Page 11 of 22
OG24.1 | Abnormal Uterine Bleeding — SDL Guide
Learning Objectives
- Define abnormal uterine bleeding (AUB) using FIGO terminology and state the normal menstrual parameters
- Apply the FIGO PALM-COEIN classification system to categorise the causes of AUB
- Describe the clinical features and investigation pathway for a woman presenting with AUB
- Outline the medical and surgical management options for AUB, including cause-specific approaches
- Identify when endometrial biopsy is mandatory and which patients require urgent investigation for malignancy
INSTRUCTIONS
Abnormal uterine bleeding is the most common gynaecological complaint, accounting for up to one-third of outpatient consultations. It spans a spectrum from benign anovulatory cycles in adolescents to endometrial carcinoma in postmenopausal women. The 2011 FIGO PALM-COEIN classification system replaced the legacy terminology (DUB, menorrhagia, metropathia haemorrhagica) and provides a structured, internationally standardised framework for understanding causes. Mastering this system is essential — it transforms a potentially bewildering clinical presentation into a logical diagnostic and management algorithm.
References
- DC Dutta's Textbook of Gynecology, 8th ed., Ch. 25 — Abnormal Uterine Bleeding (textbook)
- Shaw's Textbook of Gynaecology, 17th ed., Ch. 21 — Abnormal Uterine Bleeding (textbook)
- Munro MG et al. FIGO Classification System (PALM-COEIN) for causes of AUB in nongravid women of reproductive age. Int J Gynaecol Obstet. 2011;113(1):3-13 (guideline)
- NICE Clinical Guideline NG88: Heavy menstrual bleeding: assessment and management. 2018 (updated 2023) (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 38-year-old woman presents with heavy periods for the past 8 months — she is soaking through a pad every hour on the first two days of her cycle and has passed clots. She is pale and her haemoglobin is 9.2 g/dL. Pelvic ultrasound shows a 4 cm intramural fibroid and a 1.5 cm endometrial polyp. She has one child and does not want further pregnancies. What is the FIGO classification of her bleeding? What medical and surgical options are available, and in what order would you offer them?
WHY THIS MATTERS
Abnormal uterine bleeding affects approximately 1 in 5 women at some point in their reproductive life. It is the leading indication for hysterectomy worldwide and accounts for enormous direct healthcare costs and indirect productivity losses from anaemia and work absence. For the clinician, AUB matters because: (1) it is common — you will see it daily in outpatient practice; (2) the differential spans the entirely benign (anovulatory cycles, fibroids) to the life-threatening (endometrial carcinoma); (3) the investigation and management approach must be structured and evidence-based to avoid both over-treatment of benign conditions and missed malignancy; (4) the PALM-COEIN classification is now the international standard and will be expected in written examinations and clinical practice.
RECALL
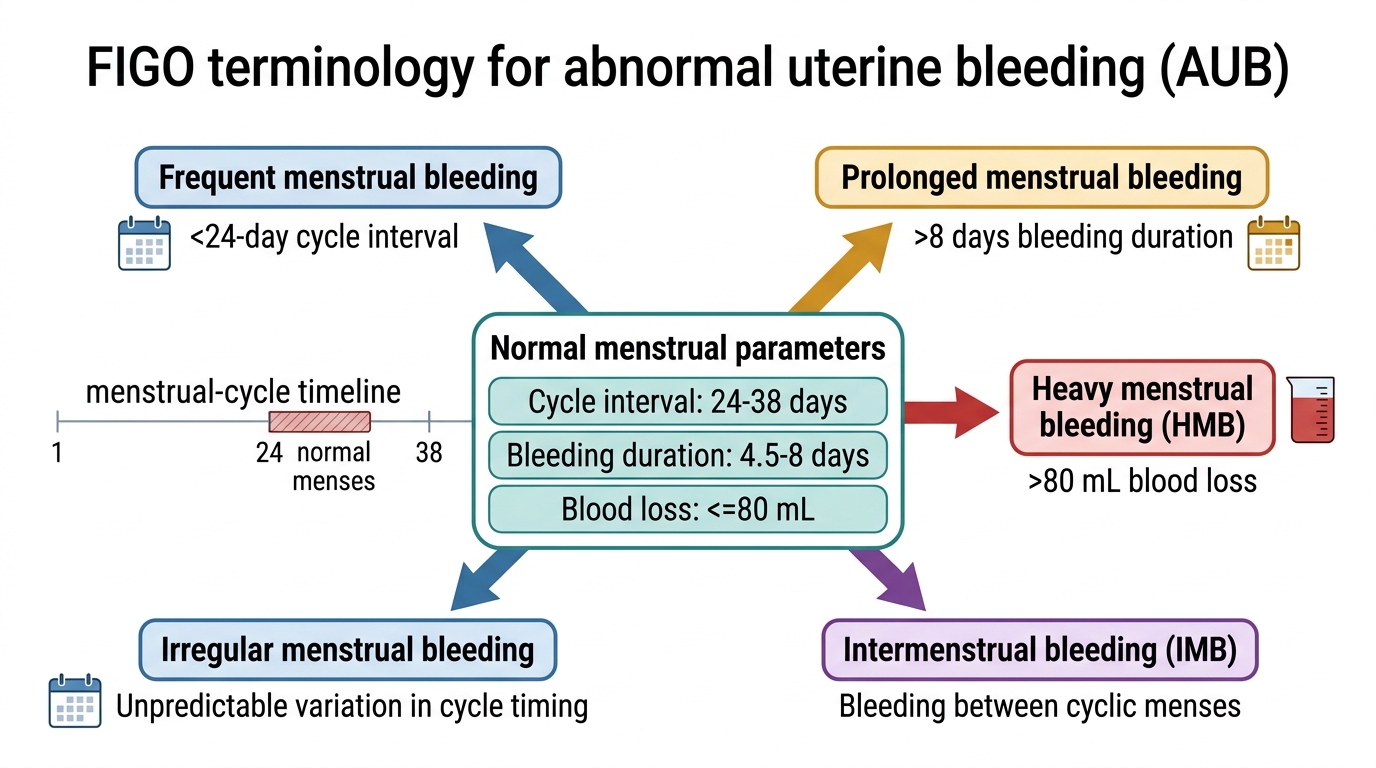
Recall the normal menstrual cycle: frequency 24–38 days; duration 4.5–8 days; blood loss ≤80 mL per cycle. The cycle is driven by the HPO axis — FSH-stimulated follicular development → oestradiol rise → LH surge → ovulation → corpus luteum → progesterone → if no pregnancy, luteal regression → oestrogen/progesterone withdrawal → menstruation. Ovulation is the key event: anovulatory cycles (from PCOS, hypothyroidism, puberty, perimenopause) produce irregular, often heavy bleeding from unopposed oestrogen without progesterone-mediated stabilisation of the endometrium.
Clinical Presentation and Definition of AUB
Abnormal uterine bleeding (AUB) is an umbrella term for any bleeding from the uterus that falls outside the normal parameters for frequency, regularity, duration, or volume, or that occurs at an abnormal time (between periods, after sex, after menopause). The FIGO system uses precise terminology to describe the bleeding pattern, because the pattern itself carries diagnostic weight: heavy regular bleeding suggests a structural cause (fibroid, polyp); irregular or unpredictable bleeding suggests ovulatory dysfunction or endometrial pathology; postcoital bleeding raises the possibility of a cervical lesion.
The FIGO-standardised terminology for AUB patterns is as follows. Normal menstrual parameters are: cycle frequency 24–38 days; cycle regularity ±7–9 days variation; menstrual duration 4.5–8 days; menstrual volume ≤80 mL per cycle. Deviations from these are named precisely: Heavy menstrual bleeding (HMB) replaces the deprecated term 'menorrhagia' — defined as blood loss >80 mL per cycle or, pragmatically, as excessive blood loss that interferes with a woman's physical, social, emotional, or quality of life. Intermenstrual bleeding (IMB) is bleeding between otherwise regular periods — this is a separate entity from HMB. Irregular menstrual bleeding refers to variation in cycle length of more than ±9 days (formerly 'oligomenorrhoea' for infrequent). Postcoital bleeding (PCB) — bleeding triggered by sexual intercourse — suggests a cervical or vaginal source and must always prompt cervical examination and colposcopy. Postmenopausal bleeding (PMB) — any uterine bleeding occurring 12 months or more after the last menstrual period — is endometrial carcinoma until proven otherwise and demands urgent investigation.
The patient's age critically shapes the differential. In adolescence, anovulatory cycles are the dominant cause (immaturity of the HPO axis), with coagulopathy (von Willebrand disease) accounting for up to 20% of heavy bleeding in adolescents. In reproductive age, the PALM structural causes (fibroids, polyps, adenomyosis) and COEIN non-structural causes (anovulation from PCOS, thyroid disease, iatrogenic) are both common. In the perimenopausal and postmenopausal period, endometrial hyperplasia and carcinoma must be excluded first — AUB after menopause is a red flag regardless of the bleeding volume.
FIGO Terminology Framework for AUB
SELF-CHECK
A 45-year-old woman reports that her periods have become irregular over the past year, sometimes every 3 weeks and sometimes every 6 weeks, with occasional spotting between cycles. Using FIGO terminology, how is this bleeding best described?
A. Heavy menstrual bleeding (HMB)
B. Irregular menstrual bleeding with intermenstrual bleeding (IMB)
C. Postmenopausal bleeding (PMB)
D. Dysmenorrhoea
Reveal Answer
Answer: B. Irregular menstrual bleeding with intermenstrual bleeding (IMB)
The cycle variation of more than ±9 days constitutes irregular menstrual bleeding. The spotting between cycles is intermenstrual bleeding (IMB). HMB refers specifically to excessive volume, which is not described here. PMB requires at least 12 months of amenorrhoea since the last period — this woman is still having periods. Dysmenorrhoea refers to painful menstruation, not to an abnormal bleeding pattern.
The FIGO PALM-COEIN Classification of AUB
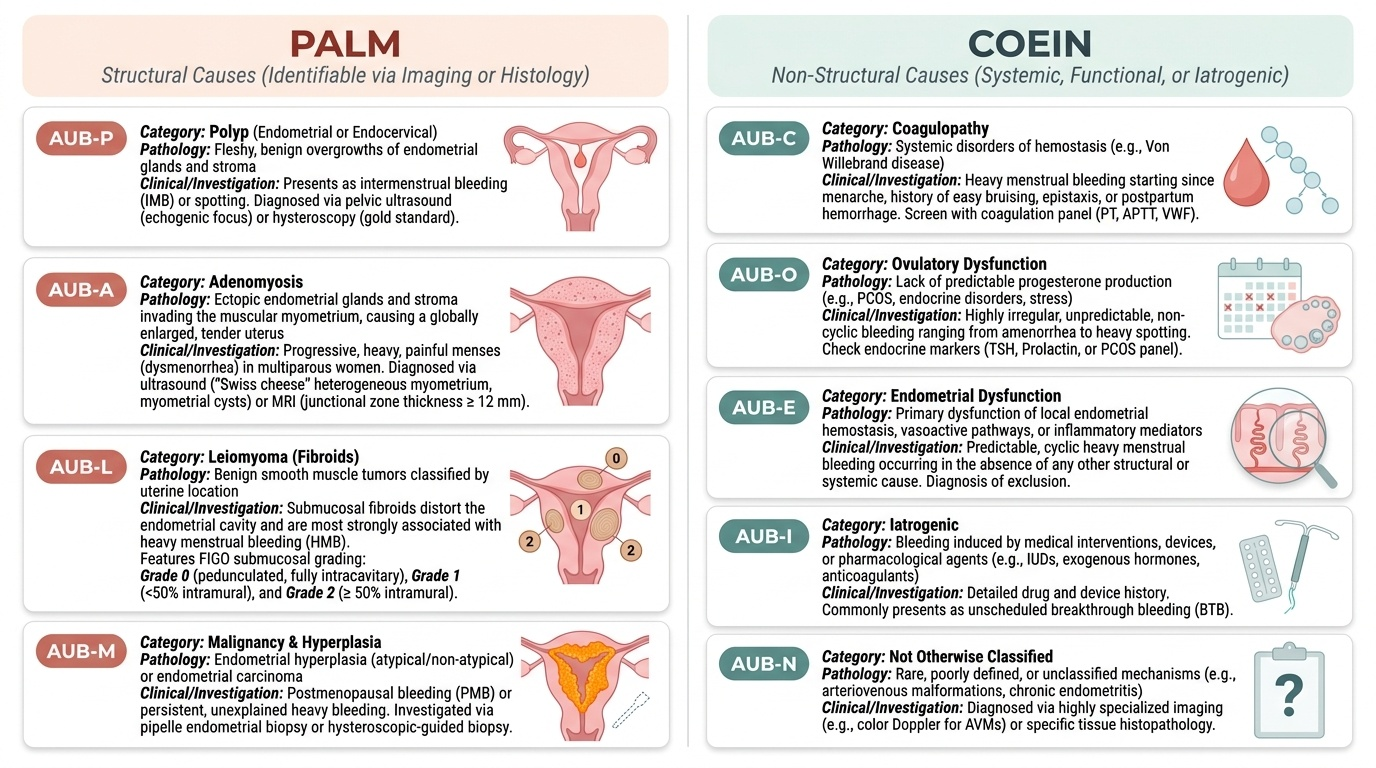
The FIGO PALM-COEIN classification (Munro et al., 2011; updated 2018) replaced the legacy terminology of 'dysfunctional uterine bleeding (DUB),' 'menorrhagia,' and 'metropathia haemorrhagica' with a structured, internationally standardised system. The acronym encapsulates the full range of causes: PALM covers structural causes identifiable by imaging or histology; COEIN covers non-structural causes. A patient may have more than one concurrent cause — for example, a woman with PCOS may have both AUB-O (anovulatory) and AUB-L (coincidental fibroid) — and the classification system accommodates this by allowing multiple concurrent labels. Understanding each category at the level of its mechanism, clinical signature, and investigation is what transforms this acronym from a memorisation exercise into a clinical decision-making tool.
PALM — Structural Causes:
AUB-P (Polyp): Endometrial or endocervical polyps are fleshy, benign overgrowths of endometrial glands and stroma. They typically cause IMB or spotting, though large polyps can cause HMB. Diagnosis by pelvic ultrasound (echogenic focus within the endometrial cavity, best seen in the early follicular phase when the endometrium is thin) or hysteroscopy (gold standard for visualisation and targeted biopsy). Management: hysteroscopic polypectomy. Risk of malignancy within a polyp is low (<1–2%) but increases with age and postmenopausal status.
AUB-A (Adenomyosis): Ectopic endometrial glands and stroma within the myometrium, causing the uterus to become enlarged, globular, and tender. Classic presentation: progressively worsening heavy, painful menstruation in a multiparous woman in her 40s. Diagnosis: pelvic ultrasound (enlarged uterus, heterogeneous myometrium, myometrial cysts — 'Swiss cheese' pattern) or MRI (more sensitive; junctional zone thickening >12 mm). Definitive diagnosis: histology after hysterectomy. The uterus is often symmetrically enlarged and tender on palpation. Management: LNG-IUS (first-line medical); hysterectomy is curative.
AUB-L (Leiomyoma/Fibroid): Benign smooth muscle tumours of the uterus. The FIGO sub-classification by location is essential because only certain fibroid locations cause bleeding — submucosal fibroids (those distorting the endometrial cavity) are most strongly associated with AUB, whereas intramural and subserosal fibroids may not cause bleeding at all. The FIGO leiomyoma sub-classification: Type 0 = pedunculated intracavitary (entirely within the cavity); Type 1 = submucosal, <50% intramural; Type 2 = submucosal, ≥50% intramural; Types 3–8 = intramural and subserosal variants. Submucosal fibroids (types 0–2) cause HMB by impairing endometrial haemostasis. Diagnosis: pelvic ultrasound; saline infusion sonography (SIS) or hysteroscopy for intracavitary fibroids.
AUB-M (Malignancy and Hyperplasia): Endometrial hyperplasia (with or without atypia) and endometrial carcinoma. Endometrial hyperplasia results from prolonged unopposed oestrogen stimulation — risk factors include obesity, PCOS, anovulatory cycles, tamoxifen, HRT (oestrogen-only). Atypical hyperplasia carries 8–29% concurrent carcinoma risk and is a premalignant lesion requiring hysterectomy in women who have completed their family. Endometrial carcinoma: most common gynaecological cancer in developed countries; presents as PMB (must be excluded first) or irregular/heavy bleeding in older reproductive-age women. Investigation: transvaginal ultrasound (endometrial thickness ≥4 mm postmenopause = threshold for biopsy), hysteroscopy, endometrial biopsy (Pipelle).
COEIN — Non-Structural Causes:
AUB-C (Coagulopathy): Systemic bleeding disorders. Von Willebrand disease (vWD) is the most common, affecting ~1% of women with HMB. Presents as HMB from menarche, often with a positive bleeding history (bruising, epistaxis, prolonged bleeding after dental/surgical procedures). Screening: platelet count, PT/APTT, von Willebrand factor antigen and activity (ristocetin cofactor assay). Also consider: thrombocytopenia (ITP, medication-induced), platelet function disorders. Anticoagulant therapy (heparin, warfarin, DOACs) is an iatrogenic cause (AUB-I, see below) — not classified under AUB-C.
AUB-O (Ovulatory Dysfunction): Anovulatory or oligo-ovulatory cycles producing irregular, often heavy, and unpredictable bleeding from unopposed oestrogen acting on the endometrium without progesterone-mediated stabilisation. The endometrium becomes thick and unstable, then sheds irregularly. The most common non-structural cause of AUB. Causes: PCOS (most common cause of AUB-O in reproductive-age women), hypothyroidism (TSH elevated — must always be excluded), hyperprolactinaemia, extremes of reproductive life (puberty, perimenopause), hypothalamic suppression (weight loss, athletics), and less commonly, adrenal disease. Investigation: TSH, prolactin, day-21 progesterone (low or absent confirming anovulation), LH:FSH ratio and testosterone in PCOS.
AUB-E (Endometrial): Disorders of local endometrial haemostatic mechanisms, prostaglandin metabolism, and vasoactive factors — in the absence of any other identifiable structural or systemic cause. The endometrium fails to regulate menstrual blood loss normally despite normal ovulatory function and no identifiable structural pathology. This is a diagnosis of exclusion after other causes have been excluded. Includes endometritis (chronic infection — Chlamydia, actinomyces from IUCD). Management: tranexamic acid and NSAIDs are highly effective (target the prostaglandin and fibrinolytic pathways).
AUB-I (Iatrogenic): Bleeding related to exogenous interventions — including anticoagulant medications (warfarin, heparin, DOACs), oestrogen-containing medications (breakthrough bleeding on OCP), gonadal steroids, intrauterine devices (copper IUD causes heavier periods; LNG-IUS causes lighter periods), and chemotherapy.
AUB-N (Not yet classified): Rare or incompletely characterised causes not fitting the above — e.g., arteriovenous malformations, caesarean scar defect (isthmocele), myometrial hypertrophy.
Provided image
SELF-CHECK
A 28-year-old woman with irregular, unpredictable heavy periods since menarche is found to have anovulatory cycles. TSH is normal. She has features of PCOS on ultrasound. According to the FIGO PALM-COEIN classification, her AUB is best categorised as:
A. AUB-L (Leiomyoma)
B. AUB-O (Ovulatory dysfunction)
C. AUB-E (Endometrial)
D. AUB-P (Polyp)
Reveal Answer
Answer: B. AUB-O (Ovulatory dysfunction)
Anovulatory cycles in PCOS cause irregular, heavy bleeding from unopposed oestrogen — this is the classic AUB-O (Ovulatory dysfunction) pattern. The absence of a structural lesion on ultrasound excludes AUB-L and AUB-P. AUB-E is a diagnosis of exclusion after ovulatory dysfunction has been confirmed absent — it applies to women with normal ovulatory function and no structural cause. AUB-O is the most common non-structural cause of AUB in reproductive-age women.
Diagnosis and Investigation of AUB
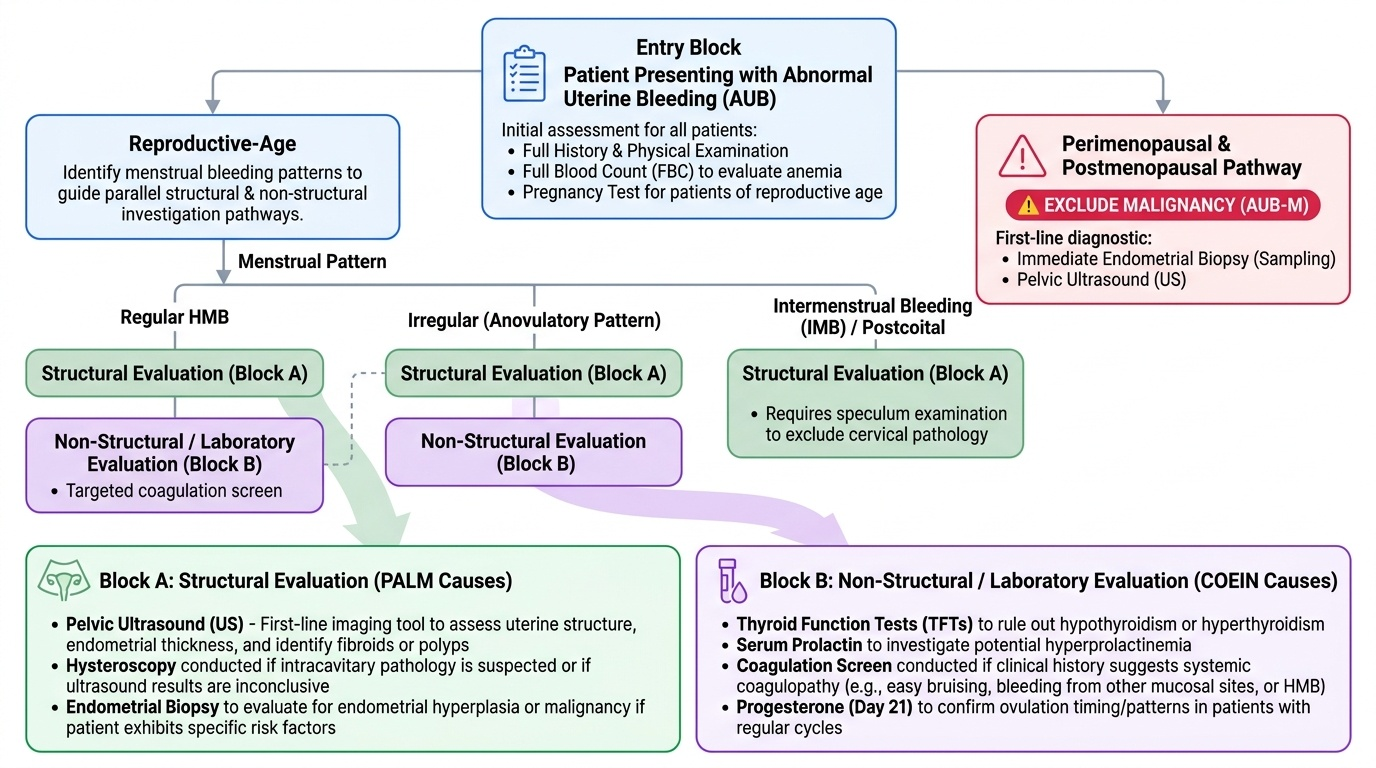
The investigation of AUB follows a structured pathway shaped by the patient's age, bleeding pattern, and the clinical suspicion raised by history and examination. The investigative priority differs by age group: in the perimenopausal and postmenopausal woman, excluding malignancy (AUB-M) takes precedence over all other considerations, and endometrial sampling must not be delayed. In the reproductive-age woman, structural causes (PALM) and systemic causes (COEIN) are pursued in parallel, guided by the clinical pattern.
A careful history is the foundation of the investigation. The menstrual history should establish: exact dates of the last two periods, cycle regularity, duration and volume of flow (pad/tampon count, presence of clots, flooding), and whether the bleeding is intermenstrual or postcoital. Associated features: dysmenorrhoea (adenomyosis), pressure symptoms such as urinary frequency or bowel changes (large fibroids), galactorrhoea (hyperprolactinaemia), weight change and cold intolerance (hypothyroidism), easy bruising and bleeding from other sites (coagulopathy). Obstetric history: parity, previous caesarean sections (scar defect as AUB-N cause). Medications: anticoagulants, hormonal preparations, tamoxifen.
Physical examination: abdominal palpation for uterine enlargement; speculum examination (cervical polyp, cervicitis, friable cervix for postcoital bleeding — urgent colposcopy referral); bimanual pelvic examination (uterine size, tenderness, mobility; adnexal masses).
Investigation pathway by age and pattern:
All women with AUB:
- Full blood count (FBC): assess for anaemia (Hb, MCV, ferritin); thrombocytopenia.
- Pregnancy test: exclude intrauterine or ectopic pregnancy in women of reproductive age — this is mandatory before any further investigation and must never be overlooked.
- Cervical smear if due (cervical pathology as cause of PCB).
Reproductive-age women (structural work-up):
- Transvaginal pelvic ultrasound (TVUS): first-line imaging; assess endometrial thickness, cavity for polyps/fibroids, ovaries for PCOS. Saline infusion sonography (SIS) or 3D ultrasound adds accuracy for intracavitary lesions.
- Hysteroscopy: gold standard for endometrial cavity visualisation — detects polyps, submucosal fibroids, and endometrial pathology with direct visual inspection and targeted biopsy. Preferred over blind endometrial sampling for intracavitary pathology.
- Endometrial biopsy (Pipelle): mandatory in women ≥45 years with AUB, or in women <45 years with risk factors for endometrial carcinoma (obesity, PCOS, prolonged anovulation, tamoxifen).
Non-structural work-up (COEIN):
- TSH (exclude hypothyroidism — must be done in every woman with irregular/heavy AUB).
- Prolactin (hyperprolactinaemia causes anovulation → AUB-O).
- Day-21 serum progesterone (mid-luteal): <3 nmol/L confirms anovulation; ≥16 nmol/L confirms ovulation.
- Coagulation screen (PT, APTT) + von Willebrand factor antigen and activity if HMB since menarche or positive bleeding history (ISTH-BAT score ≥3 in reproductive-age women).
- LH:FSH ratio, testosterone, fasting insulin (PCOS screen if irregular cycles).
Perimenopausal and postmenopausal women:
- Transvaginal ultrasound: endometrial thickness <4 mm postmenopause has a negative predictive value >99% for carcinoma. Thickness ≥4 mm → mandatory endometrial biopsy.
- Hysteroscopy and directed biopsy: preferred for definitive histological diagnosis; endometrial thickness alone does not exclude focal lesions.
- MRI pelvis: for staging if malignancy confirmed on biopsy.
Provided image
SELF-CHECK
A 52-year-old woman presents with vaginal bleeding 18 months after her last period. Transvaginal ultrasound shows an endometrial thickness of 6 mm. The most appropriate next step is:
A. Reassure — 6 mm is within normal limits for postmenopause
B. Repeat ultrasound in 6 months
C. Endometrial biopsy (Pipelle) and/or hysteroscopy — endometrial thickness ≥4 mm postmenopause mandates histological sampling
D. Start progestogen therapy empirically to reduce the endometrial thickness
Reveal Answer
Answer: C. Endometrial biopsy (Pipelle) and/or hysteroscopy — endometrial thickness ≥4 mm postmenopause mandates histological sampling
Postmenopausal bleeding with endometrial thickness ≥4 mm on TVUS mandates endometrial histological sampling to exclude endometrial carcinoma — the threshold is 4 mm, not 5 mm or higher. An endometrial thickness of 6 mm exceeds this threshold. Pipelle biopsy is the first-line outpatient method; hysteroscopy with directed biopsy is the gold standard if biopsy is inconclusive or if there is a focal lesion. Empirical progestogen without histological diagnosis is inappropriate.