Page 18 of 32
OG18.{2,4} | Neonatal Resuscitation — SDL Guide (Part 3)
Simulation Practice and Supervised Skill Consolidation
The OG-skills arc recognises that reading about neonatal resuscitation and PERFORMING it reliably under the physiological stress of a real emergency are fundamentally different cognitive and psychomotor challenges. Cognitive knowledge — knowing that PPV should be started if HR is below 100 — is a necessary but insufficient condition for competent action at the resuscitation warmer. Under stress, without prior motor rehearsal, even well-memorised protocols break down: hands fumble with the mask, the sequence is reversed, the 3:1 ratio reverts to the more-practised 30:2. Simulation-based deliberate practice is the evidence-supported bridge between knowing and doing. It allows you to make mistakes in a controlled environment where the cost of error is feedback rather than harm, and to repeat the sequence until it becomes procedurally automatic. For competency OG18.2, the NMC specifies demonstration in a simulated environment — this is not merely a training convenience but the PRESCRIBED level of attainment for this skill. In India, the Federation of Obstetric and Gynaecological Societies of India (FOGSI) and the National Neonatology Forum (NNF) have both incorporated HBB simulation training into their faculty-development and intern-training programmes, reflecting national consensus that simulation is the route to preparedness for birth attendants at all levels.
At the skill station, your practice session should cover:
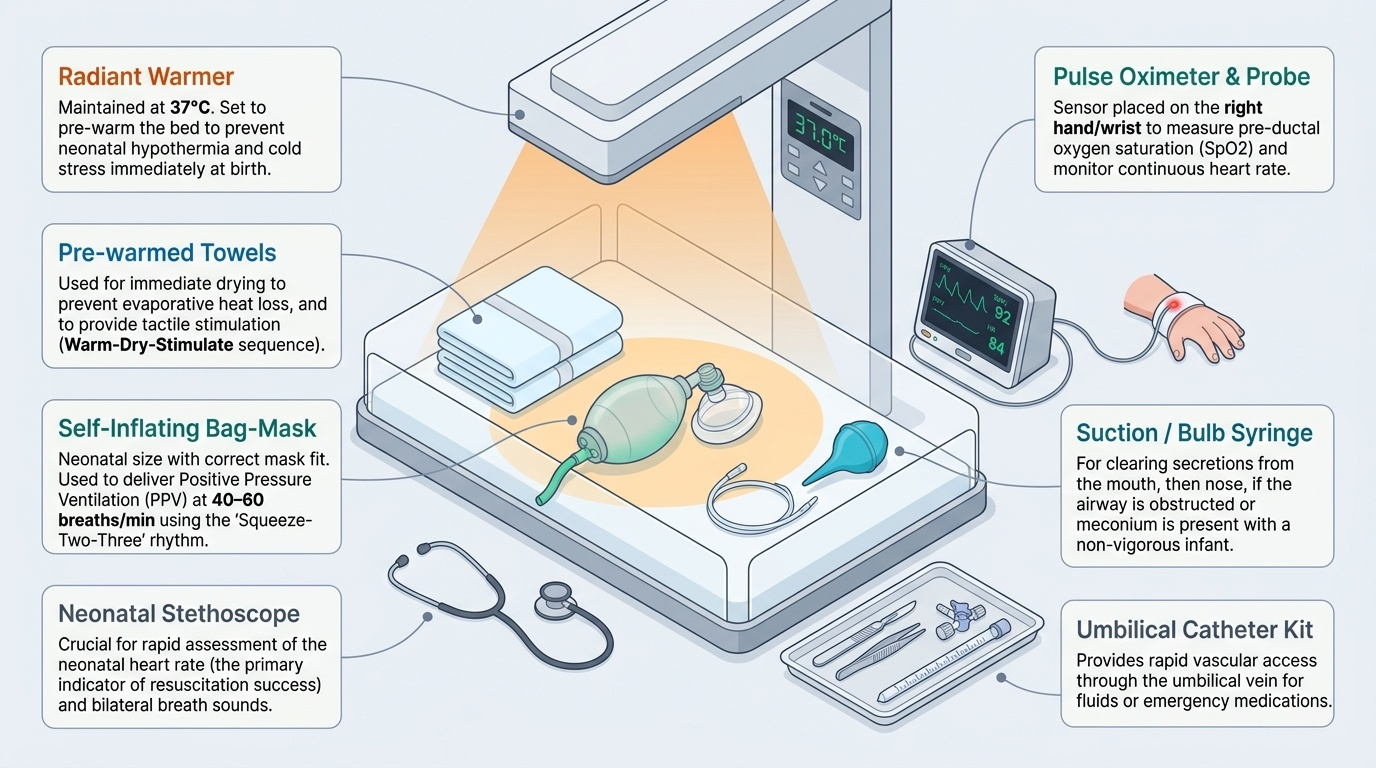
1. Equipment check (pre-delivery drill): radiant warmer set to 37°C, towels pre-warmed, bag-mask device (self-inflating recommended for initial training) with correct neonatal mask size selected and seal tested, suction source and bulb syringe, stethoscope, pulse oximeter, umbilical catheter kit available.
2. Initial steps run-through: practice the rapid WARM-DRY-STIMULATE-REPOSITION sequence on the mannequin within 30 seconds.
3. PPV drill: practice correct mask application and seal, sniffing position, and the 'Squeeze-TWO-THREE' rhythm at 40–60/min; watch for chest rise; practise the MR SOPA troubleshooting sequence if no chest rise (Mask seal → Reposition → Suction → Open mouth → Pressure increase → Alternative airway).
4. Compressions drill: two-thumb encircling technique, lower-third sternum, 3:1 ratio coordination with a partner ventilating.
5. Meconium scenario: practise the decision-making tree for vigorous vs non-vigorous baby with MSAF.
Common errors observed in simulation, which you should consciously guard against:
• Over-extending the neck (hyperextension closes the airway in neonates)
• Not checking chest rise before troubleshooting
• Forgetting to switch from chest compressions back to PPV-only when HR recovers to ≥60
• Applying adult 30:2 ratio — this error is common in students who have recently practiced adult BLS
• Not calling for help early
Debriefing rule: after every simulation run, use the Plus-Delta method — what went well (plus), what would you change (delta). Honest self-appraisal is the mechanism for skill improvement.
Provided image
CLINICAL PEARL
The most common reason PPV fails to raise the heart rate in simulation AND clinical practice is a LEAKY MASK SEAL, not inadequate pressure. Before increasing pressure (which risks pneumothorax) or moving to intubation, methodically check the MR SOPA sequence: Mask seal → Reposition head → Suction → Open mouth → Pressure up → Alternative airway. In resource-limited settings, a self-inflating bag functions without a gas source, making it more reliable during power failures; however, it cannot deliver a sustained positive end-expiratory pressure (PEEP) — so for preterm infants requiring PEEP, a T-piece resuscitator or flow-inflating bag is preferred where available.
SELF-CHECK
Which of the following correctly describes the neonatal compression-to-ventilation ratio in CPR?
A. 30:2 (same as adult single-rescuer CPR)
B. 15:2 (same as two-rescuer paediatric CPR)
C. 3:1, providing approximately 30 compressions and 10 ventilations per minute
D. 5:1, providing approximately 50 compressions and 10 ventilations per minute
Reveal Answer
Answer: C. 3:1, providing approximately 30 compressions and 10 ventilations per minute
Neonatal CPR ratio is 3:1, yielding ~90 compressions + 30 ventilations per minute. This differs from both adult single-rescuer (30:2) and two-rescuer paediatric (15:2) protocols. The higher relative ventilation rate reflects that neonatal arrest is almost always hypoxia-driven, making oxygenation proportionally more critical per cycle.
Self-Assessment: Consolidating Your Neonatal Resuscitation Knowledge
Before you proceed to the skill station and before you encounter a real resuscitation, this self-assessment step asks you to verify your cognitive readiness across all six domains covered in this module. Research on skill acquisition consistently shows that passive re-reading produces an illusion of competence — you recognise content when you see it but cannot recall it when faced with the warmer and a non-breathing baby. Active self-testing, by contrast, strengthens retrieval pathways and reveals genuine gaps while the cost of discovery is still zero. A confident, unprompted answer to each of the questions below indicates you have internalised the framework at the level required for simulation and subsequent supervised practice; uncertainty in any domain is valuable diagnostic information, not failure — it tells you exactly where to re-read, ask a faculty supervisor, or request an additional practice run before the OSCE.
Work through these questions aloud or in writing — from memory, not by re-reading the sections above — since memory retrieval is the only condition that approximates the real clinical scenario:
- Indication: State the exact HR threshold and breathing criterion that trigger PPV. What are the three questions you answer at birth to decide whether the baby needs the resuscitation warmer?
- Physiology: Why does adequate ventilation — rather than chest compressions — reverse most neonatal arrests? Connect your answer to the fetal-to-neonatal transition physiology.
- Procedure: Describe the WARM-DRY-STIMULATE-REPOSITION sequence and explain the anatomical reason for 'sniffing position' rather than full head-tilt.
- Ratio: State the neonatal CPR ratio and distinguish it explicitly from the adult and two-rescuer paediatric ratios. Give the rationale in one sentence.
- Meconium: Describe the decision tree for MSAF. What changed in NRP guidance and why? What do you do if intubation skills are not available?
- Assessment: Name the five Apgar parameters. At what time points is it scored? Why is it described as retrospective rather than prospective?
If you can answer all six confidently, you are ready for the skill station. If not, identify the gap, return to the relevant section, and re-test yourself before the session.
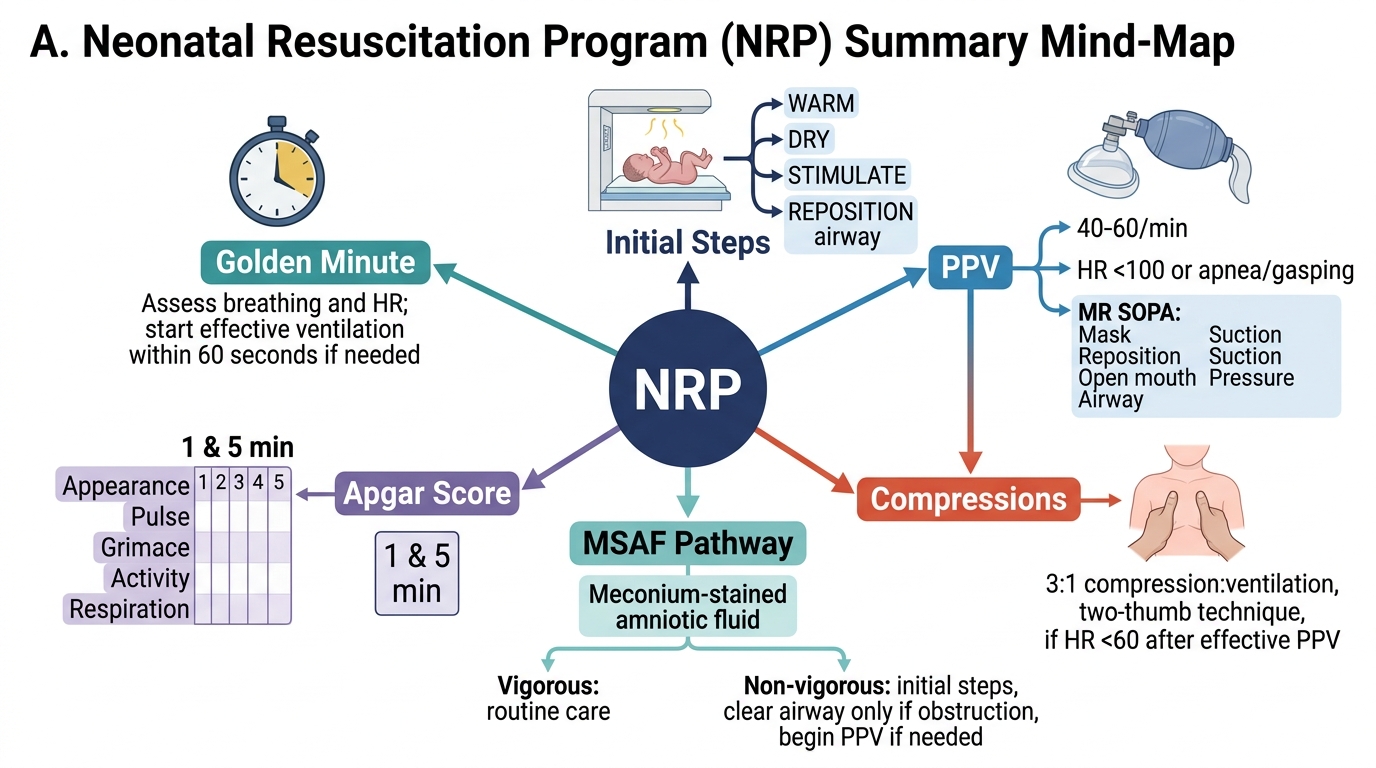
NRP Neonatal Resuscitation Summary Mind-Map