional asplenia); penicillin prophylaxis; acute chest syndrome = medical emergency (exchange transfusion + antibiotics + oxygen).
- Thalassaemia major: regular blood transfusions (every 3–4 weeks to maintain Hb >10 g/dL) + iron chelation therapy (desferrioxamine SC or deferasirox oral) to prevent iron overload; bone marrow transplant is curative.
- AIHA (warm): corticosteroids (prednisolone 1 mg/kg/day) first-line; rituximab or splenectomy for refractory cases; folic acid supplementation.
- G6PD deficiency: avoid triggering drugs and fava beans; transfusion support during acute haemolytic episodes.
Anaemia of chronic disease: Primary treatment is managing the underlying disease (TB — NTEP regimen 2HRZE + 4HRE; HIV — NACO antiretroviral therapy; rheumatoid arthritis — disease-modifying agents). ESAs (erythropoietin) for symptomatic ACD in chronic kidney disease. IV iron when functional iron deficiency is demonstrated (low sTfR/log ferritin index).
Blood transfusion is a temporary and specific intervention — not a long-term treatment for any chronic anaemia. Indications and principles of blood component therapy are detailed in the treatment module.
SELF-CHECK
A 50-year-old man with active pulmonary tuberculosis has Hb 9.8 g/dL, MCV 84 fL, serum iron 6 µmol/L (low), serum ferritin 180 µg/L (elevated), and TIBC 220 µg/dL (low normal). What is the most likely type of anaemia and the mechanism?
A. Iron deficiency anaemia — absolute iron depletion due to malnutrition
B. Megaloblastic anaemia — B12 deficiency due to TB-related malabsorption
C. Anaemia of chronic disease — hepcidin-mediated iron sequestration in macrophages
D. Haemolytic anaemia — autoimmune destruction of RBCs triggered by TB antigens
Reveal Answer
Answer: C. Anaemia of chronic disease — hepcidin-mediated iron sequestration in macrophages
Active pulmonary TB is a chronic inflammatory disease that drives IL-6 production, stimulating hepatic hepcidin synthesis. Hepcidin degrades ferroportin on macrophages and enterocytes, trapping iron inside macrophages (iron sequestration). The result: low serum iron (iron not being released by macrophages), ELEVATED ferritin (ferritin is an acute-phase reactant and rises despite functional iron deficiency), and normal or low TIBC (unlike IDA where liver synthesises more transferrin and TIBC rises). This is the classic ACD pattern. IDA would show low ferritin, high TIBC. MCV is normocytic (84 fL) as is typical in ACD.
CLINICAL PEARL
When evaluating a patient with microcytic anaemia, the MCV alone does not distinguish iron deficiency anaemia from thalassaemia trait — yet the management is completely different (IDA requires iron replacement; thalassaemia trait requires genetic counselling and no iron supplementation unless concurrent IDA is confirmed). The three bedside discriminators are: (1) RDW — high in IDA (>14.5%), typically normal in thalassaemia trait; (2) Mentzer Index (MCV ÷ RBC count) — if >13, favours IDA; if <13, favours thalassaemia trait; and (3) serum ferritin — low in IDA (most specific test), normal or elevated in thalassaemia trait. Confirmatory test: HPLC showing elevated HbA2 >3.5% in β-thalassaemia trait. Never prescribe empirical iron therapy for microcytic anaemia without excluding thalassaemia in a patient from a high-prevalence region — unnecessary iron loading in thalassaemia major can be harmful.
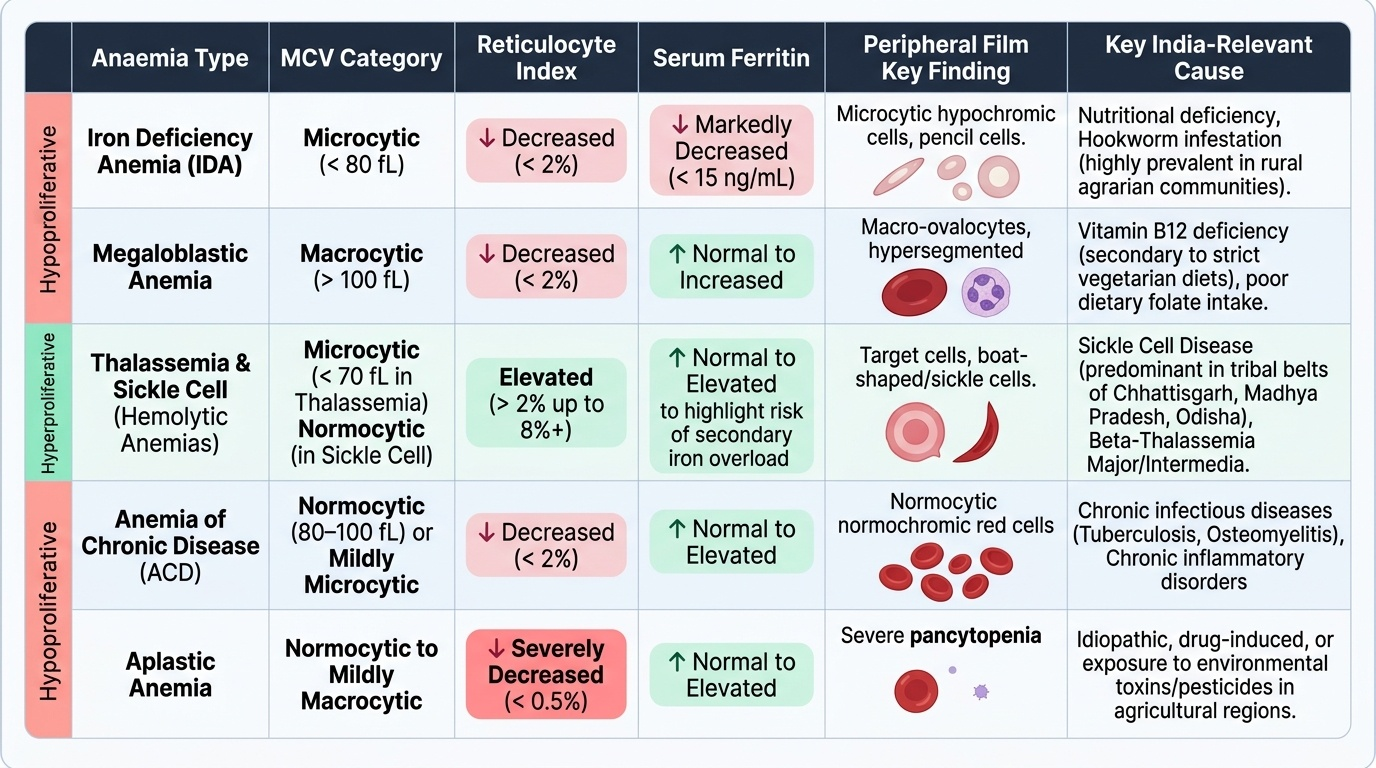
Self-Assessment: Integrating Classification and Aetiology
You have now covered the definitional thresholds of anaemia, the two-axis morphological-kinetic classification framework, and the major aetiological groups — IDA, megaloblastic anaemias (B12 and folate), haemolytic anaemias (intrinsic and extrinsic, with India-specific emphasis on sickle cell disease, thalassaemia, and G6PD deficiency), anaemia of chronic disease, and aplastic anaemia. The three self-assessment scenarios below ask you to apply the classification matrix to real clinical and laboratory data, arriving at the morphological class, kinetic category, mechanism, and aetiology before reading the analysis. This integrative skill — reading a set of haematological results and reasoning to a diagnosis — directly addresses the IM9.1 and IM9.2 competencies at the KH (applied knowledge) level expected of a final-year MBBS student. For each case, note which axis (morphological or kinetic) gives you the first clue, which single test would confirm the diagnosis, and what the mandatory next clinical step is. The reference summary below anchors your self-assessment.
Provided image
Scenario A: A 15-year-old boy from Chhattisgarh has Hb 7.8 g/dL, MCV 72 fL, reticulocyte count 8%, elevated bilirubin, and low haptoglobin. Peripheral film: target cells and boat-shaped cells. What is the classification and most likely diagnosis?
Analysis: Microcytic anaemia (MCV 72 fL) + hyperproliferative (reticulocyte 8%) + haemolysis markers (elevated bilirubin, low haptoglobin) = microcytic haemolytic anaemia. Target cells are characteristic of haemoglobinopathies. The boat-shaped or elongated cells, combined with geographic origin (tribal belt, central India), suggest sickle cell disease or HbS-thalassaemia compound heterozygote. Confirm with HPLC (HbS band).
Scenario B: A 70-year-old woman has Hb 10.2 g/dL, MCV 68 fL, RDW 17.8%, serum iron 5 µmol/L, ferritin 6 µg/L, TIBC 420 µg/dL. She has no menstrual history. What is the aetiology and the mandatory additional investigation?
Analysis: Microcytic hypochromic anaemia with markedly low ferritin and high TIBC = textbook IDA. However, in a postmenopausal woman (or any male at any age) presenting with IDA, gastrointestinal malignancy must be excluded — colonoscopy and upper GI endoscopy are mandatory, regardless of any other plausible explanation for iron deficiency.
Scenario C: A 32-year-old pregnant woman has Hb 9.0 g/dL, MCV 80 fL, reticulocyte index 1.2, normal serum iron, normal ferritin, and normal RDW. Peripheral film shows a dimorphic RBC population — some microcytic hypochromic cells, some normocytic. TSH is normal. What is the likely explanation?
Analysis: Dimorphic blood film with normal MCV = mixed deficiency (concurrent iron and folate deficiency — common in pregnancy). Iron deficiency shifts MCV down, folate deficiency shifts it up, resulting in a 'pseudo-normal' average MCV. The peripheral film reveals the two populations. This is a classic pregnancy scenario in India where both nutritional deficiencies coexist — treat with concurrent iron and folate supplementation.