Page 2 of 14
MI3.1-4 | Infective Endocarditis & Rheumatic Fever — SDL Guide (Part 2)
Infective Endocarditis: Clinical Features & Complications
Infective Endocarditis: Features, Duke's Criteria & Complications
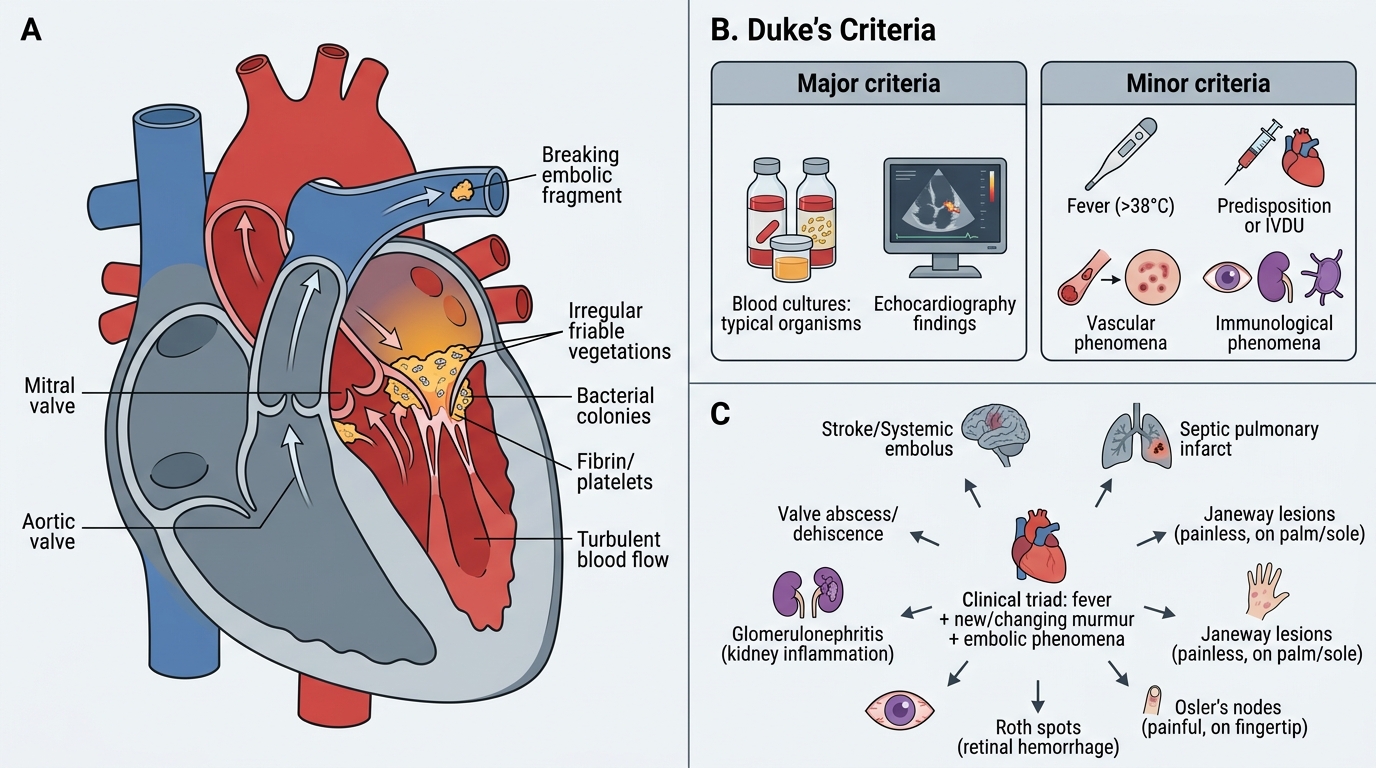
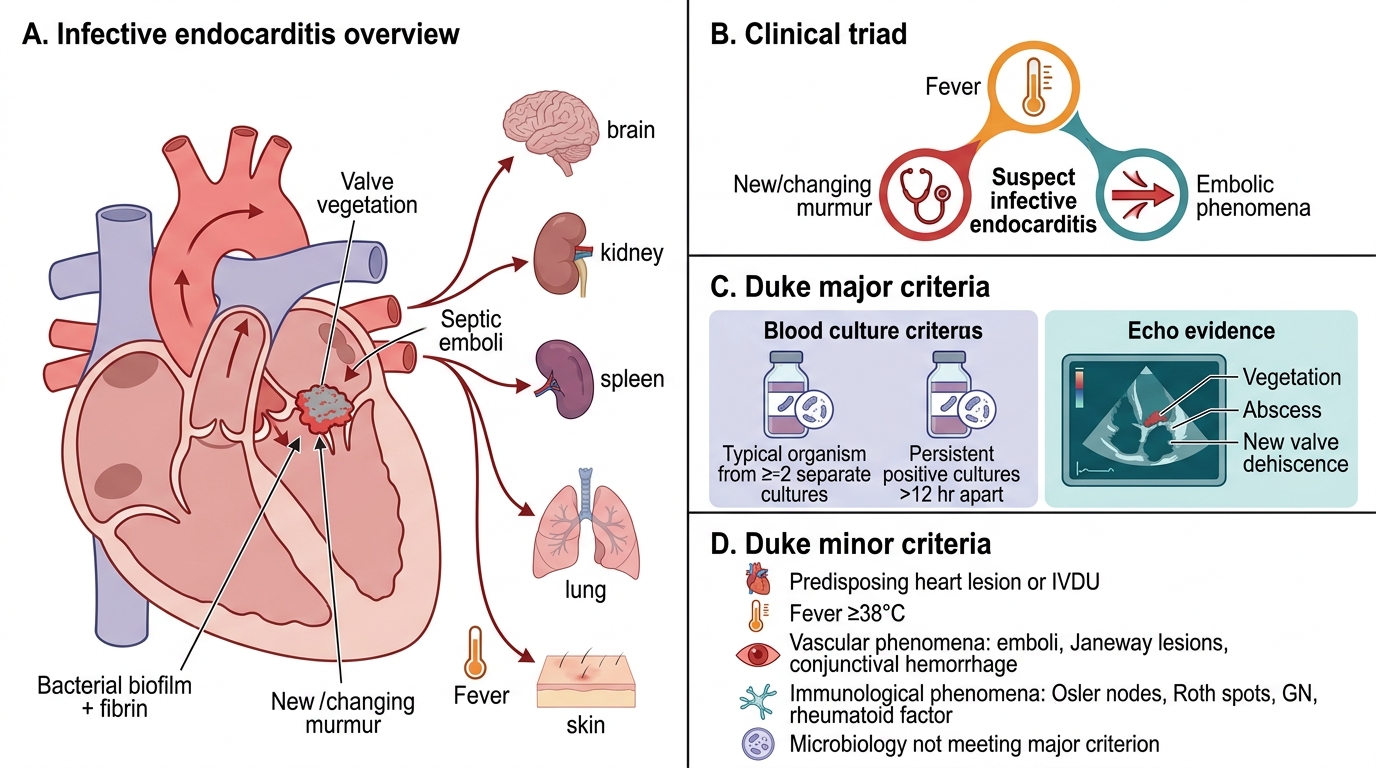
Clinical triad: Fever + new/changing murmur + embolic phenomena.
Duke's Criteria — diagnostic standard (Definite IE = 2 major, or 1 major + 3 minor, or 5 minor criteria):
Major criteria:
- Blood culture: Typical organism (viridans strep, S. aureus, HACEK, enterococcus) from ≥2 separate cultures; or persistently positive (>12 hr apart) — key diagnostic pillar
- Echocardiographic evidence: Vegetation, abscess, or new partial valve dehiscence
Minor criteria:
- Predisposing cardiac condition or IVDU
- Fever ≥38°C
- Vascular phenomena: major arterial emboli, septic pulmonary infarcts, Janeway lesions, conjunctival haemorrhages
- Immunological phenomena: Osler's nodes, Roth's spots, glomerulonephritis, positive rheumatoid factor
- Microbiological evidence (positive blood culture not meeting major criteria)
Classic peripheral stigmata:
- Janeway lesions — non-tender haemorrhagic macules on palms/soles (embolic, S. aureus)
- Osler's nodes — painful nodules on finger pulps (immune complex vasculitis)
- Roth's spots — oval retinal haemorrhages with white centres
- Splinter haemorrhages — subungual linear haemorrhages
Complications:
- Local: valve destruction, ring abscess, fistula, heart failure
- Embolic: stroke (left-sided IE), pulmonary septic emboli (right-sided IE), splenic/renal infarction
- Immunological: glomerulonephritis, arthritis
CLINICAL PEARL
Blood culture timing in IE: Bacteraemia in IE is continuous (not intermittent), so blood cultures can be taken at any time — you do NOT need to wait for fever spikes. Collect 3 sets of blood cultures from 3 separate venepuncture sites within 1–2 hours before starting antibiotics. Each set = aerobic + anaerobic bottle. Volume matters: 10 mL per bottle in adults. Never delay antibiotics >1–2 hours in severely ill patients — culture sensitivity remains high even after one dose.
Laboratory Diagnosis: Blood Cultures & Sepsis Concept
Infective Endocarditis: Clinical Features and Duke Criteria
Blood culture — the cornerstone of IE diagnosis:
Collection protocol:
1. Disinfect venepuncture site with 70% alcohol + povidone-iodine (or chlorhexidine); allow to dry fully
2. Use strict aseptic technique — gloves, mask; disinfect bottle rubber septum
3. Inoculate aerobic bottle first (from the syringe; air bubbles less concern in aerobic bottle)
4. 3 sets from 3 sites — within 1–2 hours if acute; over 24 hours if subacute
5. Transport to laboratory at body temperature (not refrigerated); load into automated BACTEC/BacT/ALERT system immediately
BACTEC/automated blood culture systems:
- Continuously monitor CO₂ production (metabolic indicator of bacterial growth)
- Flag positive bottles → Gram stain → subculture → identification + sensitivity
- Time to positivity: Staphylococci 1–2 days; HACEK organisms 5–7 days (require extended 6-week incubation for suspected IE)
Blood culture-negative IE (BCNIE):
- Accounts for 5–10% of IE cases
- Causes: prior antibiotic use (commonest), fastidious organisms (Coxiella burnetii, Bartonella, Brucella, Tropheryma whipplei)
- Investigations: serology (Coxiella phase II IgG ≥1:800), PCR of excised valve tissue, broad-range 16S rRNA PCR
Concept of sepsis in IE:
Sepsis = life-threatening organ dysfunction caused by a dysregulated host response to infection (Sepsis-3 definition). In IE, septic emboli seed distant organs; toxins and immune complexes drive systemic inflammation. Septic shock = sepsis + vasopressor requirement + lactate >2 mmol/L despite fluid resuscitation. IE is a recognised cause of sepsis — prompt blood cultures and antibiotics are life-saving.
Interpreting IE laboratory results:
| Investigation | Significance |
|---|---|
| Blood culture positivity (≥2/3 with same organism) | Major Duke's criterion |
| ESR, CRP elevated | Supportive (non-specific) |
| Anaemia, haematuria | Systemic involvement |
| Echocardiography (TTE/TOE) | Visualises vegetations; TOE more sensitive |
| Rheumatoid factor | Positive in 50% — immune complexes |
⚑ AI image — pending faculty review (auto-QA score 5/10; best of 3 attempts)
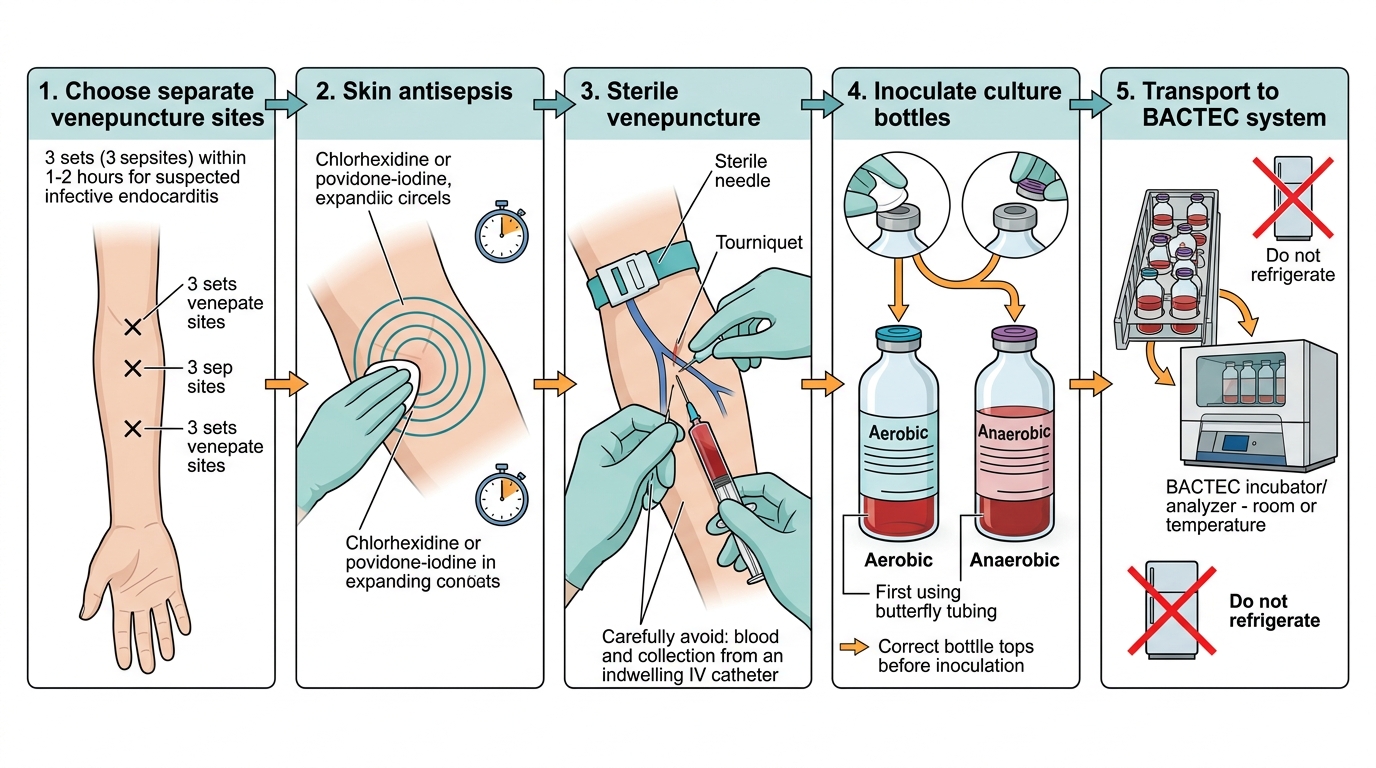
Step-by-Step Blood Culture Collection for Suspected Infective Endocarditis
SELF-CHECK
A patient with suspected infective endocarditis needs blood cultures. Which statement about collection is CORRECT?
A. Wait for fever spike before collecting blood cultures to maximise yield
B. Collect blood only from an indwelling IV catheter to avoid pain
C. Collect 3 sets from 3 separate venepuncture sites within 1–2 hours
D. Refrigerate blood culture bottles to preserve organisms during transport
Reveal Answer
Answer: C. Collect 3 sets from 3 separate venepuncture sites within 1–2 hours
IE bacteraemia is continuous — timing relative to fever is irrelevant. Catheter blood cultures have high contamination rates. 3 sets from 3 separate sites maximise sensitivity and help distinguish true bacteraemia from skin contaminants. Blood culture bottles must be transported at body/room temperature (NOT refrigerated) — cold temperatures kill fastidious organisms.
SELF-CHECK
Which of the following organisms is the MOST common cause of subacute infective endocarditis on a previously damaged (rheumatic) mitral valve?
A. Staphylococcus aureus
B. Viridans streptococci
C. Candida albicans
D. Pseudomonas aeruginosa
Reveal Answer
Answer: B. Viridans streptococci
Viridans streptococci (S. sanguinis, S. mutans, S. salivarius) are part of the oral flora and enter the bloodstream during dental procedures. They preferentially colonise previously damaged valves (rheumatic heart disease) and cause the classic subacute, indolent course. S. aureus causes acute IE and can destroy normal valves.