Page 18 of 28
OG22.1 | Physiological Vaginal Discharge — SDL Guide
Learning Objectives
- Describe the four sources that contribute to normal vaginal discharge
- Describe the clinical characteristics (volume, colour, consistency, odour) of physiological vaginal discharge
- Explain the cyclical hormonal variation in vaginal discharge across the menstrual cycle
- Explain the role of Lactobacillus species and vaginal pH in maintaining a healthy vaginal environment
- Distinguish the clinical features of physiological discharge from early warning signs of pathological discharge
INSTRUCTIONS
Vaginal discharge is one of the most common gynaecological complaints encountered in clinical practice, yet the majority of women presenting with it have entirely normal, physiological secretions. A firm grasp of what constitutes normal discharge — its sources, hormonal variation, and protective microbiological context — is the prerequisite for confidently recognising and managing the pathological causes covered in the next SDL. This module focuses exclusively on physiological discharge; work through it carefully before proceeding to the discharge syndromes module.
References
- DC Dutta's Textbook of Gynecology, 8th ed., Ch. 24 (Leucorrhoea and Vaginal Discharge) (textbook)
- Jeffcoate's Principles of Gynaecology, 8th ed., Ch. 20 (textbook)
- Shaw's Textbook of Gynaecology, 17th ed., Ch. 18 (textbook)
- Ravel J et al. Vaginal microbiome of reproductive-age women. PNAS 2011;108(Suppl 1):4680–7 (journal)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 19-year-old unmarried woman presents to your outpatient clinic appearing visibly embarrassed. She reports a whitish vaginal discharge for the past four months. She has no sexual partner. She says the discharge is odourless, not itchy, and seems to increase 'in the middle of the month' and just before her period. She is deeply anxious, having read online that discharge 'always means an infection'. Examination reveals normal external genitalia, a healthy-looking cervix with clear mucoid secretion at the os, and no vaginal wall inflammation. Vaginal pH is 4.2. How would you counsel her, and what is the underlying physiology?
WHY THIS MATTERS
Understanding physiological vaginal discharge matters for three clinical reasons. First, it prevents unnecessary investigations and treatments: a significant proportion of women presenting with discharge to primary care or outpatient gynaecology have physiological secretions that require only reassurance and hygiene counselling, not antibiotics or antifungals. Prescribing unnecessarily disrupts the protective vaginal microbiome and creates drug resistance. Second, accurate knowledge of normal discharge characteristics is the baseline from which all pathological patterns are defined — if you do not know what is normal, you cannot reliably identify what is abnormal. Third, this knowledge underpins reproductive health counselling: changes in cervical mucus are used in natural family planning methods, and patients frequently ask about discharge-related concerns during antenatal visits, contraceptive consultations, and well-woman check-ups. The competency (OG22.1, KH level) reflects that this is foundational knowledge every graduating physician must command.
RECALL
Before beginning, recall: (1) The vaginal epithelium is stratified squamous, non-keratinised, oestrogen-sensitive — glycogen deposition in the cells is oestrogen-driven. (2) Cervical mucus is secreted by the columnar epithelium of the endocervical glands; its physical properties (viscosity, water content, ferning) vary with oestrogen and progesterone. (3) The normal menstrual cycle is approximately 28 days: follicular phase (days 1–14, oestrogen rising), ovulation (day ~14), luteal phase (days 14–28, progesterone dominant). (4) Bartholin glands are paired mucous glands at the posterior vestibule — they contribute a small volume of lubricating mucus. (5) The concept of normal flora: resident microbial communities that compete with pathogens and contribute to local immunity.
Orientation and Clinical Relevance
Vaginal discharge is a universal experience among women of reproductive age. The term refers to any fluid secreted from or passing through the vagina; distinguishing normal from abnormal requires understanding the biology of normal secretion before applying clinical pattern recognition to pathological variants. In everyday clinical encounters, the most common error is over-pathologising normal discharge — labelling physiological secretion as infection and initiating unnecessary treatment. This error has real consequences: inappropriate antibiotic use destroys the protective lactobacillus-dominant microbiome, creates antibiotic-resistant flora, may predispose to secondary fungal infection (post-antibiotic candidiasis), and causes patient distress through repeated treatment cycles for a problem that was never present.
Leucorrhoea (from the Greek leukos, white + rhoia, flow) is the clinical term for white or whitish vaginal discharge; in practice, 'leucorrhoea' is used to describe normal physiological discharge, though the term is sometimes applied broadly to any discharge. Physiological leucorrhoea is expected and normal. It increases at predictable physiological states: at puberty (rising oestrogen), in the mid-cycle peri-ovulatory period (oestrogen surge), during pregnancy (increased vascularity and glandular activity), and in the premenstrual week. Each of these variations is driven by the hormonal milieu and reflects healthy reproductive tract function, not disease.
The clinical relevance of this SDL is direct: in the gynaecological consultation, the first question after a patient reports discharge is 'does this look and feel normal, or are there features suggesting infection or inflammation?' That question is only answerable if you have a precise mental model of what normal looks, smells, and feels like — and what its normal variation patterns are.
Sources and Composition of Normal Vaginal Discharge
Normal vaginal discharge is not secreted by a single gland or tissue — it is a composite fluid arising from four distinct anatomical sources, each contributing different components. Understanding this composite origin helps explain why the discharge changes with hormonal state, infection, and reproductive events.
The four sources of physiological vaginal discharge are: (1) Endocervical glands — columnar epithelial cells lining the cervical canal secrete mucus that forms the bulk of visible discharge; this mucus varies enormously in volume and consistency across the menstrual cycle under oestrogen and progesterone influence. (2) Vaginal wall transudation — the vaginal epithelium is not a secretory tissue in the traditional sense, but plasma transudes across the mucosal capillaries in response to oestrogen stimulation, contributing a serous fluid component to the discharge. (3) Desquamated vaginal epithelial cells — the oestrogen-stimulated squamous epithelium undergoes rapid turnover; shed cells, rich in glycogen, constitute a significant solid fraction and give discharge its whitish or creamy colour when accumulated. (4) Bartholin and Skene gland secretions — paired mucous glands at the posterior vaginal introitus and periurethral area contribute a small volume of lubricating mucus, particularly during sexual arousal, but also as a baseline trickle.
The resulting composite fluid in a healthy reproductive-age woman is: whitish or clear, non-offensive (mildly acidic smell acceptable; any fishy or yeasty odour is abnormal), variable in volume (approximately 1–4 mL per 24 hours by weight, though this is rarely measured clinically), and variable in consistency — watery to mucoid depending on cycle phase. There is no blood, no curd-like consistency (that suggests candidiasis), and no frothy yellow-green character (that suggests trichomoniasis). The absence of odour, pruritus, and vulval soreness are the key negative features that define physiological discharge at the bedside.
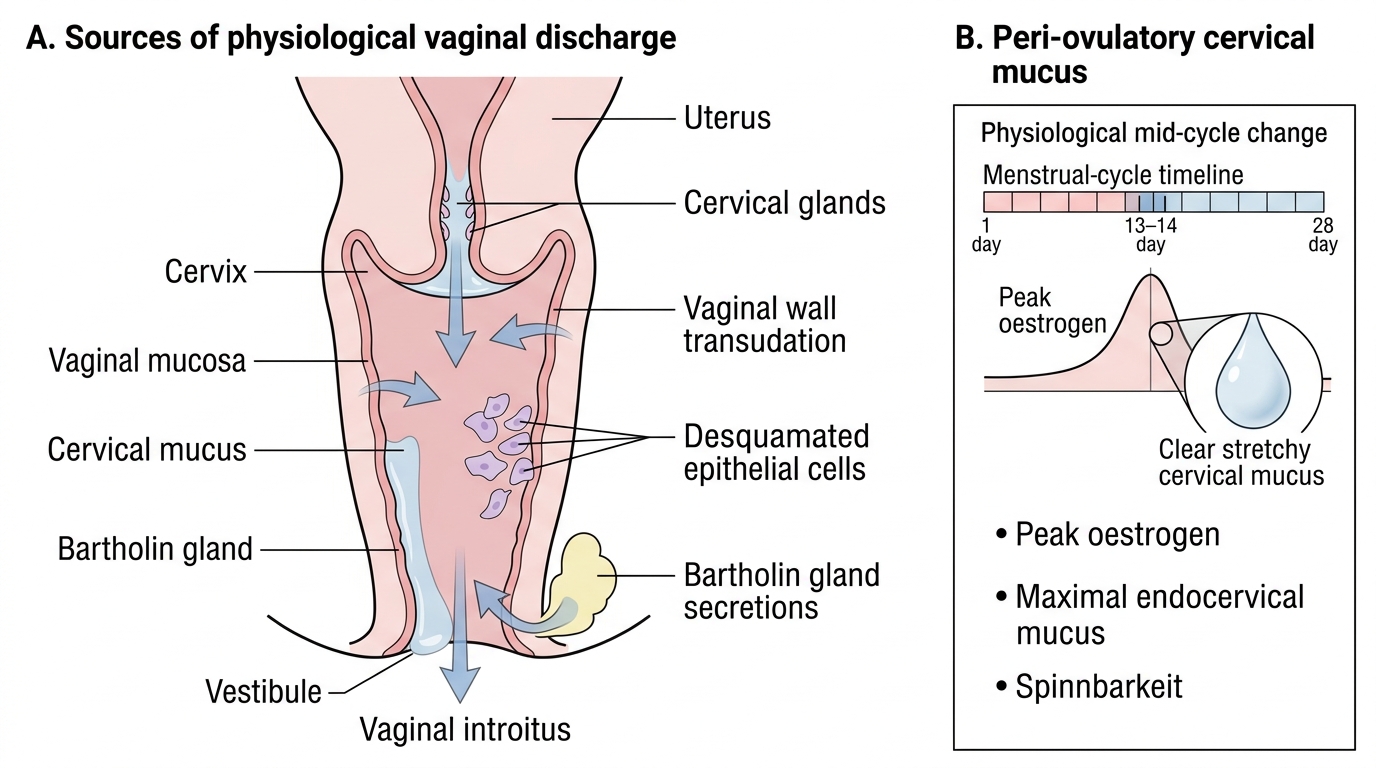
Sources of Physiological Vaginal Discharge
SELF-CHECK
A 22-year-old woman reports that her vaginal discharge is noticeably more copious and clear/stretchy for about 2 days every month, around day 13–14 of her 28-day cycle. She has no other symptoms. What is the most likely explanation for this cyclical increase?
A. Bacterial overgrowth occurring cyclically at mid-cycle
B. Peak oestrogen at the peri-ovulatory phase causing maximal endocervical mucus production
C. Progesterone dominance in the luteal phase making mucus more viscous and visible
D. Shedding of the endometrium beginning at ovulation
Reveal Answer
Answer: B. Peak oestrogen at the peri-ovulatory phase causing maximal endocervical mucus production
The peri-ovulatory rise in oestrogen (LH/FSH surge day ~14) causes maximum endocervical mucus production: high volume, clear, highly hydrated, with characteristic 'spinnbarkeit' (ability to be stretched in a thread) and ferning pattern on microscopy. This is the most fertile-quality mucus and is entirely physiological. Progesterone (luteal phase) does the opposite — it makes mucus thick, scanty, and hostile to sperm. Endometrial shedding does not occur at ovulation.
Cyclical Variation and Hormonal Determinants
The volume and physical properties of vaginal discharge change predictably across the menstrual cycle, driven by the reciprocal actions of oestrogen and progesterone on the endocervical epithelium and vaginal mucosa. Appreciating this cyclical pattern is essential for counselling women who present with concerns about mid-cycle or premenstrual discharge, and for understanding the physiological basis of natural family planning methods.
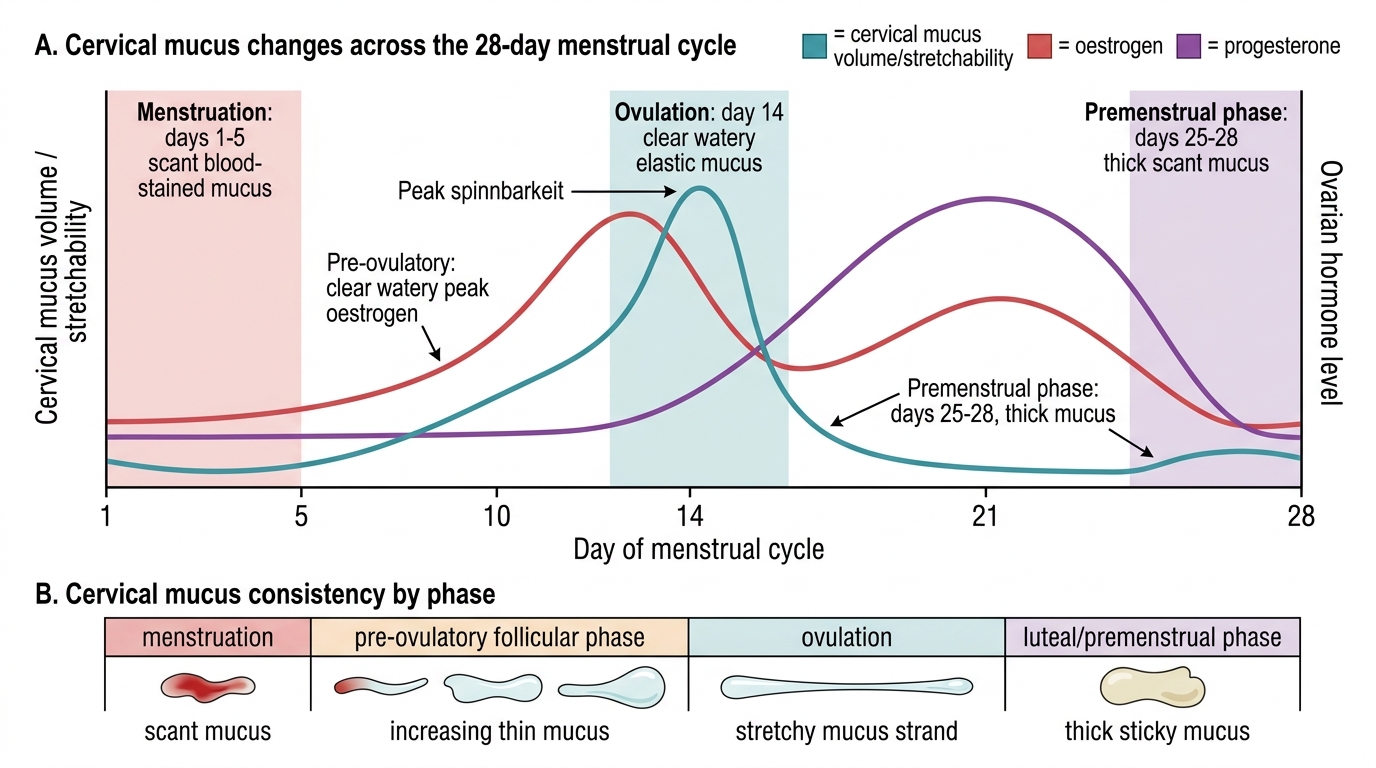
Follicular phase (days 1–14, oestrogen rising): As oestrogen rises from the low levels of menstruation toward its mid-cycle peak, the endocervical glands progressively increase mucus production. The discharge gradually increases in volume and becomes more watery and transparent. At the same time, oestrogen stimulates glycogen deposition in vaginal squamous cells, promoting epithelial thickness and increasing the substrate available to lactobacilli. By the late follicular phase, discharge is noticeably more copious.
Peri-ovulatory phase (approximately day 13–15): The pre-ovulatory oestrogen surge drives maximum endocervical mucus secretion. The mucus at this point is characteristically: high volume (up to 700 mg/day), crystal-clear, highly hydrated, thin, and exhibits spinnbarkeit — the ability to be stretched into a thread of 8–10 cm or more without breaking. This is the 'egg-white cervical mucus' that women using fertility awareness methods are taught to identify as the peak fertile window. On microscopic examination of dried mucus from this phase, a ferning pattern (arborisation) is seen, caused by sodium chloride crystallisation in the low-protein mucus — this is the basis of the ferning test used historically to assess oestrogen status.
Luteal phase (days 15–28, progesterone dominant): Following ovulation, progesterone from the corpus luteum rapidly changes cervical mucus properties. The mucus becomes thick, scant, viscous, and opaque — forming a cervical mucus plug that physically occludes the internal os and is hostile to sperm penetration. Visible discharge from the vagina decreases in the early-to-mid luteal phase. In the late luteal phase (premenstrual), as progesterone falls, discharge may increase again slightly and become more yellowish in colour — this is physiological and related to increased desquamation and some neutrophil influx in the late cycle endometrium.
Special physiological states: In pregnancy, oestrogen stimulation causes dramatically increased cervical mucus and vaginal transudation; pregnant women commonly notice copious, white/yellowish, non-offensive discharge from the first trimester onward. This is physiological leucorrhoea of pregnancy and requires no treatment. In postmenarchal adolescents, a similar oestrogen-driven leucorrhoea is often the first vaginal secretion noticed and commonly causes anxiety — reassurance and hygiene advice are the appropriate response. With combined oral contraceptives, synthetic progestogens suppress endogenous oestrogen and reduce mucus volume; many women notice reduced discharge on the pill.
Cyclical Cervical Mucus and Hormonal Changes