Page 5 of 32
OG17.2 | Breastfeeding Counselling — SDL Guide
Learning Objectives
- Identify women who require breastfeeding counselling and the optimal timing of counselling interventions
- Describe the anatomical basis for effective latch and the mechanical principles of milk extraction by the infant
- Demonstrate the four standard breastfeeding positions (cradle, cross-cradle, football, side-lying) and state the indication for each
- Describe the steps for achieving and correcting a correct latch, including recognition of a good versus poor latch
- Counsel a mother on breast care including nipple soreness prevention, engorgement management, and hand expression
- Apply the LATCH assessment tool and identify signs of effective and ineffective breastfeeding
- Counsel mothers in a simulated environment using appropriate communication skills, addressing common misconceptions and cultural barriers
INSTRUCTIONS
Breastfeeding is a learned skill — for both mother and infant. Most breastfeeding problems that lead to early cessation are preventable or correctable with timely, skilled counselling. This module builds on the physiology of lactation to equip you with the practical skills of breastfeeding support: how to position mother and baby, how to achieve and correct a latch, how to assess feeding effectiveness, and how to counsel mothers with sensitivity and evidence. These are skills assessed in OSCE-format examinations and practised daily on postnatal wards.
References
- DC Dutta's Textbook of Obstetrics, 9th ed., Ch. 17 — Lactation and Breastfeeding (textbook)
- WHO/UNICEF, Counselling on Infant and Young Child Feeding (IYCF) Counselling Cards, 2010 (guideline)
- National Guidelines for Lactation Management, Government of India / NHM, 2017 (guideline)
- Riordan & Wambach, Breastfeeding and Human Lactation, 5th ed. — Positioning and Latch (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are a house officer on the postnatal ward. A 22-year-old primipara on day 2 postpartum is in tears. She says: 'The baby won't latch, my nipples are cracked and bleeding, and I think I have no milk. My mother-in-law says I should just give formula.' The nursing staff report the baby has had only three wet nappies since birth. How do you respond? This scenario — common in any Indian maternity hospital — demands more than pharmacological knowledge: it requires a structured approach to positioning and latch assessment, ability to identify correctable technique errors in real time, and communication skills that are empathetic, evidence-based, and culturally sensitive.
WHY THIS MATTERS
Breastfeeding initiation and continuation rates in India remain suboptimal despite clear evidence of benefit. The primary reason women stop breastfeeding in the first month is not insufficient milk — it is pain, poor positioning, and lack of skilled support at the critical window when feeding is being established. As a final-year student and future clinician, your counselling skills directly determine whether a mother continues breastfeeding through the first challenging days. Beyond individual patients, the OSCE skill assessment for this competency (OG17.2) requires you to demonstrate correct technique in a simulated environment. Getting these skills right is simultaneously evidence-based medicine, communication medicine, and examination preparation.
RECALL
Activate prior knowledge before proceeding:
- Lactation physiology (og10-lactation-physiology): Milk ejection depends on the oxytocin let-down reflex, which is initiated by suckling and inhibited by pain and stress — poor latch causes pain, which inhibits let-down, which reduces milk transfer, which undermines galactopoiesis.
- Mammary anatomy: Alveoli → lobules → lactiferous ducts → lactiferous sinuses → nipple. The myoepithelial cells surrounding alveoli contract under oxytocin. The nipple-areola complex is the zone the infant must engage deeply.
- Colostrum (first 2–3 days): Small volumes (2–10 mL per feed) are normal and appropriate. The mother's complaint of 'no milk' in the first 48 hours usually means lactogenesis II has not yet begun — reassurance and technique correction are the intervention.
- BFHI Step 7: Supporting mothers to manage common breastfeeding difficulties — this is the institutional mandate for the counselling you are learning.
Clinical Indication: Who Needs Breastfeeding Counselling and When
Breastfeeding counselling is indicated for all postpartum mothers, not only those who present with problems. The evidence base for universal, proactive support — beginning antenatally and continuing through the first weeks postpartum — is consistent: Cochrane reviews confirm that both skilled professional support and lay peer support significantly increase breastfeeding initiation and duration rates. The timing of counselling is as important as its content. Interventions delivered at the right moment — before problems arise, or in the critical first hour after birth — are far more effective than reactive advice given after a mother has already decided to stop, after engorgement has become severe, or after formula supplementation has already blunted the prolactin reflex. A structured, proactive, time-anchored counselling programme — beginning antenatally and continuing through the early postnatal period — is therefore the standard of care rather than crisis-driven support.
All postpartum women should receive:
- Antenatal preparation (from 36 weeks): realistic expectations about colostrum, timing of milk 'coming in', positioning options, and access to support
- Immediate postpartum support (within the first hour of birth): initiation of skin-to-skin contact and the first breastfeed (BFHI Step 6)
- Day 1–2 postnatal ward support: positioning, latch assessment, LATCH scoring, engorgement anticipation
- Day 3–5 follow-up: assessment after lactogenesis II onset, management of engorgement and early nipple problems
- Discharge counselling: signs of adequate feeding, when to seek help, community support resources
High-priority groups who require more intensive and proactive counselling include:
- Primiparae — no previous breastfeeding experience; highest risk for early cessation
- Women with flat or inverted nipples (grades I–III) — latch technique needs modification; nipple formers or breast shields may be needed antenatally
- Mothers of preterm or low-birth-weight infants — infant may have weak or absent suckling reflex; expressing and cup-feeding are bridge strategies
- Mothers who have had caesarean sections — delayed skin-to-skin; side-lying or football hold reduces incision discomfort
- Women with previous breastfeeding difficulty or previous breast surgery
- Socioeconomically vulnerable women or those with strong family pressure toward formula use — requires culturally sensitive, non-judgemental communication
Anatomy and Principles of Effective Breastfeeding
A clear understanding of the anatomical mechanics of breastfeeding prevents the most common counselling errors — most notably the instruction to 'put the baby to the nipple', which is anatomically incorrect and leads to nipple damage and poor milk transfer.
The infant does NOT feed from the nipple alone. Effective milk extraction requires the infant to take a substantial mouthful of the nipple-areola complex — the nipple is drawn deep into the infant's mouth, beyond the hard palate junction, while the jaws compress the areola and underlying lactiferous sinuses. The tongue plays the primary extractive role: it moves in a peristaltic wave, compressing the lactiferous sinuses from their base toward the nipple, stripping milk forward. The soft palate seals around the nipple above, creating negative intraoral pressure that further draws milk. This is why the latch must be deep and asymmetric — more areola should be visible above the infant's upper lip than below the lower lip (the lower jaw should be closer to the base of the nipple than the upper jaw).
The myoepithelial cells surrounding the alveoli contract in response to oxytocin (released by suckling stimulation of the nipple-areola), ejecting milk into the ducts. However, myoepithelial contraction alone is insufficient without the mechanical extraction action of the infant's tongue — both the let-down reflex AND effective tongue mechanics are required for complete milk transfer.
Nipple variations affect latch technique:
- Protractile (normal) nipples: protrude easily when the areola is compressed; standard technique applies
- Flat nipples: do not protrude with compression; respond to nipple rolling exercises, breast shells worn in late pregnancy, or cold-stimulation immediately before feeding
- Inverted nipples (Grade I): protrude with stimulation; most improve with early latching
- Inverted nipples (Grade II/III): retract actively; may require nipple formers (worn 30 min before feeds), nipple shields, or expressing and cup-feeding temporarily
IMARK: Breast size has no relationship to milk-producing capacity — the relevant anatomy is alveolar density and duct patency, not adipose volume.
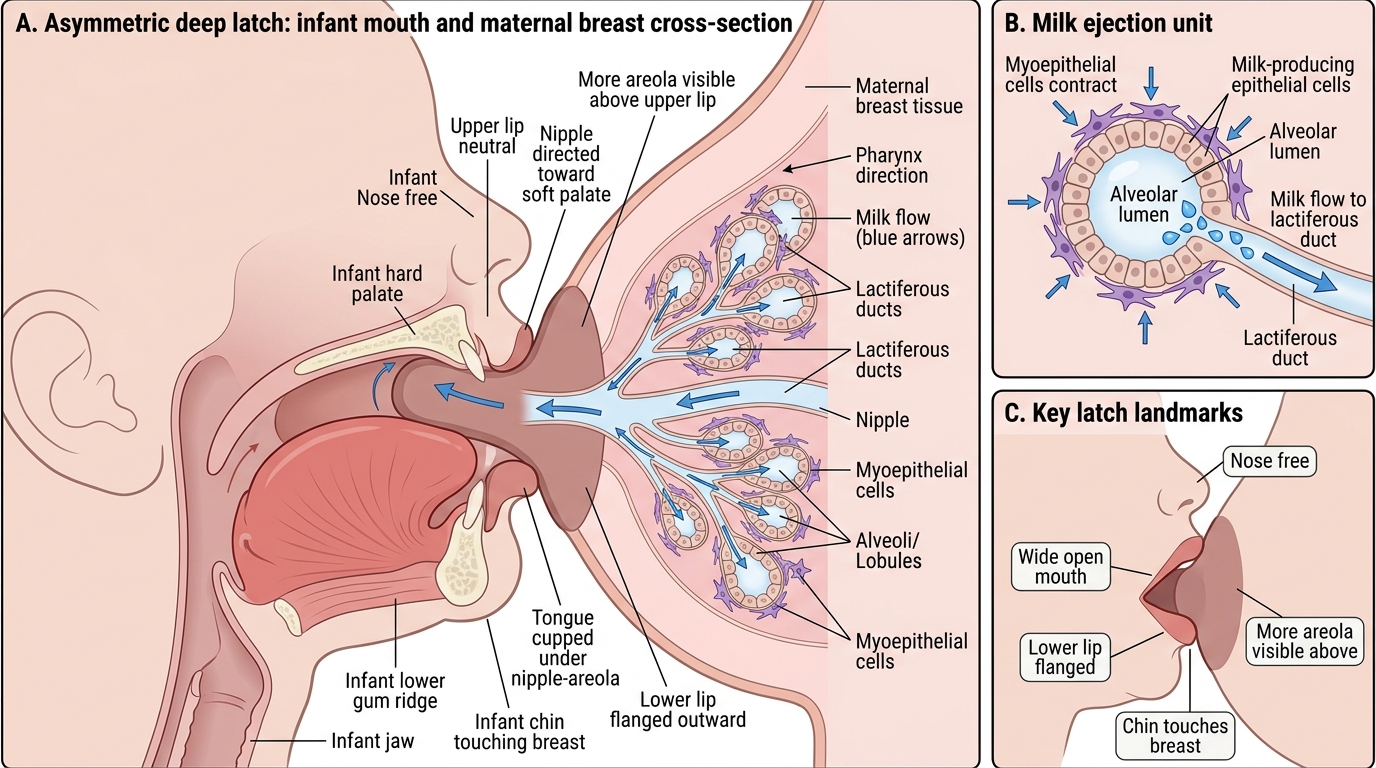
Asymmetric Deep Latch and Milk Transfer During Breastfeeding
Positioning the Mother and Baby: The Four Standard Holds
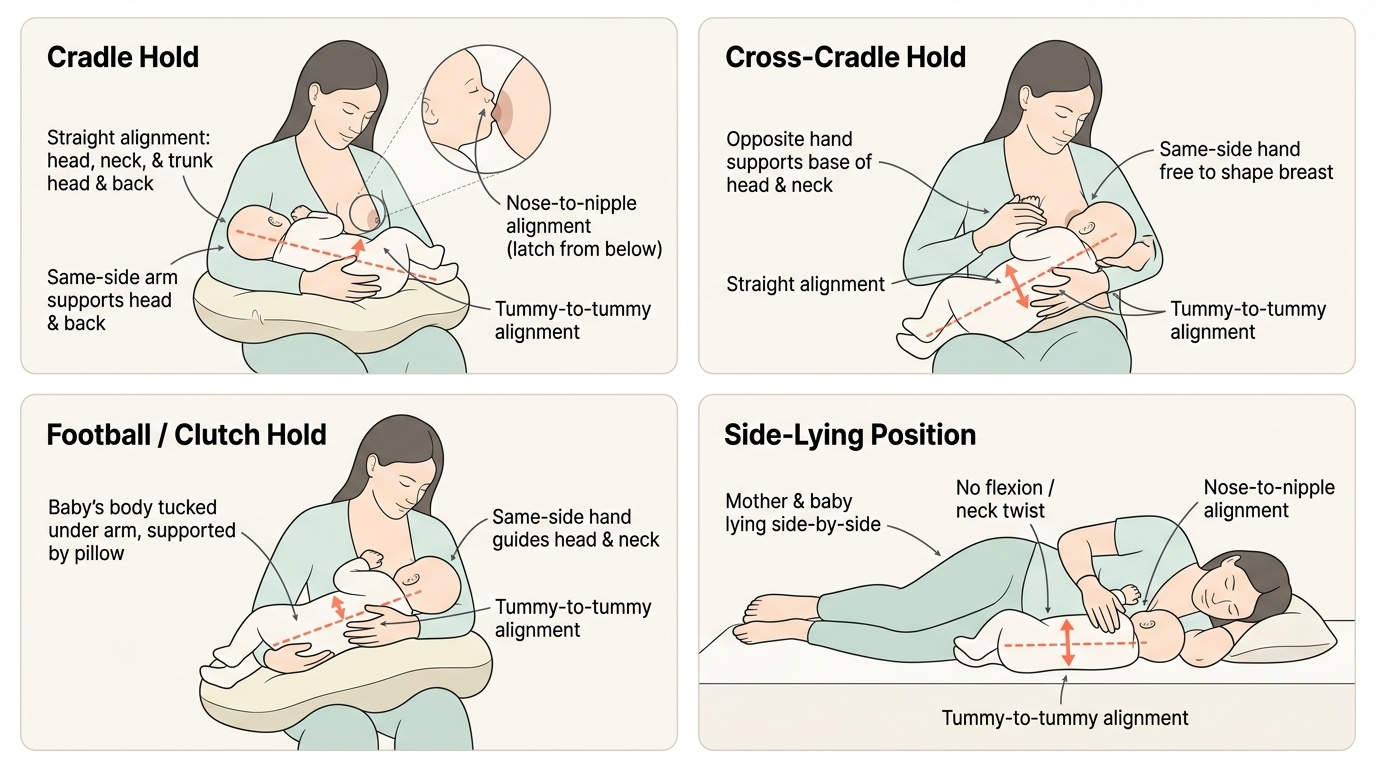
Correct positioning is the foundation of effective breastfeeding. Poor position is the most common root cause of poor latch, which in turn causes nipple trauma, poor milk transfer, and the cascade toward early cessation. The overarching anatomical principle common to all positions is tummy-to-tummy alignment: the infant's body should face the mother's body squarely, with no head-turning to the side (which closes the infant's airway and makes swallowing difficult). The infant's head, neck, and trunk should be in a straight line — no neck flexion or extension.
Four standard breastfeeding positions:
1. Cradle hold: The most commonly adopted position after the first days. The infant lies horizontally across the mother's body, head resting in the crook of the arm on the same side as the breast being used. The mother's forearm supports the infant's back; the hand supports the baby's bottom. The nipple faces the infant at nose level (not mouth level) so the infant latches from below, chin-first.
2. Cross-cradle hold: Particularly useful for newborns and for learning to latch. The infant is held with the opposite arm to the breast being used — e.g., feeding from the right breast, the left hand and forearm support the infant, with the left hand supporting the infant's head and neck (not pushing the head onto the breast — supporting it). The right hand is free to shape the breast. This position gives maximum control and is ideal for the first days and for primiparae.
3. Football (clutch) hold: The infant's body is tucked under the mother's arm on the same side as the feeding breast, like carrying a football, with the infant facing upward and the mother's hand supporting the head. Particularly useful after caesarean section (avoids abdominal wound pressure), for women with large breasts (better control), for twins (simultaneous feeding), and for premature infants (better head control).
4. Side-lying position: Both mother and infant lie on their sides facing each other. Particularly useful for night feeds, after perineal trauma (avoids sitting pain), and after caesarean section. Requires care to ensure the infant is not partially covered by bedding (safe-sleep principles).
In all positions, the mother should support the breast in a C-hold (thumb above, four fingers below) or U-hold, ensuring fingers are well behind the areola (not on the areola, which compresses the ducts and impedes latch depth). The scissors grip (two fingers straddling the nipple) is discouraged as it limits the tissue available for the infant's mouth.
Provided image