Page 2 of 11
MI9.1-3 | Zoonotic & Opportunistic Infections — SDL Guide (Part 2)
Opportunistic Infections (OI) in Immunocompromised Hosts (MI9.2)
Opportunistic Infections in Immunocompromised Hosts
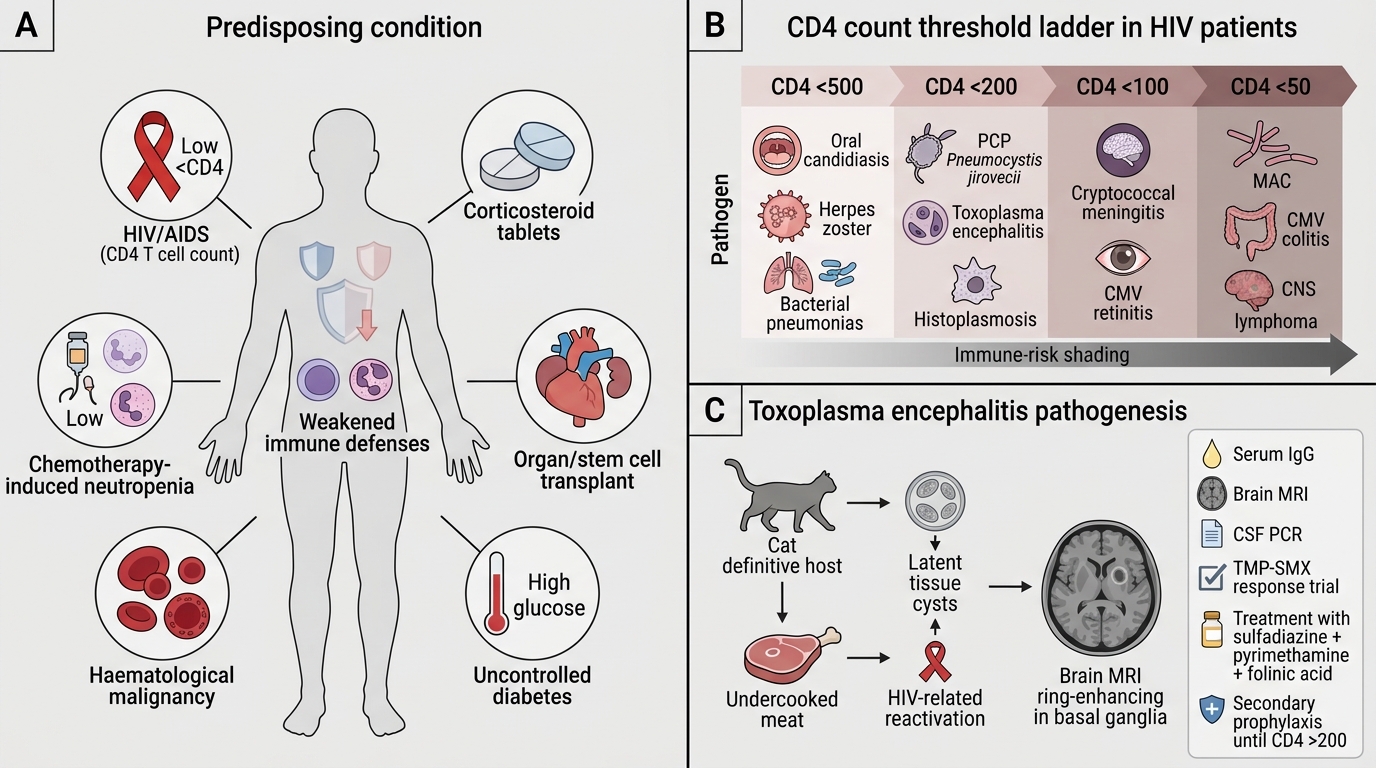
Predisposing conditions: HIV/AIDS, prolonged corticosteroid therapy, neutropenia (post-chemotherapy), organ/stem cell transplant, haematological malignancies, uncontrolled diabetes.
OIs classified by CD4 count threshold (HIV patients):
| CD4 Count | OI |
|---|---|
| <500 | Oral candidiasis, Herpes zoster, Bacterial pneumonias |
| <200 | PCP (Pneumocystis jirovecii), Toxoplasma encephalitis, Histoplasmosis |
| <100 | Cryptococcal meningitis (C. neoformans), CMV retinitis |
| <50 | MAC (M. avium complex), CMV colitis, CNS lymphoma (EBV-driven) |
Key OIs:
Toxoplasma encephalitis (Toxoplasma gondii):
- Obligate intracellular parasite; definitive host: cats; transmission via undercooked meat (bradyzoites) or oocysts (cat faeces)
- HIV patients: reactivation of latent tissue cysts → ring-enhancing lesions on MRI (basal ganglia) → seizures, focal deficits
- Diagnosis: Serum IgG (past infection = latent cyst); brain MRI + empirical TMP-SMX response trial; PCR of CSF
- Treatment: Sulfadiazine + pyrimethamine + folinic acid; lifelong secondary prophylaxis until CD4 >200
Cryptococcal Meningitis (Cryptococcus neoformans):
- Encapsulated yeast; pigeon droppings; India ink (cryptococcal capsule appears as halo around dark yeast)
- Subacute meningitis in HIV (CD4 <100); elevated opening pressure; CSF: mild pleocytosis
- Diagnosis: India ink of CSF; Cryptococcal Antigen (CrAg) lateral flow assay (serum/CSF — rapid, highly sensitive); culture on Sabouraud's/Niger seed agar (melanin production — black colonies)
- Treatment: Liposomal amphotericin B + flucytosine (induction) → fluconazole (consolidation and maintenance)

India Ink Preparation of Cryptococcus neoformans in CSF
Candida infections in immunocompromised:
- Oral thrush (CD4 <500) → oesophageal candidiasis (AIDS-defining, CD4 <200)
- Candidaemia in neutropenic patients and ICU (central line, broad-spectrum antibiotics)
- Diagnosis: KOH mount (pseudohyphae + budding yeast); blood culture in BACTEC; MALDI-TOF for species identification
- Treatment: Fluconazole (non-severe); echinocandins (caspofungin) for invasive/fluconazole-resistant
CMV retinitis: CD4 <50; painless progressive visual loss; 'pizza pie' retina on fundoscopy; PCR of vitreous; Ganciclovir IV + oral valganciclovir maintenance
SELF-CHECK
A 40-year-old HIV-positive patient presents with 3 weeks of severe headache, neck stiffness and photophobia. CSF analysis shows: lymphocytic pleocytosis, low glucose, elevated protein. India ink stain shows organisms with clear halos. The MOST sensitive rapid diagnostic test available is:
A. Serum VDRL
B. Cryptococcal Antigen (CrAg) lateral flow assay
C. Serum ASO titre
D. Widal test
Reveal Answer
Answer: B. Cryptococcal Antigen (CrAg) lateral flow assay
India ink showing organisms with capsular halos in CSF of an HIV patient confirms Cryptococcal meningitis. The CrAg lateral flow assay (serum or CSF) has >99% sensitivity and >95% specificity — it is the recommended rapid test by WHO and NACO for diagnosis and targeted screening (CrAg screening when CD4 <100).
Choosing the Right Investigation (MI9.3)
Choosing the Right Investigation in Suspected Zoonosis and Opportunistic Infection
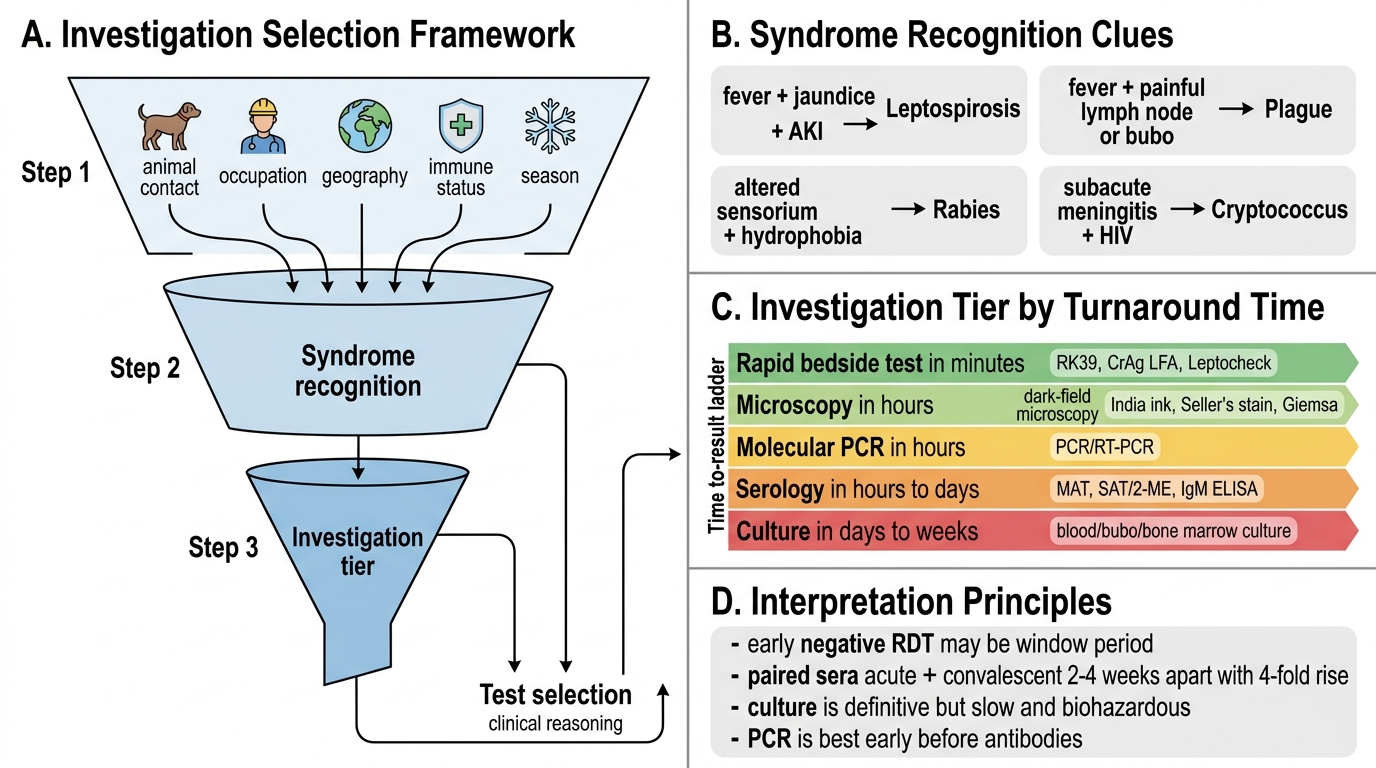
Framework for investigation selection in suspected zoonosis/OI:
Step 1 — Epidemiological clue (animal contact, occupation, geography, immune status, season)
Step 2 — Syndrome recognition (fever + jaundice + AKI → leptospirosis; fever + lymph node + bubo → plague; altered sensorium + hydrophobia → rabies; subacute meningitis + HIV → cryptococcus)
Step 3 — Investigation tier:
- Rapid bedside test (minutes): RDTs — RK39 for Kala-azar, CrAg LFA for Cryptococcus, Leptocheck for Leptospirosis, HRIG eligibility score for rabies exposure
- Microscopy (hours): Dark-field for Leptospira, India ink for Cryptococcus, Seller's stain for Negri bodies (Rabies), Giemsa for intracellular pathogens
- Serology (hours–days): MAT for Leptospirosis, SAT/2-ME for Brucella, Widal for typhoid (not a zoonosis per se), IgM ELISA
- Culture (days–weeks): Blood/bubo/bone marrow culture (BSL considerations for Brucella/Plague)
- Molecular (hours): PCR/RT-PCR for rabies, Nipah, KFD, Leptospira
Interpretation principles:
- A negative RDT does not rule out infection in early disease (window period)
- Paired sera (acute + convalescent, 2–4 weeks apart) with 4-fold rise in titre = gold standard serology
- Culture positivity = definitive diagnosis but slow and biohazardous for BSL-3 organisms
- PCR is most sensitive in the early/acute phase before antibody development