Page 14 of 28
OG21.2 | IUCD Insertion and Removal — SDL Guide
Learning Objectives
- Enumerate the indications and WHO MEC contraindications for IUCD insertion
- Describe the mechanism of action of copper-bearing (CuT 380A) and levonorgestrel-releasing (LNG-IUS) intrauterine devices
- Describe the step-by-step technique for IUCD insertion using the no-touch plunger-withdrawal method
- Describe the technique for IUCD removal, including management of missing threads
- Recognise and describe initial management of complications: expulsion, perforation, PID, and ectopic pregnancy
- Demonstrate IUCD insertion and removal in a simulated (task-trainer) environment
INSTRUCTIONS
Intrauterine contraceptive devices are among the most effective, reversible long-acting contraceptives available, with failure rates under 1% per year. Mastery of safe insertion and removal technique is a core clinical skill for any practitioner providing reproductive healthcare. This SDL prepares you to perform IUCD procedures in a simulated environment and to understand the clinical decision-making framework governing device selection, eligibility, and complication management. Work through each section sequentially; attempt every micro-quiz before reading the explanation.
References
- DC Dutta's Textbook of Gynecology, 8th ed., Ch. 30 (Contraception) (textbook)
- Jeffcoate's Principles of Gynaecology, 8th ed., Ch. 28 (textbook)
- WHO Medical Eligibility Criteria for Contraceptive Use (MEC), 5th ed., 2015 (guideline)
- Ministry of Health & Family Welfare, India — PPIUCD Reference Manual, 2010 (updated 2014) (guideline)
- Berek & Novak's Gynecology, 16th ed., Ch. 10 (Contraception) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 28-year-old woman, G2P2, delivered her second child 36 hours ago by normal vaginal delivery. She requests a reliable long-acting contraceptive before discharge and says she does not want another pregnancy for at least four years. She is breastfeeding. On counselling she expresses concern about remembering a daily pill and asks whether 'a device' can be placed now. Her uterine involution is satisfactory and there are no signs of infection. What device would you offer, when can it be inserted, and what must you explain before obtaining informed consent?
WHY THIS MATTERS
IUCDs are a cornerstone of India's family planning programme, accounting for the majority of long-acting reversible contraception (LARC) use in government facilities. The postpartum IUCD (PPIUCD) programme under the National Rural Health Mission has trained hundreds of thousands of providers because the post-delivery period is a uniquely high-motivation, high-clinical-contact moment for contraceptive uptake. As a graduating physician you will be expected to counsel couples on method eligibility, obtain informed consent, perform device insertion and removal in simulation, and recognise the uncommon but serious complications — perforation, ectopic pregnancy — that can follow a technique error or missed contraindication. Getting this skill right protects patients and enables you to provide equitable reproductive care across India's diverse practice settings.
RECALL
Before beginning, recall: (1) The layers of the uterine wall from lumen outward — endometrium, myometrium, perimetrium/serosa. (2) The internal os is the functional junction between the cervical canal and the uterine cavity; the cervical canal in the non-pregnant uterus is approximately 3–4 cm long. (3) Uterine sounding depth in a normal non-pregnant uterus is typically 6–9 cm from the external os to the uterine fundus. (4) The normal uterus is anteverted and anteflexed; the degree of flexion affects the angle of instrument passage. (5) Copper is spermicidal and impairs fertilisation; progesterone thickens cervical mucus, suppresses endometrium, and in higher doses inhibits ovulation. These anatomical and pharmacological anchors directly determine insertion technique and mechanism of action.
Clinical Indication and Patient Selection
Intrauterine contraceptive devices offer highly effective, reversible, long-term contraception and are appropriate for a broad range of patients. The choice between a copper-bearing IUCD (CuT 380A, effective up to 10 years) and a levonorgestrel-releasing intrauterine system (LNG-IUS, effective up to 5 years) depends on patient preference, breastfeeding status, and eligibility under the WHO Medical Eligibility Criteria (MEC). Broadly, IUCDs are indicated for women seeking long-acting reversible contraception who are not currently pregnant, have no active pelvic or cervical infection, and have no uterine anomaly distorting the cavity. They are particularly suited to women who want to space or limit further pregnancies without relying on user-dependent methods.
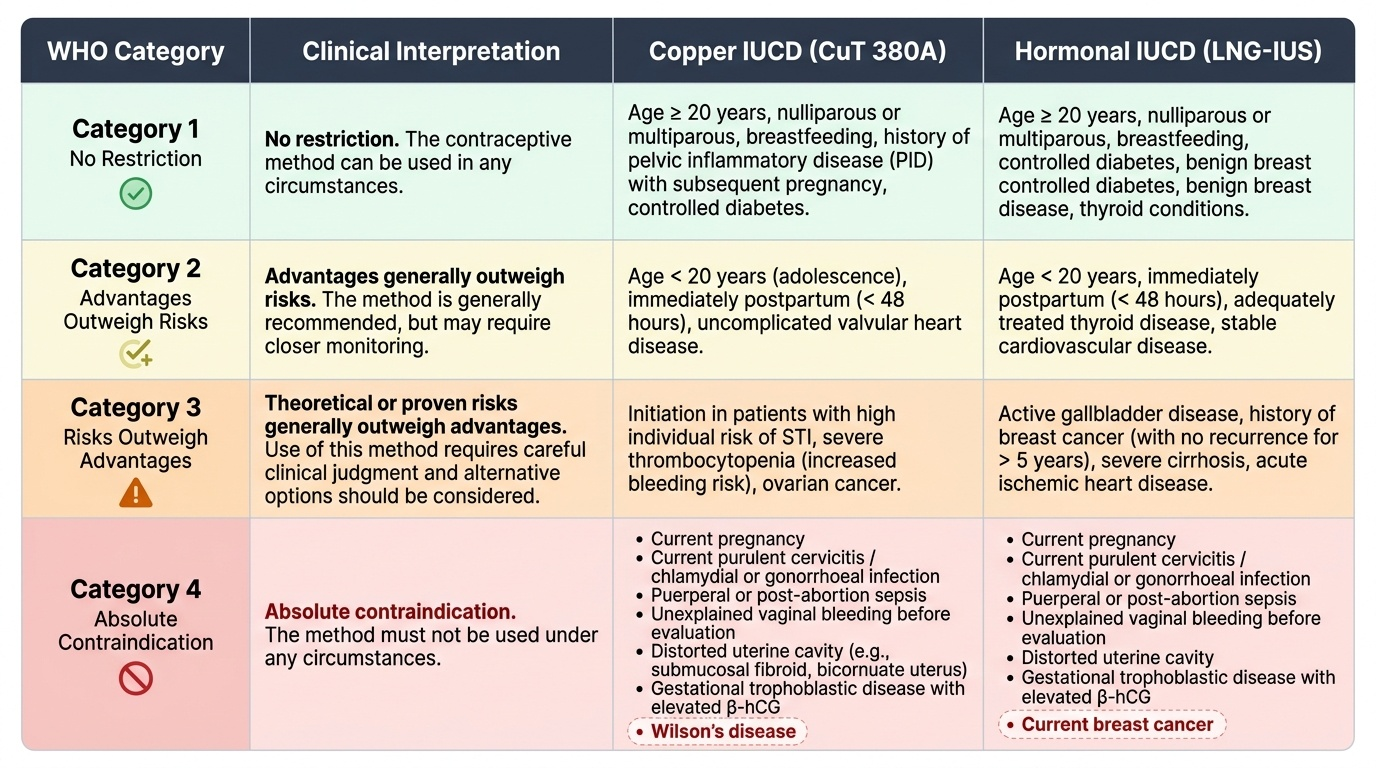
The WHO MEC classifies contraceptive eligibility across four categories: Category 1 (no restriction — use the method), Category 2 (advantages generally outweigh theoretical or proven risks), Category 3 (theoretical or proven risks generally outweigh advantages — use requires clinical judgement), and Category 4 (absolute contraindication — method must not be used). For both CuT 380A and LNG-IUS, WHO MEC 4 conditions include current pregnancy, current purulent cervicitis or chlamydial/gonorrhoeal infection, puerperal or post-abortion sepsis, unexplained vaginal bleeding before evaluation, distorted uterine cavity (e.g., submucosal fibroid, bicornuate uterus), and known or suspected gestational trophoblastic disease with elevated β-hCG. Additionally, copper IUCDs are WHO MEC 4 in women with Wilson's disease. The LNG-IUS carries an additional category 4 for current breast cancer.
Timing of insertion defines specific clinical windows. Interval insertion (outside the postpartum or post-abortion periods) is safest within the first 12 days of the menstrual cycle, when the woman is unlikely to be pregnant and the cervix is slightly more patent. Post-abortion IUCD can be inserted immediately after a complete first- or second-trimester abortion, provided there is no infection or haemorrhage. Post-partum IUCD (PPIUCD) is inserted either within 48 hours of delivery (immediate postpartum) while the uterus is still large and soft, making placement at the fundus technically easier, OR deferred until 4–6 weeks postpartum (interval). The 48-hour-to-6-week window carries higher expulsion risk and is generally avoided.
Pre-insertion counselling must cover: device types, duration of action, mechanism of action, expected changes in menstrual pattern (heavier bleeding with copper IUCDs; oligomenorrhoea/amenorrhoea possible with LNG-IUS), how to check threads, when to return for review (pain, fever, missing threads, pregnancy symptoms), and that the IUCD provides no protection against sexually transmitted infections. Informed written consent must be obtained and documented.
Provided image
SELF-CHECK
A 30-year-old woman with a history of Chlamydia trachomatis PID treated successfully 18 months ago, now with a new male partner who has been tested and is negative for STIs, requests a copper IUCD. She is currently asymptomatic with no discharge. What is the WHO MEC category for copper IUCD in this situation?
A. WHO MEC 4 — absolute contraindication; copper IUCD must not be inserted
B. WHO MEC 3 — risks outweigh advantages; prefer alternative method
C. WHO MEC 2 — advantages generally outweigh risks; IUCD can be provided
D. WHO MEC 1 — no restriction; insert freely
Reveal Answer
Answer: C. WHO MEC 2 — advantages generally outweigh risks; IUCD can be provided
Past PID, now resolved, in a woman in a mutually monogamous relationship with a tested negative partner is WHO MEC 2 for copper IUCD: the theoretical risk of recurrence exists, but advantages of a highly effective LARC generally outweigh it. Active PID or current STI would be WHO MEC 4 (absolute contraindication). Category 3 would apply to high-risk behaviour for STIs with current exposure concern. Always reassess before insertion.
Anatomy and Governing Principles
Safe IUCD placement depends on a clear mental model of the uterine axis and cavity dimensions. The non-pregnant uterus is typically anteverted (the corpus tilts anteriorly relative to the vagina) and anteflexed (the fundus tilts anteriorly relative to the cervix). In a retroverted uterus, instruments must be angled posteriorly during passage. The cervical canal runs from the external os to the internal os, normally 3–4 cm in length in a nulliparous woman and slightly wider after deliveries. The internal os is the narrowest point and the principal resistance to instrument passage; gentle traction on the cervix with a vulsellum straightens the cervico-uterine angle and reduces this resistance. The uterine cavity itself extends from the internal os to the fundus; sounding depth is normally 6–9 cm, and the device must be placed at the fundus to maximise efficacy and minimise expulsion.
The mechanism of action differs between the two main device types. The CuT 380A releases copper ions continuously; copper is toxic to spermatozoa (impairs motility and viability), interferes with fertilisation, and creates a local endometrial inflammatory response that is hostile to implantation. It is also an effective emergency contraceptive if inserted within 5 days of unprotected intercourse. The LNG-IUS releases approximately 20 µg of levonorgestrel per day (in the standard Mirena formulation), acting primarily by: (1) thickening cervical mucus to block sperm penetration, (2) causing endometrial atrophy, and (3) in some cycles, suppressing ovulation — though the primary mechanisms are local. Because LNG is released locally, systemic progestogenic effects are minimal, and the device is safe for use in breastfeeding women (WHO MEC 2 after 4 weeks postpartum, when milk supply is established).
Aseptic technique governs every step: IUCD insertion introduces a foreign body through a non-sterile vaginal and cervical canal into a normally sterile uterine cavity, and any breach in technique can seed organisms from the lower genital tract upward. The no-touch technique means that the part of the inserter that will enter the uterine cavity never contacts the vaginal walls, speculum, gloves once contaminated, or any unsterile surface. All instruments in contact with the uterus must be sterile or high-level disinfected. The speculum is cleaned but need not be sterile. The cervix is swabbed with antiseptic solution. Povidone-iodine (Betadine) is the most commonly used agent in Indian government facilities.
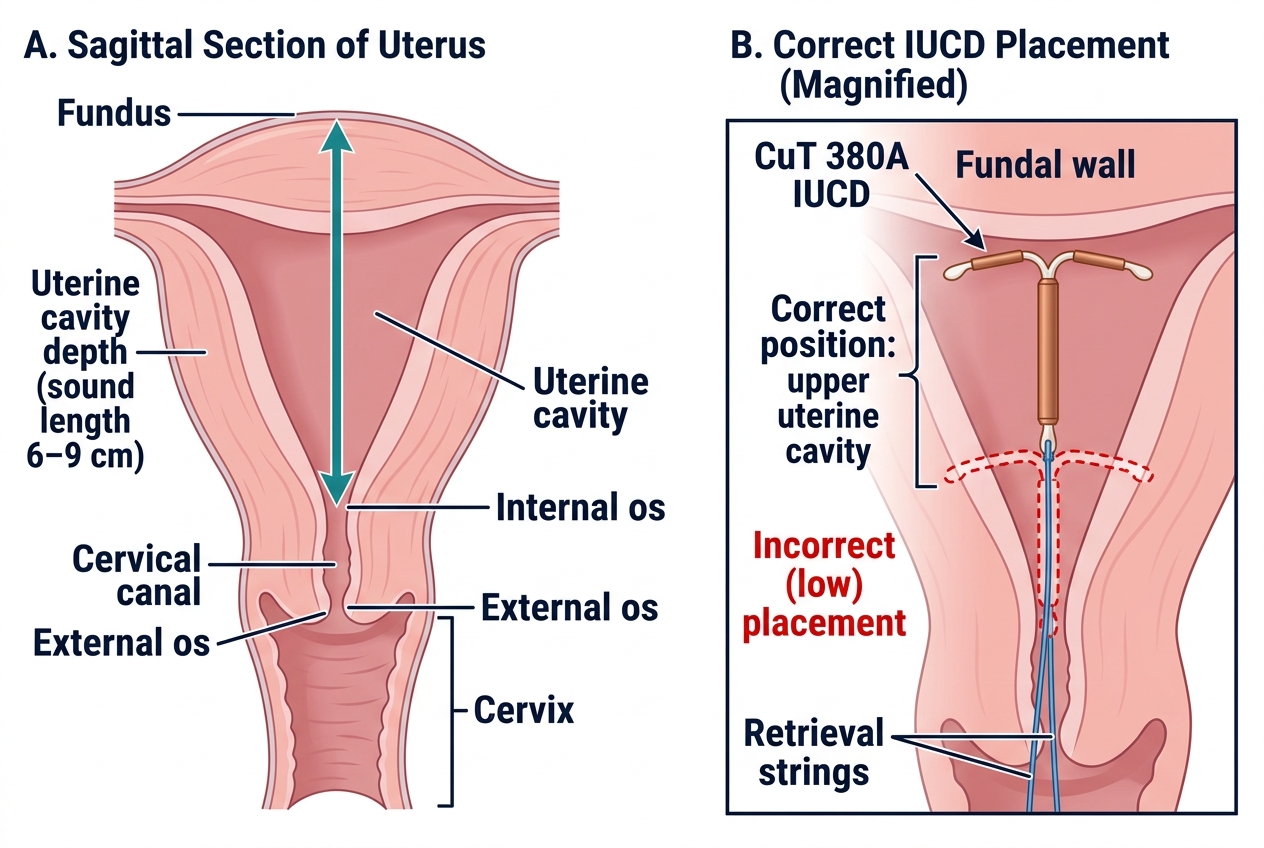
Sagittal anatomy of the uterus and correct IUCD placement
IUCD Insertion Technique
The following describes the standard technique for CuT 380A insertion in a non-pregnant, interval patient; the post-partum variant is noted at the end. Proficiency in this procedure is built through deliberate, supervised practice on a pelvic task-trainer model before any attempt at clinical insertion. Unlike many examination skills, IUCD insertion is irreversible once initiated — the device must be placed correctly on the first attempt, because repositioning after partial deployment can dislodge the arms and reduce efficacy. Every step must be rehearsed as a mental and physical sequence until it becomes automatic. The technique described below follows the standard no-touch plunger-withdrawal method recommended by the Ministry of Health and Family Welfare's PPIUCD Reference Manual and is aligned with the WHO guidance for copper IUCD insertion. Careful attention to asepsis, instrument handling, and patient communication during the procedure is as important as the mechanical steps.
Equipment required (sterile or high-level disinfected): bivalve vaginal speculum, long-handled sponge-holding forceps, cervical vulsellum (single-toothed or Allis), uterine sound, CuT 380A inserter kit (pre-loaded in sterile packaging), antiseptic solution (povidone-iodine), sterile gloves, good light source.
Step-by-step procedure:
1. Position and drape — patient in dorsal lithotomy position, bladder emptied, perineum cleaned with antiseptic.
2. Bimanual examination — assess uterine size, position (anteverted/retroverted), mobility, and tenderness. A tender uterus or adnexal tenderness should prompt deferral to exclude PID.
3. Speculum insertion — introduce the bivalve speculum, visualise the cervix under good light, clean the ectocervix and cervical os with povidone-iodine swabs.
4. Vulsellum application — apply a single-toothed vulsellum to the anterior lip of the cervix (12 o'clock). Gentle downward traction straightens the cervico-uterine angle.
5. Uterine sounding — insert the sterile sound gently through the cervical canal into the uterine cavity; advance to the fundus and note the depth in centimetres. A sound depth <6 cm suggests a small cavity (nulliparous, atrophic) that may not accommodate a standard device; >9 cm may indicate an enlarged or submucosal fibroid. Record the depth and uterine position.
6. Load and calibrate the inserter — adjust the moveable flange on the CuT 380A inserter tube to the measured sounding depth, so the flange will indicate when the device has reached the fundus.
7. Device loading — ensuring no-touch technique, load the T-arms into the inserter tube in the sterile package. The arms are folded into the tube no more than 5 minutes before insertion to prevent stress fracture of the copper sleeve.
8. Insertion — withdrawal technique (recommended for most settings): advance the loaded inserter tube through the cervical canal until the flange is at the level of the external os (indicating the device is at the fundal level). While holding the solid plunger rod steady, withdraw the outer tube 1–2 cm ('plunger-withdrawal' or 'no-push' technique) — this releases the T-arms within the uterine cavity. Then remove the inserter completely by withdrawing both tubes/rod together.
9. Thread trimming — cut the threads to leave approximately 2–3 cm protruding from the external os. Do not cut threads flush with the cervix (makes removal difficult) or leave them very long (patient discomfort; partner may feel them).
10. Remove vulsellum and speculum — examine for bleeding from the cervical puncture site; apply pressure if needed.
11. Post-insertion counselling — remind the patient how to check threads (monthly after each period), advise on when to return (missed period, lower abdominal pain, fever, thread absent/longer), and document insertion in the records including device type, batch number, and sounding depth.
PPIUCD (postpartum within 48 hours) variant: After a normal vaginal delivery, the uterus is large and soft. The device is inserted manually (by hand, reaching into the uterine cavity) or with ring/sponge-holding forceps immediately after placental expulsion or within 48 hours. The device is placed at the fundus with the arms in the coronal plane. Expulsion rates are higher than interval insertion (approximately 10–12% vs 2–5%) but the method remains effective overall and is preferred for its contraceptive immediacy. PPIUCD is NOT recommended at caesarean section unless specific training in the intra-caesarean technique has been received.
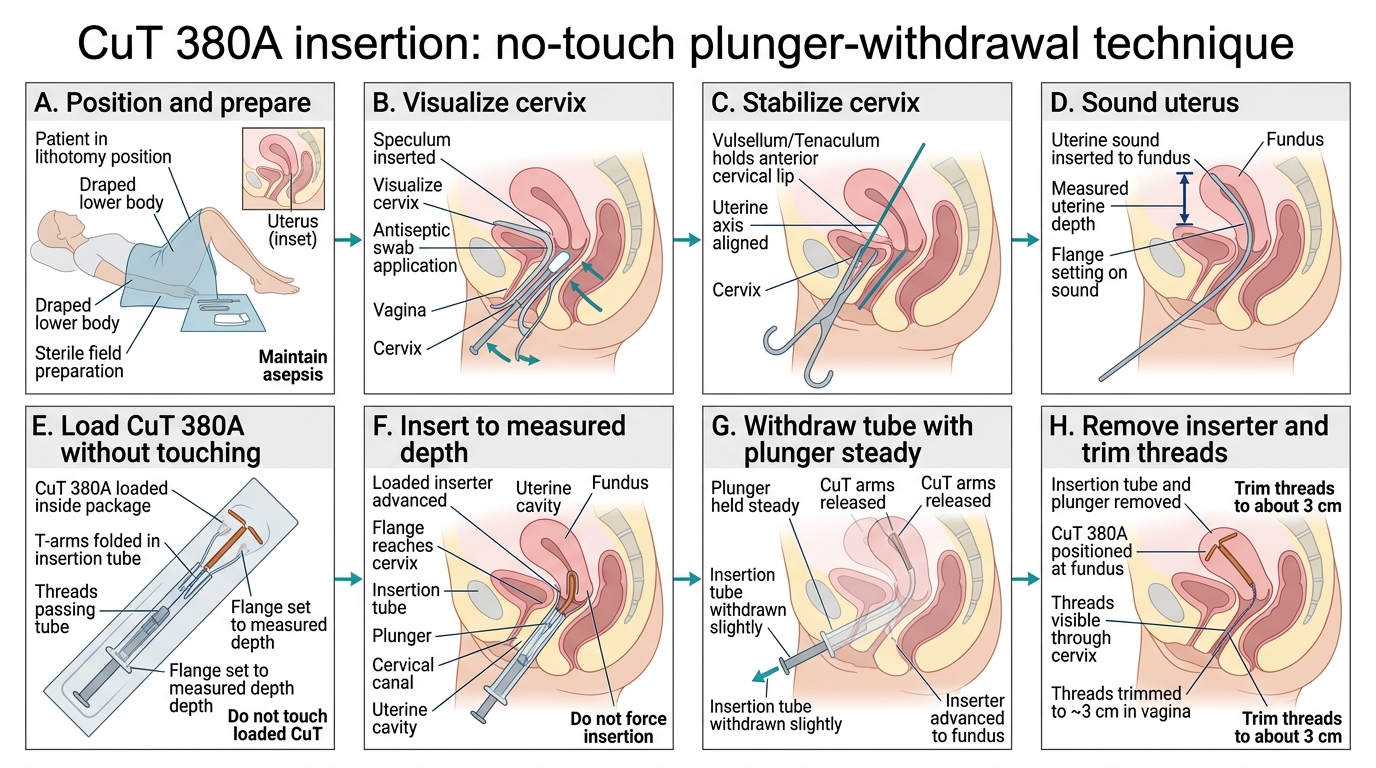
CuT 380A Insertion by No-Touch Plunger-Withdrawal Technique