Page 2 of 10
MI8.{1-2,4} | Urinary Tract & Sexually Transmitted Infections — SDL Guide (Part 2)
Viral STIs and Parasitic Genitourinary Infections
Viral STIs: HSV and HPV
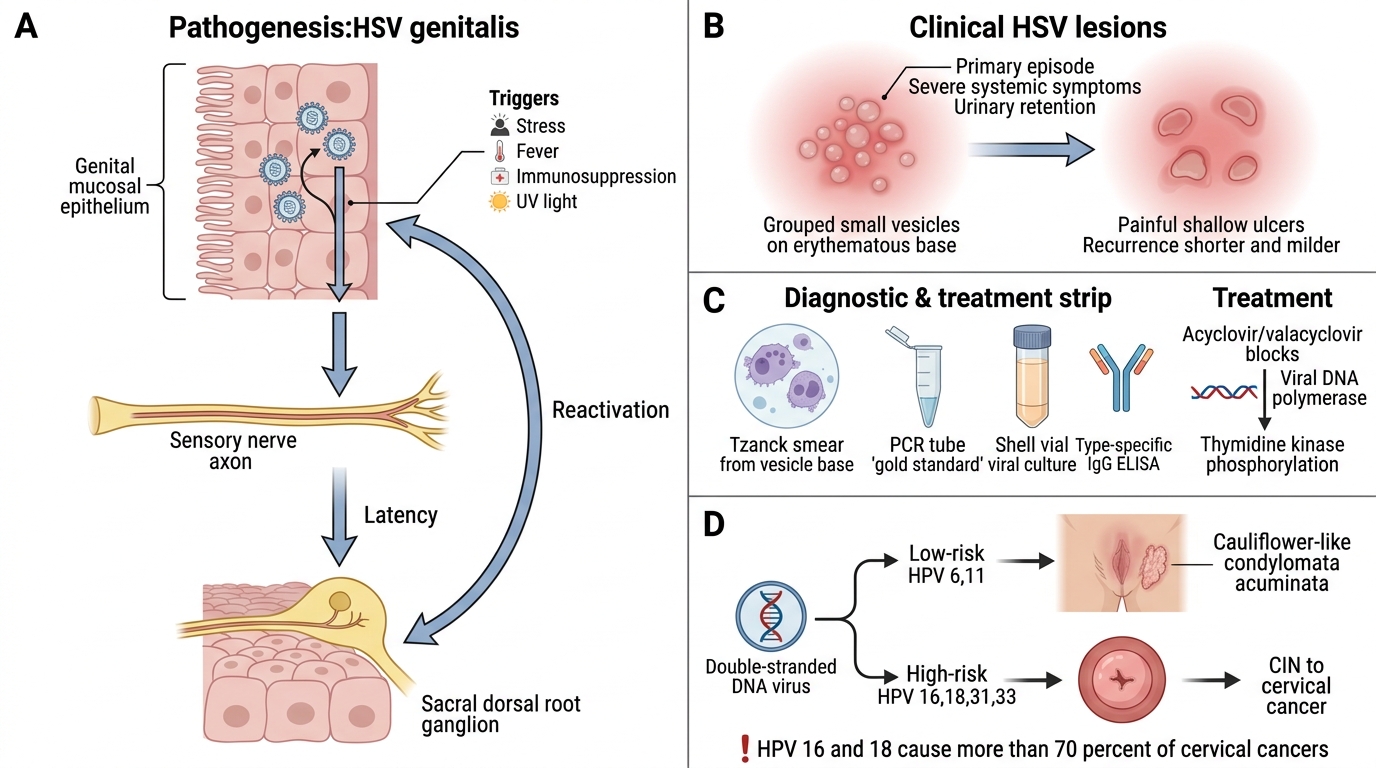
Herpes Genitalis (HSV-1/HSV-2)
- Pathogenesis: Primary infection → epithelial replication → retrograde axonal transport → latency in sacral dorsal root ganglia → reactivation triggers (stress, fever, immunosuppression, UV light)
- Clinical features: Multiple small grouped vesicles on an erythematous base → painful ulcers → heal in 10–14 days. Primary episode is more severe (systemic symptoms, urinary retention). Recurrences are shorter and milder.
- HSV-2 predominantly causes genital herpes; HSV-1 is increasingly common cause (oral–genital transmission)
- Neonatal herpes: Acquired during delivery through infected birth canal; devastating — can cause disseminated disease, encephalitis; mortality ~60% without treatment
- Diagnosis: Tzanck smear (vesicle base → multinucleated giant cells), viral culture (Shell vial), PCR (gold standard), type-specific IgG ELISA (seroprevalence studies)
- Management: Acyclovir (nucleoside analogue — phosphorylated by viral thymidine kinase → inhibits viral DNA polymerase); valacyclovir for recurrences
Human Papillomavirus (HPV)
- Double-stranded DNA virus; >200 types; sexually transmitted
- Low-risk types (6, 11): Genital warts (condylomata acuminata) — cauliflower-like, on glans, vulva, perianal region
- High-risk types (16, 18, 31, 33): Cervical intraepithelial neoplasia (CIN) → cervical cancer; also oropharyngeal, anal, penile, vulvar cancers. HPV 16 and 18 cause >70% of cervical cancers
- Pathogenesis: E6 oncoprotein binds and degrades p53 (tumour suppressor); E7 oncoprotein inactivates pRb → uncontrolled cell proliferation
- Diagnosis: Cervical cytology (Pap smear) — detects CIN (koilocytes = pathognomonic HPV-infected cells); colposcopy + biopsy for CIN grading; HPV DNA test (Cobas, Hybrid Capture 2)
- Prevention: Bivalent (HPV 16/18), quadrivalent (6/11/16/18), or 9-valent vaccines; India's UIP includes bivalent HPV vaccine for girls aged 9–14 years
Trichomonas vaginalis (Parasitic STI)
- Pathogen: Flagellated protozoan; anaerobic; pear-shaped; 5 flagella (4 anterior + 1 posterior forming undulating membrane)
- Clinical features: Females: frothy, yellow-green, malodorous vaginal discharge; pruritus; strawberry cervix (punctate haemorrhages on colposcopy). Males: usually asymptomatic; mild urethritis
- Pathogenesis: Binds to vaginal epithelial cells; alkaline pH (raised vaginal pH); cytotoxin production
- Diagnosis: Wet mount preparation of vaginal discharge (or urethral discharge) — motile trichomonads with characteristic tumbling motility; NAAT (most sensitive — PCR-based); culture on Diamond's medium; Gram stain less reliable
- Management: Metronidazole (single dose 2g) for patient and partner simultaneously
Renal tuberculosis and other genitourinary infections
- Renal TB: M. tuberculosis reaches kidney haematogenously; granulomata form in renal cortex → caseous necrosis → cavitation → spread to ureters (structure/stricture) and bladder. Sterile pyuria is the classic microbiological clue.
- Schistosomiasis (S. haematobium): Endemic in Africa; rare in India; eggs deposited in bladder wall → haematuria, chronic cystitis, squamous cell carcinoma of bladder
- Filariasis (Wuchereria bancrofti): Lymphatic obstruction → lymphoedema; scrotal lymphoedema → hydrocele; chyluria (lymph in urine — milky white urine)
CLINICAL PEARL
Syndromic management of STIs in India: NACO's syndromic management approach treats STI syndromes (urethral discharge, genital ulcer, vaginal discharge) empirically without microbiological diagnosis, targeting the commonest causative organisms. For urethral discharge: treat both gonorrhoea (ceftriaxone 500 mg IM single dose) and chlamydia (azithromycin 1g stat or doxycycline 100 mg BD × 7 days) simultaneously — this two-drug approach covers the syndromic cause without culture. Partner treatment and condom promotion are integral to the NACO STI management protocol used at all PHC-level clinics across India.
Prevention of STIs and UTIs
⚑ AI image — pending faculty review (auto-QA score 7/10; best of 3 attempts)
Prevention of STIs and UTIs
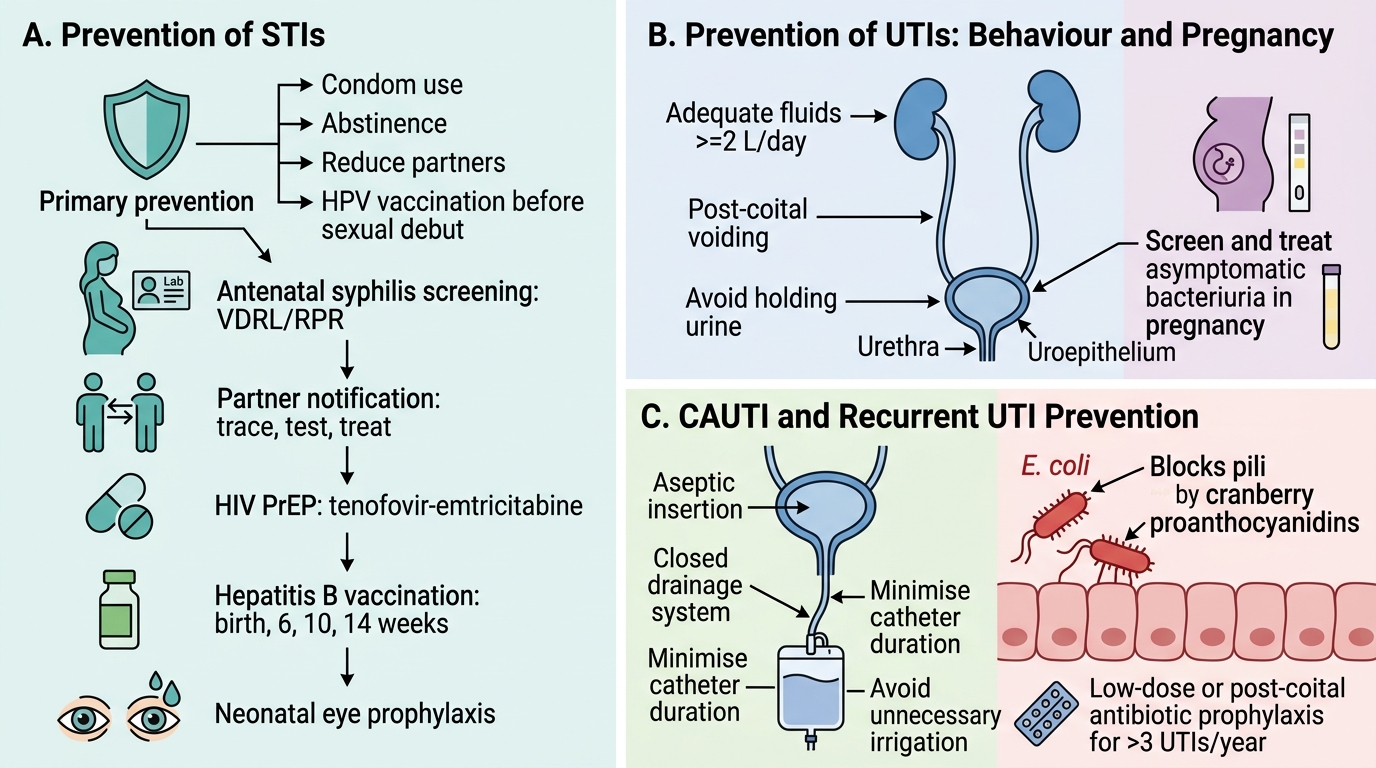
Prevention of STIs:
- Primary prevention: Condom use (male and female), sexual abstinence, reducing number of partners, HPV vaccination (before sexual debut, most effective)
- Screening: Antenatal syphilis screening (VDRL/RPR) in all pregnant women is mandatory in India — early treatment prevents congenital syphilis
- Partner notification: Index patient's sexual contacts must be traced and offered testing/treatment
- Pre-exposure prophylaxis (PrEP): Tenofovir–emtricitabine for HIV-negative high-risk individuals (now available under NACO)
- Hepatitis B vaccination: UIP schedule (birth + 6 weeks + 10 weeks + 14 weeks) prevents HBV STI
- Neonatal prophylaxis: Eye drops at birth (prophylaxis for gonococcal/chlamydial ophthalmia neonatorum)
Prevention of UTIs:
- Behavioural: Post-coital voiding, adequate fluid intake (≥2 L/day), avoid holding urine
- Catheter care (CAUTI prevention): Minimise catheter use and duration; maintain closed drainage system; aseptic insertion technique; avoid unnecessary bag irrigation
- Cranberry products: Proanthocyanidins inhibit E. coli type 1 pili adhesion to uroepithelium — evidence for prevention in women with recurrent UTIs is moderate
- Antibiotic prophylaxis: Low-dose prophylactic antibiotics for women with >3 UTIs/year (nitrofurantoin, trimethoprim); post-coital prophylaxis is an alternative
- Asymptomatic bacteriuria in pregnancy: Must be screened and treated (risk of progression to pyelonephritis is 20–40%)