Page 20 of 32
OG19.1 | Normal and Abnormal Puerperium — SDL Guide
Learning Objectives
- Describe the physiological changes of the normal puerperium including uterine involution, lochia progression, cervical changes, and perineal healing
- Define puerperal pyrexia and enumerate the differential diagnosis systematically by day of onset
- Describe the pathophysiology, causative organisms, clinical features, and management of puerperal sepsis
- Identify the causes, assessment, and management of secondary postpartum haemorrhage and subinvolution
- Distinguish puerperal blues, postpartum depression, and puerperal psychosis and outline the management of each
- Counsel a woman on the normal puerperium, warning signs, and contraceptive options before discharge
INSTRUCTIONS
The puerperium — the six weeks following delivery — is a period of profound physiological restoration for the mother, and also a window of significant vulnerability to complications that, if missed, carry high mortality and morbidity. This module follows the OG disease arc to take you from the clinical presentations that bring puerperal women back to hospital, through the underlying physiology and pathophysiology, to diagnosis and management. The competency (OG19.1) spans both normal physiology and its departures — master both together.
References
- DC Dutta's Textbook of Obstetrics, 9th ed., Ch. 14 — The Puerperium (textbook)
- Shaw's Textbook of Gynaecology, 16th ed. (textbook)
- Williams Obstetrics, 25th ed., Ch. 36 — The Puerperium (textbook)
- RCOG Green-top Guideline No. 64b — Bacterial Sepsis Following Pregnancy (2012) (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Day 5 after a normal vaginal delivery, a 24-year-old primipara is brought to the emergency department by her family. She has been feverish since yesterday, has lower abdominal pain, and the family reports that her vaginal discharge has become 'foul-smelling.' On examination: temperature 39.2°C, pulse 112/min, BP 100/68 mmHg, uterus tender and soft on palpation. Her lochia has a fetid odour. What is happening, and what could go wrong in the next hour if you do not act?
WHY THIS MATTERS
Maternal mortality from puerperal causes remains a major contributor to India's maternal mortality ratio (MMR). The three direct obstetric killers worldwide — haemorrhage, hypertension, and sepsis — all have a postpartum phase. Puerperal sepsis, in particular, is responsible for approximately 10–15% of maternal deaths globally, and in India accounts for a substantial proportion of the 'puerperal complications' cluster in MMR reports. Beyond mortality, missed puerperal complications — undiagnosed secondary PPH, subinvolution from retained products, and untreated postpartum psychosis — cause avoidable morbidity and family disruption. As the doctor who conducts the discharge examination on day 2 or 3 after delivery, your ability to recognise the early signs of abnormal involution, pyrexia, and psychological distress determines whether these complications are caught in time. This module equips you with that clinical framework.
RECALL
Before we begin the arc, test your baseline. From your obstetrics and physiology modules: (1) What is the normal mechanism of placental separation and what prevents postpartum haemorrhage? (2) What hormonal changes drive uterine involution? (3) Where does the placental site scar form and how long does it take to fully epithelialise? (4) What triggers lactation and why do oxytocin-driven 'afterpains' occur during breastfeeding? Write brief answers before reading on — the physiology of normal puerperium underpins every complication we will discuss.
The Puerperal Patient: What Brings Her Back to the Ward
The puerperium is conventionally defined as the period from delivery of the placenta until six weeks (42 days) postpartum, during which the maternal reproductive organs and physiology return to their pre-pregnant state. The term derives from the Latin puer (child) + parere (to bring forth). This six-week window is clinically important because it encompasses both the rapid physiological restoration of the first two weeks and the more gradual hormonal and anatomical recovery of weeks three to six. For the clinician at the bedside, the puerperium is not a passive recovery period but a surveillance window: the major complications — sepsis, secondary haemorrhage, venous thromboembolism, and psychiatric breakdown — are all time-sensitive presentations whose outcome depends on early recognition. Knowing what is NORMAL at each stage makes the abnormal immediately apparent.
Women return to care in the puerperium for a defined set of clinical presentations, and recognising the pattern by day of onset is the foundation of differential diagnosis:
- Days 1–2: Primary postpartum haemorrhage (if unresolved from delivery), uterine atony, retained placental fragments, perineal/wound pain.
- Days 1–3: Breast engorgement, nipple trauma from breastfeeding initiation, afterpains (especially multiparae).
- Days 3–5: Puerperal blues (emotional lability, tearfulness) — normal variant; wound infection beginning (C/S or episiotomy); urinary tract infection (catheterisation-related).
- Days 5–10: Endometritis/puerperal sepsis — fever, uterine tenderness, offensive lochia; mastitis (particularly in breastfeeding women); deep vein thrombosis.
- Day 10 onwards: Secondary PPH (from retained products or infection); subinvolution; postpartum depression (emerging); puerperal psychosis (rare but emergency).
The single most important clinical question in every puerperal consultation is: Is the uterus involuting normally, and is the lochia normal in colour, quantity, and smell? These two parameters serve as the body's own monitoring system for the most common and dangerous puerperal complications.
Postpartum Uterine Involution and Lochia Timeline
SELF-CHECK
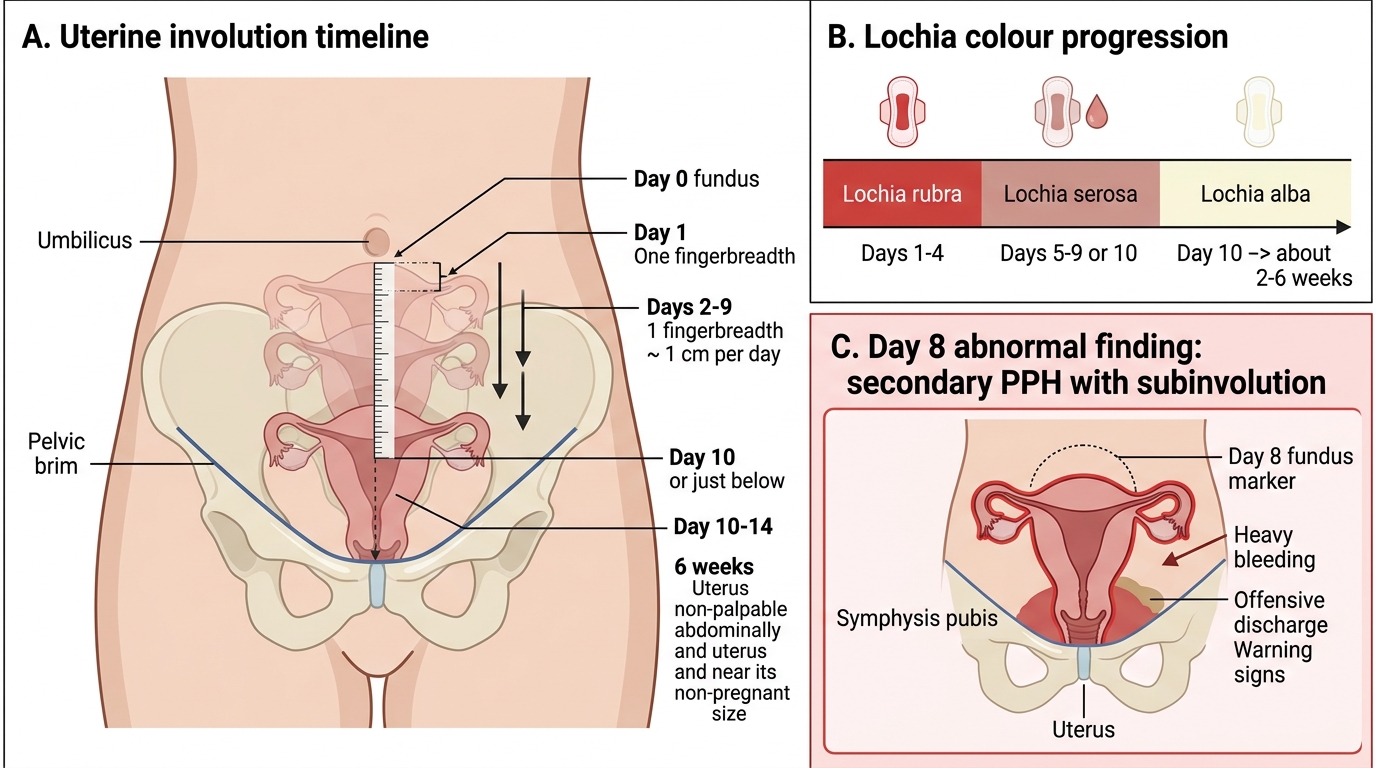
A woman at day 8 postpartum presents with per vaginal bleeding that is heavier than her normal period, offensive-smelling discharge, and a uterus that is palpable 4 cm above the symphysis pubis. What is the most likely diagnosis?
A. Normal lochia serosa
B. Primary postpartum haemorrhage
C. Secondary PPH with subinvolution, likely due to retained products of conception or infection
D. Puerperal psychosis
Reveal Answer
Answer: C. Secondary PPH with subinvolution, likely due to retained products of conception or infection
The uterus should be entering the pelvis by day 10 and non-palpable by 6 weeks — palpable at 4 cm above symphysis at day 8 is subinvolution. Heavy bleeding from 24 hours to 12 weeks is secondary PPH. The offensive odour points to infection or retained products (most common causes of subinvolution). Primary PPH is within 24 hours. Puerperal psychosis presents with psychiatric symptoms, not vaginal bleeding.
Physiology of the Normal Puerperium: Involution, Lochia and Healing
Uterine involution is the process by which the uterus, which weighs approximately 1,000 g immediately after delivery, returns to its non-pregnant weight of about 60–80 g by six weeks. This remarkable reduction is achieved through a combination of ischaemia and autolysis of the decidual and myometrial cells, proteolytic enzyme activity, and mechanical contraction driven by oxytocin (augmented by suckling during breastfeeding). Clinically, the uterine fundus is palpable at the level of the umbilicus immediately after delivery of the placenta. It then descends at approximately one fingerbreadth (1.25 cm) per day: at the symphysis-to-umbilicus midpoint by day 5, into the pelvis and no longer palpable abdominally by day 10–14. By six weeks, the uterus has returned to its pre-pregnant size. The rate of involution is monitored clinically at every postnatal check and is one of the earliest clinical indicators of complications.
Afterpains are intermittent, cramp-like uterine contractions in the first 2–3 days postpartum, more pronounced in multiparae (whose uterine tone is lower between contractions) and in breastfeeding women (suckling releases oxytocin from the posterior pituitary). They are normal and self-limiting but can be distressing enough to require paracetamol or NSAIDS.
Lochia is the vaginal discharge that results from the sloughing of the decidual layer and the gradual healing of the placental site. It progresses through three characteristic stages:
• Lochia rubra (red): days 1–4. Composed predominantly of blood, decidual debris, and fetal membranes. Normal to be moderately heavy, like a normal menstrual flow.
• Lochia serosa (pinkish-brown): days 5–9. The blood component diminishes; discharge becomes serosanguineous. Any return to bright-red flow at this stage suggests secondary PPH or subinvolution.
• Lochia alba (white/yellow): from day 10 onwards, lasting up to 4–6 weeks. Composed mainly of leucocytes, cervical mucus, and epithelial cells. A foul odour at any stage indicates infection.
Cervical and vaginal changes: The markedly oedematous, effaced cervix of labour closes progressively. The external os, which admits 2 fingers immediately post-delivery, narrows to admit 1 finger by 1 week and is functionally closed by 4 weeks. The internal os closes within a few days. The vaginal rugae, obliterated by the passage of the baby, begin to reform within 3 weeks.
Perineal healing: Episiotomies and perineal tears heal by primary intention. Oedema subsides within 72 hours, sutures are absorbed within 2–3 weeks, and most women report comfortable sitting by day 10–14. Wound infection or haematoma can complicate this process.
Return of menstruation: In non-breastfeeding women, the first menstrual period returns at 6–8 weeks. In exclusively breastfeeding women, prolactin-driven lactational amenorrhoea suppresses ovulation — but this is NOT a reliable contraceptive method without meeting all three LAM criteria (see og10-postpartum-contraception).
Puerperal Pyrexia: Causes, Assessment and Investigation
Puerperal pyrexia is classically defined as a temperature of 38°C (100.4°F) or above, occurring on any two of the first ten days postpartum, exclusive of the first 24 hours (the traditional Colebrook definition, adopted by RCOG). A pragmatic clinical approach treats any fever ≥38°C after the first 24 hours as requiring investigation. The first 24 hours are excluded because a transient temperature rise is common from the physiological inflammatory response to delivery and does not indicate pathology. The 'two days' criterion distinguishes a persistent infectious process from a transient physiological one.
The differential diagnosis of puerperal pyrexia is broad and must be approached systematically by organ system and day of onset. A useful mnemonic is the '5 Ws': Wind (respiratory — atelectasis, pneumonia, particularly after general anaesthesia), Water (urinary tract infection — very common post-catheterisation), Wound (episiotomy, C-section wound, perineal tears), Walking (deep vein thrombosis — calf pain, low-grade fever), and Womb/milk (endometritis/mastitis — the most dangerous). Some authorities add a sixth 'W' for 'Wonder drugs' (drug fever from antibiotics or methylergometrine).
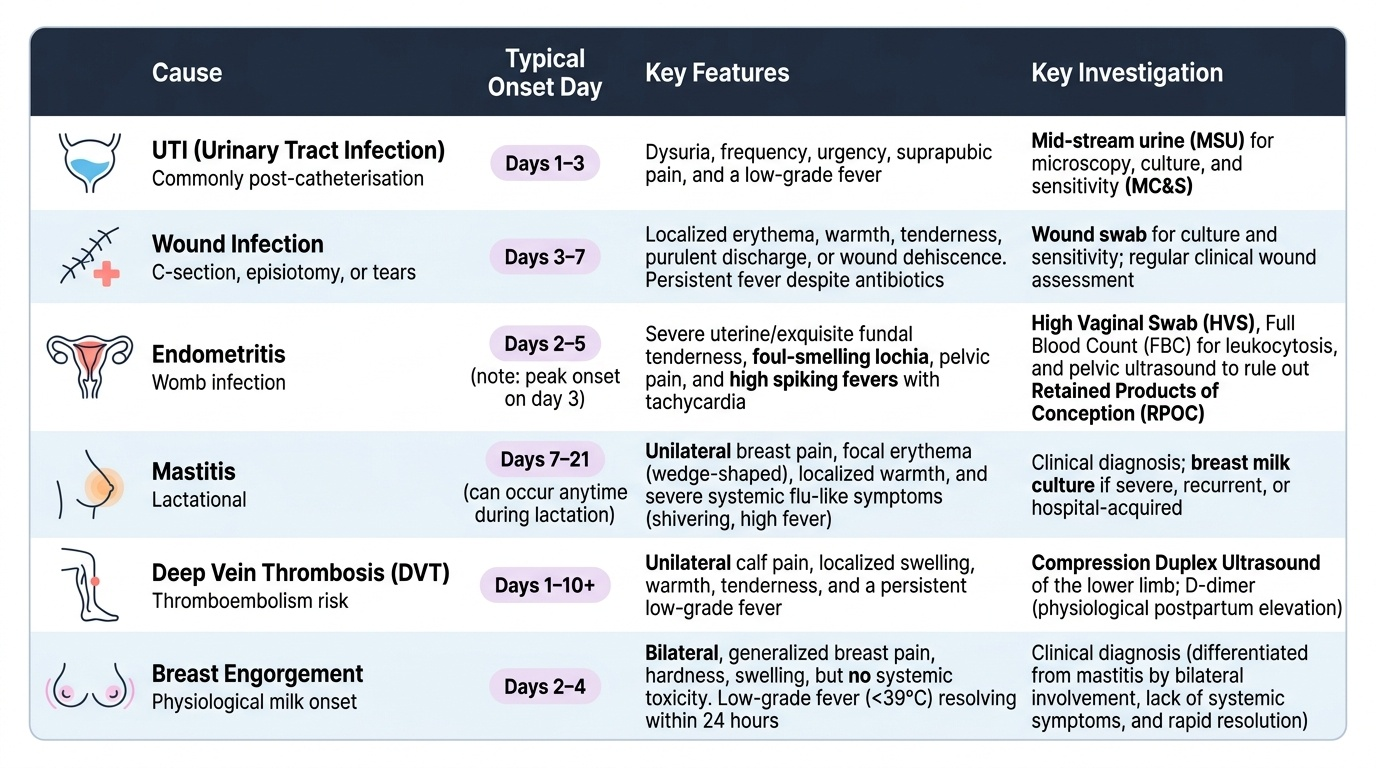
Provided image
Clinical assessment must include: temperature trend (sustained vs spiking), pulse (tachycardia out of proportion to temperature → sepsis), blood pressure, fundal height and tenderness (subinvolution + tenderness = endometritis), lochia (offensive odour, colour change), breast examination (localised induration, erythema = mastitis), wound inspection, calf tenderness, and respiratory examination. Investigations guided by the clinical picture include: full blood count (leucocytosis), blood cultures (before antibiotics), high vaginal swab, urine culture, wound swab, and Doppler ultrasound of lower limbs if DVT suspected. Pelvic ultrasound is performed to exclude retained products of conception when endometritis or subinvolution is present.