Page 9 of 22
OG23.3 | Precocious Puberty — SDL Guide (Part 2)
Management of Precocious Puberty
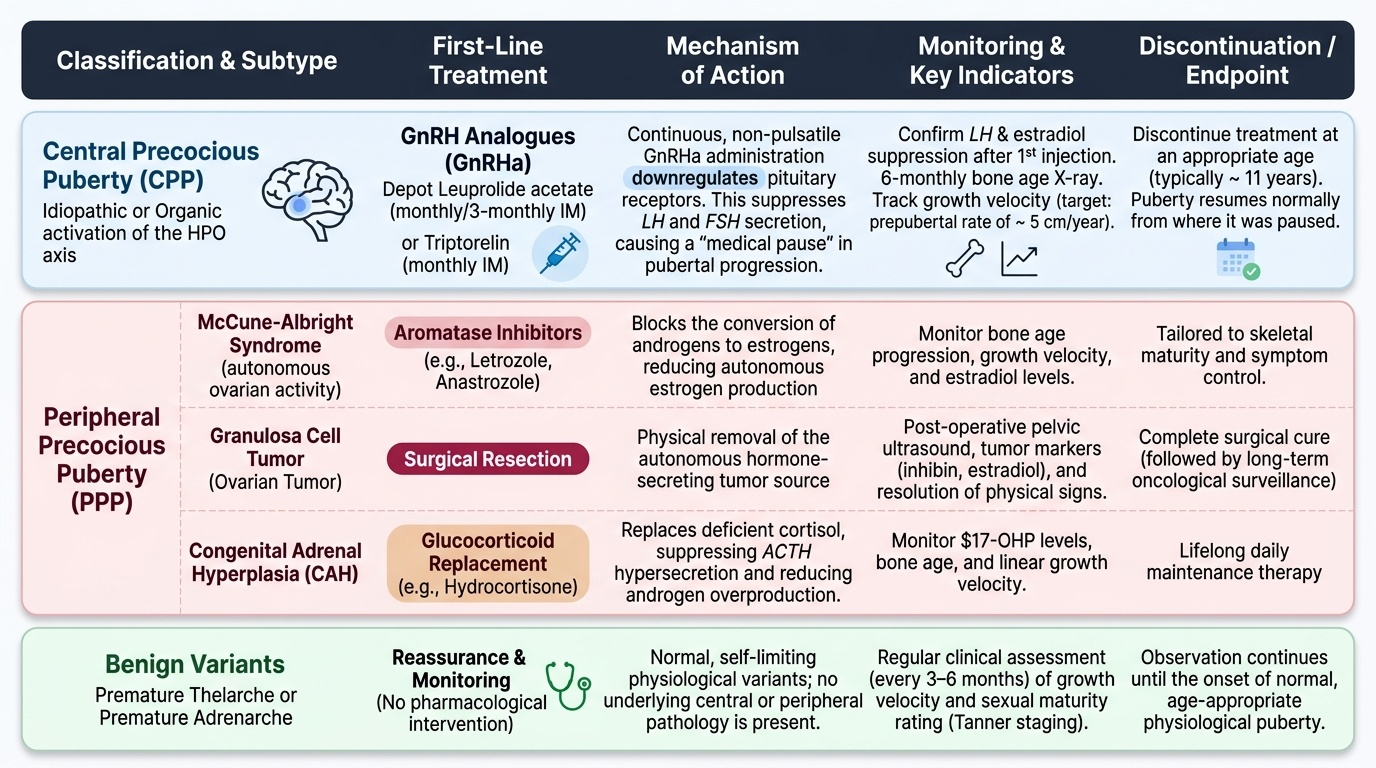
The management of precocious puberty is dictated entirely by the classification. Central precocious puberty has a well-established, effective treatment in the form of GnRH analogues, which suppress the prematurely activated HPO axis and allow the child to reach her genetically programmed adult height. Peripheral precocious puberty requires treatment of the underlying autonomous hormone source — this varies by cause, from surgical removal of an ovarian tumour to steroid replacement for CAH to targeted medical therapy for McCune-Albright syndrome. Benign variants (premature thelarche, premature adrenarche) require monitoring and reassurance, not active treatment.
Central Precocious Puberty — GnRH Analogue Therapy:
The principle of treatment exploits the fact that GnRH receptors in the pituitary are only activated by pulsatile GnRH. Continuous, non-pulsatile GnRH (provided by a long-acting depot analogue) downregulates GnRH receptors, suppressing LH and FSH secretion and reversing pubertal progression. The result is a 'medical pause' in puberty — breast tissue does not regress significantly but further progression is halted, growth velocity normalises to prepubertal rates, and bone age advancement is arrested. When treatment is stopped (usually at an appropriate age — typically around 11 yr), puberty resumes from where it was paused.
GnRH analogues used: leuprolide acetate (monthly or 3-monthly depot IM injection), triptorelin (monthly depot IM), or histrelin (annual subcutaneous implant). Monitoring during treatment: LH and oestradiol suppression confirmed after the first injection; 6-monthly bone age X-ray; growth velocity (should decrease to prepubertal rate of ~5 cm/yr). Height prediction using bone age improves over the treatment course.
Indicators for treatment: (a) age at onset <6 yr regardless of rate; (b) onset 6–8 yr with rapidly advancing bone age (>2 yr above chronological age) and/or predicted adult height significantly below genetic target; (c) significant psychosocial distress. Girls with very slowly progressing central PP and onset close to 8 yr may not need treatment if predicted height is acceptable — the decision is shared with family.
Peripheral Precocious Puberty — Cause-Directed Treatment:
- McCune-Albright syndrome: Aromatase inhibitors (anastrozole, letrozole) reduce oestrogen production from autonomous ovarian cysts; tamoxifen is an alternative. These do not fully suppress puberty but slow progression. GnRH analogues are NOT effective because the axis is already suppressed.
- Granulosa cell tumour: Surgical resection — typically unilateral salpingo-oophorectomy. Prognosis is excellent for juvenile granulosa cell tumours (low malignant potential). Follow up with inhibin B levels.
- CAH (21-hydroxylase deficiency): Hydrocortisone replacement suppresses ACTH drive and therefore reduces adrenal androgen excess. This is both the treatment and the definitive management of the underlying disease.
- Exogenous sex steroid exposure: Remove the source — stop the medication or remove the contact.
Benign Variants:
- Premature thelarche: Reassurance; Tanner staging and bone age repeated at 6 months to confirm non-progression. If progression to full precocious puberty occurs, re-investigate accordingly.
- Premature adrenarche: Reassurance; DHEAS and 17-OHP measured to exclude CAH; counsel about long-term PCOS and metabolic syndrome monitoring.
Provided image
CLINICAL PEARL
The majority (80–90%) of central precocious puberty in girls is idiopathic — but brain MRI is still mandatory in every case. The reason is that the 10–15% with an underlying CNS cause (hypothalamic hamartoma, glioma, craniopharyngioma) include tumours that are treatable and whose diagnosis significantly alters the child's care plan beyond just puberty management. In boys, the reverse is true: approximately 75% of central PP has an identifiable CNS cause, making MRI even more urgent. Hypothalamic hamartoma is the most common pathological cause — it is benign and does not require surgical resection for the PP component (GnRH analogues control puberty effectively), but it may require neurosurgical intervention if gelastic seizures are refractory.
Self-Assessment
Work through the scenarios below using the central vs peripheral classification framework before consulting the preceding sections. These scenarios are representative of the clinical situations in which precocious puberty is encountered at the final-year MBBS level, and they test the core skill of applying the LH/FSH result to correctly classify the case and then direct management accordingly. Remember: the LH/FSH level is the pivot — high LH/FSH = central (HPO axis activated), suppressed LH/FSH = peripheral (autonomous sex steroids suppressing the axis). This single result should always precede decisions about MRI or pelvic ultrasound. Practising the classification step explicitly before moving to investigation prevents the common error of ordering a brain MRI before confirming the category — MRI is only indicated after central PP is confirmed, not as a screening tool for all early puberty presentations. Each scenario below requires you to state category, then investigation, then management — in that order.
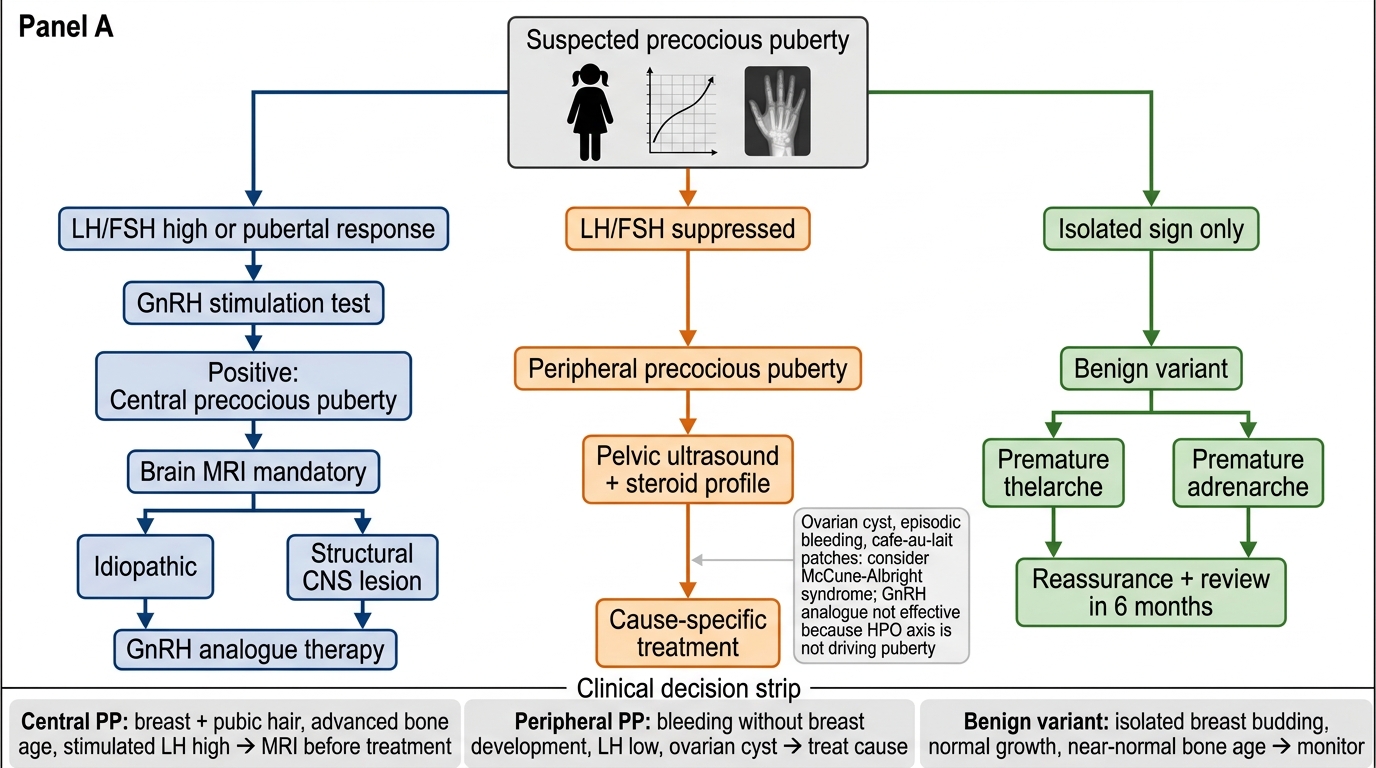
Precocious Puberty Management Flowchart
- A 7-year-old girl has breast development and pubic hair that have been progressing for 4 months. Bone age is 10 years. LH is elevated at 2.8 IU/L on GnRH stimulation test. What category is this? What investigation is now mandatory before starting treatment?
- A 5-year-old girl has episodic vaginal bleeding without breast development, café-au-lait patches on her trunk, and an ovarian cyst on ultrasound. LH is 0.08 IU/L. What is the diagnosis? Why is GnRH analogue therapy not effective in this case?
- A 7-year-old has isolated breast budding (B2) for 6 months without pubic hair, normal growth velocity, and a bone age of 7.5 years. What is the most likely diagnosis and what is your management plan?
SELF-CHECK
A 7-year-old girl is diagnosed with idiopathic central precocious puberty. Bone age is 10 years. Predicted adult height is 148 cm (her genetic target height is 165 cm). Brain MRI is normal. The most appropriate management is:
A. Reassure and monitor — idiopathic central PP resolves spontaneously
B. GnRH analogue therapy (e.g. monthly depot leuprolide) to suppress HPO axis and preserve adult height
C. Oestrogen supplementation to accelerate menarche and close epiphyses
D. Aromatase inhibitor to reduce oestrogen production
Reveal Answer
Answer: B. GnRH analogue therapy (e.g. monthly depot leuprolide) to suppress HPO axis and preserve adult height
GnRH analogue therapy is the treatment of choice for central precocious puberty when there is significant bone age advancement and a large gap between predicted and target adult height. Continuous non-pulsatile GnRH analogues downregulate pituitary GnRH receptors, suppressing LH/FSH and arresting pubertal progression. This preserves growth time and improves predicted adult height. Aromatase inhibitors are used in peripheral PP (e.g. McCune-Albright), not central PP. Oestrogen supplementation would worsen epiphyseal advancement.