Page 1 of 14
OG1.1-3 | Maternal, Perinatal, Stillbirth and Abortion Statistics — SDL Guide
Learning Objectives
- Define and distinguish maternal mortality ratio (MMR), maternal mortality rate, maternal morbidity, and maternal near-miss with their correct numerators and denominators
- Define and distinguish perinatal mortality rate, neonatal mortality rate, stillbirth rate, and abortion with their gestational thresholds
- Explain the concept and process of perinatal and neonatal mortality audit
- Interpret current Indian vital statistics figures in the context of SDG targets
- Apply knowledge of vital statistics definitions in clinical governance and audit contexts
INSTRUCTIONS
Vital statistics are the quantitative language of maternal and perinatal health. Every obstetric department uses these indicators to benchmark care quality, identify preventable deaths, and justify resource allocation. As a final-year student entering clinical practice, you will encounter these definitions in case discussions, departmental audits, and national programme reviews. Understanding the precise numerators, denominators, and gestational thresholds is not a theoretical exercise — it determines how deaths are classified, how audits are conducted, and how India measures its progress toward Sustainable Development Goals.
References
- DC Dutta's Textbook of Obstetrics, 9th Ed, Ch 1 — Vital Statistics (textbook)
- Williams Obstetrics, 25th Ed, Ch 1 — Overview of Obstetrics (textbook)
- WHO: Evaluating the Quality of Care for Severe Pregnancy Complications — The WHO Near-Miss Approach for Maternal Health, 2011 (guideline)
- India SRS (Sample Registration System) Statistical Report 2020, Office of the Registrar General, India (report)
- India Maternal Death Review (MDR) Guidelines, MoHFW 2017 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
It is 2 AM. A 24-year-old woman, 32 weeks pregnant, arrives unconscious at your district hospital after a prolonged journey from a remote village. She had severe headache and fits at home. She dies 40 minutes after arrival despite resuscitation. The next morning, the obstetric department conducts a case review. Is her death classified as a maternal death? What numerator does it enter — the MMR or the maternal mortality rate? Which denominator applies? And what systemic failures does this death flag in the perinatal audit that will follow for her baby, who was delivered by emergency caesarean and now lies in the NICU? Before you can answer any of these questions, you need to master the precise definitions of vital statistics in obstetrics.
WHY THIS MATTERS
India's maternal mortality ratio fell from 556 per 100,000 live births in 1990 to 97 per 100,000 live births in 2018–20 (SRS) — an extraordinary achievement, yet still more than double the SDG target of fewer than 70 by 2030. Every number in that sentence depends on a precisely defined denominator. As a clinician, you will participate in maternal death reviews, perinatal audits, and facility quality assessments. Misclassifying a death — say, calling an abortion-related death 'indirect' when it is 'direct' — distorts the data that policies are built on. Getting these definitions right is a clinical governance responsibility, not just an exam requirement.
RECALL
From Community Medicine (Preventive and Social Medicine), recall: the crude death rate uses total population in the denominator; cause-specific rates use the at-risk population. From basic obstetrics, recall: the gestational milestones — viability is generally accepted at 28 weeks in India (some guidelines use 20 weeks for abortion definition). From anatomy and physiology, recall: the reproductive age span (15–49 years) that defines the denominator for some maternal indicators. These building blocks are the scaffolding for today's material.
Why Vital Statistics Matter in Obstetric Practice
Vital statistics in obstetrics are a systematic set of quantitative indices that measure outcomes of pregnancy and childbirth at the population level. They serve three inter-related functions in clinical practice. First, they provide epidemiological benchmarks: a facility's maternal mortality ratio can be compared against district, state, or national figures to identify whether care quality is above or below expectation. Second, they drive accountability — national programmes like Janani Suraksha Yojana (JSY) and Janani Shishu Suraksha Karyakram (JSSK) are evaluated precisely against trends in these indicators. Third, they are the trigger for clinical audit: every maternal death must be reviewed under India's Maternal Death Review (MDR) programme, and every perinatal death enters a structured perinatal mortality audit. The indicators studied today — covering maternal mortality and morbidity, perinatal and neonatal mortality, stillbirth, and abortion — are the core vocabulary you will use throughout your career in obstetrics and gynaecology.
These statistics are collected through two principal systems in India. The Sample Registration System (SRS), operated by the Office of the Registrar General of India, provides annual national and state-level data on births, deaths, and cause-specific rates including the MMR and infant mortality rate (IMR). The Health Management Information System (HMIS) of the Ministry of Health and Family Welfare captures facility-level data on deliveries, complications, and deaths from all government health institutions. Together, these systems form the data backbone for planning, monitoring, and evaluation of maternal and child health programmes.
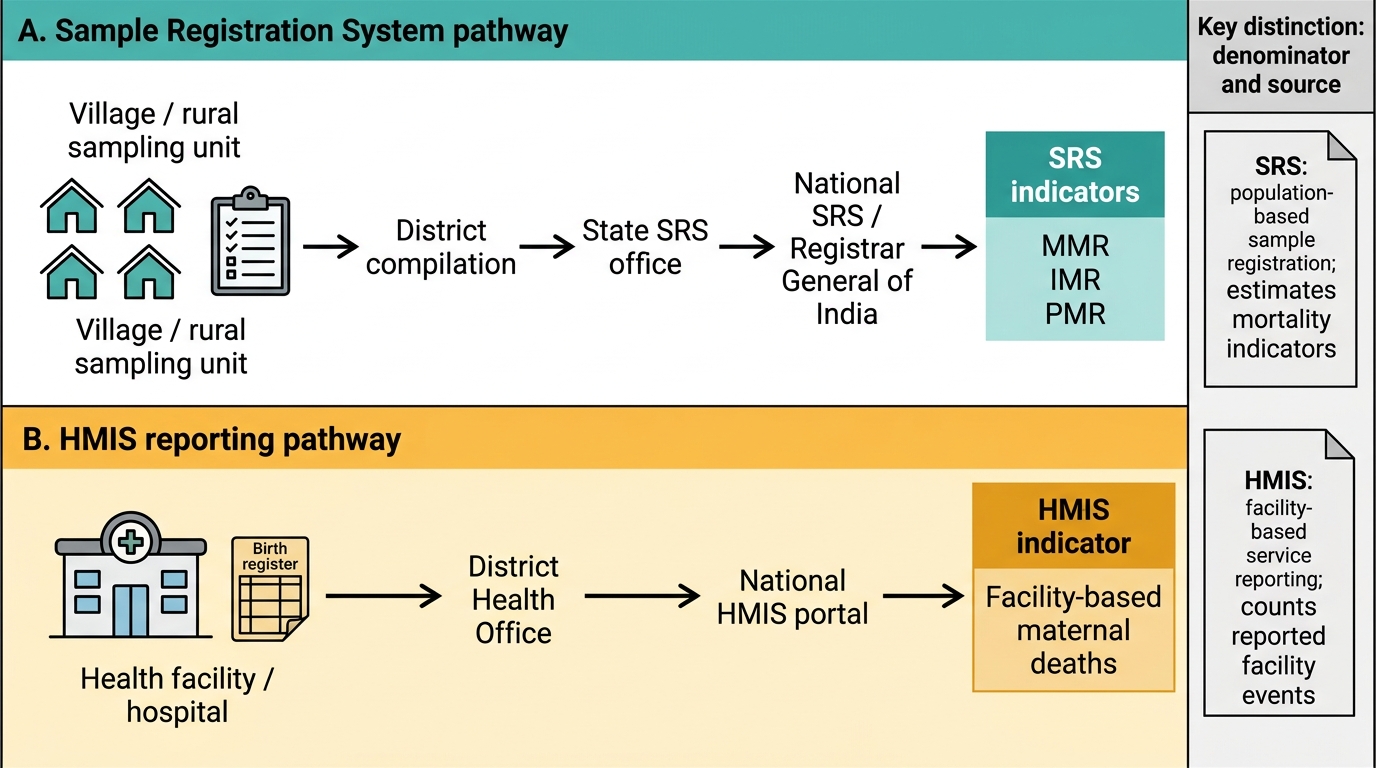
Data Flow in India's Vital Statistics System
Understanding why different indicators use different denominators is foundational. Denominators are chosen to reflect the population actually at risk of the event being measured. Maternal deaths occur in women who are pregnant or recently delivered — so live births (the proxy for completed pregnancies) form the denominator for MMR, not total population. Women of reproductive age carry the cumulative risk of pregnancy across their fertile life, so maternal mortality rate uses that denominator. This distinction matters when comparing across populations with very different fertility rates.
Maternal Mortality: Definitions and Measurement
A maternal death is defined by the World Health Organization as the death of a woman while pregnant or within 42 days of termination of pregnancy, irrespective of the duration and site of the pregnancy, from any cause related to or aggravated by the pregnancy or its management — but NOT from accidental or incidental causes. This 42-day window reflects the period during which pregnancy-specific physiological changes and their complications can still cause death. Deaths beyond 42 days but within one year of delivery may be captured as late maternal deaths for surveillance purposes, but these do not enter the standard MMR numerator.
Maternal deaths are classified into two broad categories. Direct obstetric deaths result from obstetric complications of the pregnant state itself — haemorrhage, hypertensive disorders (pre-eclampsia/eclampsia), sepsis, obstructed labour, and complications of unsafe abortion account for the vast majority. Indirect obstetric deaths result from previously existing disease or disease developing during pregnancy that is not due to direct obstetric causes but is aggravated by the physiological effects of pregnancy — anaemia, cardiac disease, diabetes, and tuberculosis are the leading indirect causes in India. A death from a road-traffic accident during pregnancy is neither direct nor indirect and does not enter the maternal death numerator.
The two principal maternal mortality indicators are:
- Maternal Mortality Ratio (MMR) = (Number of maternal deaths in a given period) ÷ (Number of live births in the same period) × 100,000. The denominator is live births, which serves as a proxy for the number of women exposed to the risk of maternal death through pregnancy and delivery. The multiplier is 100,000 (not 1,000). India's MMR was 97 per 100,000 live births (SRS 2018–20), down from 130 in 2014–16. The SDG target is fewer than 70 by 2030.
- Maternal Mortality Rate = (Number of maternal deaths) ÷ (Number of women aged 15–49 years) × 1,000. This uses women of reproductive age as the denominator and reflects the overall risk of maternal death across the entire reproductive-age population, not just those who became pregnant. It is less commonly used in clinical audit but provides a population-level burden estimate.
Lifetime risk of maternal death is the probability that a 15-year-old girl will eventually die from a maternal cause; it combines the per-pregnancy risk (MMR) with the total fertility rate. In high-fertility, high-MMR settings, lifetime risk can exceed 1 in 20.

Provided image
Maternal Morbidity and Near-Miss Surveillance
Maternal morbidity encompasses any condition or complication arising during pregnancy, delivery, or the puerperium that has a negative effect on the woman's wellbeing. The severity spectrum ranges from minor complications (e.g., gestational hypertension without features of severity) through significant morbidity (e.g., severe anaemia requiring transfusion, wound dehiscence) to life-threatening conditions (e.g., uterine rupture, disseminated intravascular coagulation). Tracking maternal morbidity data alongside mortality reveals the 'tip of the iceberg' problem: for every maternal death, estimates suggest dozens of women experience near-fatal complications without dying.
The maternal near-miss concept was formalised by the WHO in 2011 to capture precisely this group — women who nearly died but survived a severe acute complication during pregnancy, childbirth, or within 42 days of termination of pregnancy. The WHO near-miss criteria are organ-dysfunction-based and are defined at a specific clinical threshold: a woman meets near-miss criteria if she has at least one of the defined markers of severe organ dysfunction (cardiovascular, respiratory, renal, coagulation, hepatic, neurological, or uterine dysfunction) while being treated in an intensive care setting. Specific WHO markers include: inability to maintain mean arterial pressure >50 mmHg, oxygen saturation <90% for ≥60 minutes, creatinine ≥300 µmol/L, severe thrombocytopaenia (<50,000/µL), jaundice in the presence of pre-eclampsia, loss of consciousness >12 hours, and stroke. The advantage of the near-miss framework is that it captures preventable near-fatalities that represent system failures — the same system failures that, in another patient or at another facility, would have resulted in a death.
The Maternal Near-Miss Ratio = (Number of near-miss cases) ÷ (Number of live births) × 1,000. A complementary metric is the Severe Maternal Outcome Ratio = (Near-miss + maternal deaths) ÷ live births × 1,000. The Mortality Index = (Maternal deaths) ÷ (Near-miss + maternal deaths) × 100 — a high mortality index (e.g., >20%) indicates that most women with life-threatening complications are dying rather than surviving, suggesting inadequate emergency obstetric care. Under India's Maternal Death Review programme, health facilities are mandated to notify and review all maternal deaths occurring in their institution within 24 hours, and increasingly, near-miss cases are reviewed alongside deaths to capture a wider set of learning opportunities for quality improvement.
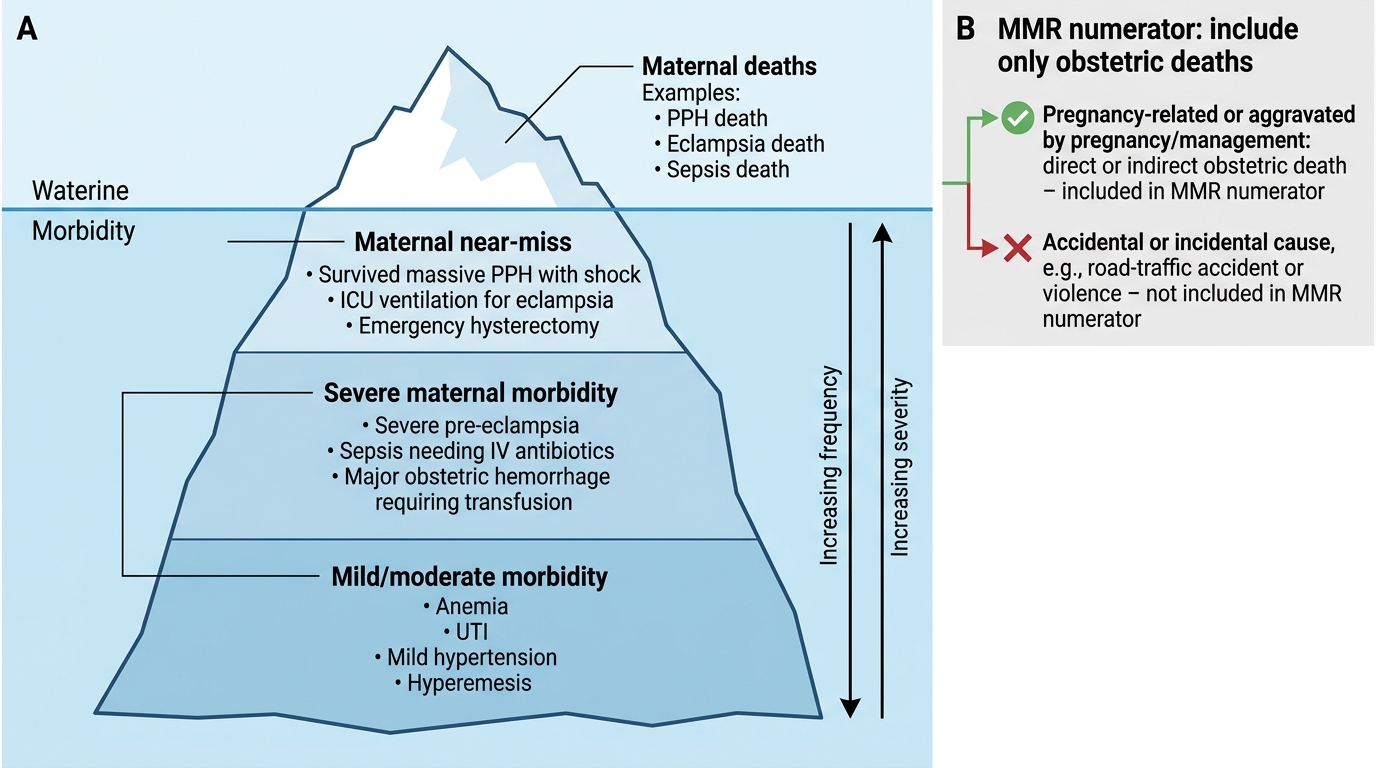
Maternal Morbidity Spectrum as an Iceberg
SELF-CHECK
A 28-year-old woman, 36 weeks pregnant, dies in a road-traffic accident. Which statement about classifying her death is correct?
A. It is a direct obstetric death and enters the MMR numerator
B. It is an indirect obstetric death and enters the MMR numerator
C. It is an accidental death and does NOT enter the MMR numerator
D. It is a late maternal death and enters a separate surveillance category
Reveal Answer
Answer: C. It is an accidental death and does NOT enter the MMR numerator
A maternal death is classified as obstetric only when the cause is related to or aggravated by pregnancy or its management. Deaths from accidental causes (road-traffic accidents, violence) are neither direct nor indirect obstetric deaths and do not enter the MMR numerator, even though the woman was pregnant.