Page 11 of 18
OG27.3 | Pelvic Inflammatory Disease — SDL Guide
Learning Objectives
- Describe the aetiology and polymicrobial nature of pelvic inflammatory disease including the roles of N. gonorrhoeae, C. trachomatis, and endogenous anaerobes
- Explain the pathophysiology of ascending PID and the mechanism of Fitz-Hugh-Curtis syndrome
- Apply the CDC minimum diagnostic criteria for empirical treatment of PID
- Distinguish between indications for outpatient versus inpatient treatment and state the recommended antibiotic regimens
- Describe the management of tubo-ovarian abscess including criteria for surgical intervention
- Discuss the long-term implications of PID including tubal infertility, ectopic pregnancy risk, and recurrence
INSTRUCTIONS
Pelvic inflammatory disease (PID) is the commonest serious complication of sexually transmitted infections and a major preventable cause of infertility, ectopic pregnancy, and chronic pelvic pain in women of reproductive age. Prompt diagnosis — based on clinical criteria, not requiring laboratory confirmation — and immediate treatment are essential to prevent irreversible tubal damage. This module follows the OG disease arc: clinical presentation → pathophysiology → diagnosis → management → self-assessment.
References
- CDC STI Treatment Guidelines 2021 — Pelvic Inflammatory Disease (guideline)
- DC Dutta's Textbook of Gynaecology, 7th ed., Ch 19 (Pelvic Inflammatory Disease) (textbook)
- Shaw's Textbook of Gynaecology, 16th ed., Ch 21 (Pelvic Inflammatory Disease) (textbook)
- FOGSI: Good Clinical Practice Recommendations — PID, 2020 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 24-year-old woman presents to the emergency department with a two-day history of lower abdominal pain, fever (38.4°C), and a mucopurulent vaginal discharge. She is sexually active with a new partner over the past three months and does not use barrier contraception. On examination, she has bilateral lower abdominal tenderness, bilateral adnexal tenderness on bimanual examination, and exquisite cervical motion tenderness (CMT) — pain on rocking the cervix from side to side. She winces when you gently move the cervix. Her WBC is 14,000/mm³ and CRP is elevated. You suspect pelvic inflammatory disease (PID). But then you notice she also complains of right upper quadrant pain radiating to the right shoulder — an unexpected finding. This is Fitz-Hugh-Curtis syndrome — perihepatitis from PID, where the infection has ascended to the peritoneum and spread to the hepatic capsule. How do you diagnose, classify severity, and treat this patient — and what can you do to protect her future fertility? This module gives you those answers.
WHY THIS MATTERS
Pelvic inflammatory disease is the most common serious complication of sexually transmitted infections and one of the leading preventable causes of female infertility worldwide. The WHO estimates that PID affects approximately 106 million women annually across the globe. In India, PID accounts for a substantial proportion of gynaecological outpatient consultations and emergency admissions, though its true incidence is underestimated because many cases are mild and subclinical. The consequences of inadequately treated or recurrent PID are profound and long-lasting: a single episode of PID is associated with a 15–20% risk of tubal factor infertility; three episodes raise this to over 50%. PID also increases the risk of ectopic pregnancy seven-fold — by causing partial tubal obstruction that traps a fertilised ovum in the tube. Chronic pelvic pain and dyspareunia are additional long-term sequelae. For the clinician, the critical insight is that treatment must begin immediately on clinical grounds — waiting for microbiological confirmation delays therapy and allows irreversible tubal damage to accumulate. The CDC minimum criteria for empirical treatment exist precisely to prevent this delay.
RECALL
Before proceeding, activate your prior knowledge of anatomy and microbiology. Recall the anatomical pathway from the external genitalia to the peritoneal cavity: the vagina → cervix → uterine cavity → fallopian tubes → peritoneum. This is the ascending route by which sexually transmitted pathogens travel from the lower genital tract to the upper genital tract in PID. Recall that the cervix normally acts as a mechanical barrier against ascending infection — mucus plug, acidic pH, and local immune factors. When this barrier is breached (by menstruation, instrumentation, or concurrent STI disrupting the mucosa), pathogens ascend. Recall from the STI module: N. gonorrhoeae is a gram-negative intracellular diplococcus that attaches to columnar epithelium; C. trachomatis is an obligate intracellular organism that silently damages the tube. Recall from anatomy that the hepatoduodenal ligament and hepatodiaphragmatic space are adjacent to the liver capsule — the route by which peritoneal infection from PID can spread to cause Fitz-Hugh-Curtis perihepatitis.
Clinical Presentation of PID
Pelvic inflammatory disease presents along a clinical spectrum from mild subclinical disease — detectable only on laparoscopy in women with unexplained infertility — to a life-threatening emergency with generalised peritonitis and septic shock. The clinician must be alert to the full range, because the mildest cases, if untreated, cause the same tubal scarring as the severe cases and carry equivalent long-term infertility risk. The threshold for empirical treatment must therefore be low, and this is codified in the CDC diagnostic criteria.
Symptoms of acute PID:
The characteristic presentation is a young, sexually active woman with lower abdominal pain (usually bilateral, dull-aching, and constant), mucopurulent vaginal discharge, and systemic features of infection. The onset is typically subacute — symptoms develop over 1–3 days and do not have the dramatic sudden onset of an ectopic pregnancy rupture or appendicitis. Fever (≥38.3°C) is present in moderate-to-severe cases. Irregular uterine bleeding, deep dyspareunia, and dysuria may accompany the presentation. The temporal relationship to menstruation is important: PID most commonly begins within 7 days of the onset of a menstrual period, because menstrual blood provides a culture medium and the cervical os is briefly open, facilitating ascent.
CDC minimum diagnostic criteria (2021): Empirical treatment for PID should be initiated in a sexually active woman (or any woman at risk of STIs) who has one or more of the following on pelvic examination — with no other cause identified:
- Uterine tenderness (on bimanual palpation of the uterine fundus)
- Adnexal tenderness (unilateral or bilateral, on palpation of the adnexae)
- Cervical motion tenderness (CMT) — the pathognomonic sign of PID: pain on gentle lateral movement of the cervix during bimanual examination; indicates parametrial/peritoneal involvement.
These minimum criteria do not require laboratory confirmation. The rationale: the risk of untreated PID (irreversible tubal damage) greatly outweighs the risk of treating with antibiotics when the diagnosis turns out to be wrong. Additional criteria that increase diagnostic specificity are listed in the investigations section.
Fitz-Hugh-Curtis syndrome (perihepatitis) occurs in 4–14% of women with PID and represents spread of infection from the pelvis to the hepatic capsule via the peritoneal cavity and hepatodiaphragmatic ligaments. The classic presentation is right upper quadrant (RUQ) pain — sharp, pleuritic, and sometimes radiating to the right shoulder — occurring concurrently with lower abdominal PID symptoms. Laparoscopy reveals 'violin-string' adhesions between the liver capsule (Glisson's capsule) and the anterior abdominal wall or diaphragm. The syndrome is most commonly associated with C. trachomatis (though gonorrhoea also causes it) and is an important differential for right upper quadrant pain in a young woman. A woman presenting with RUQ pain should always have a pelvic examination.
Tubo-ovarian abscess (TOA): At the severe end of the spectrum, the infection organises into a pelvic abscess involving the tube and ovary. Presentation: severe pelvic pain, high fever, systemic sepsis, and a palpable tender adnexal mass. TOA does not respond to outpatient oral antibiotics and requires hospital admission for IV antibiotic therapy.
Differential diagnosis of PID:
- Ectopic pregnancy — pelvic pain but typically unilateral, β-hCG positive, may have haemoperitoneum
- Appendicitis — RIF pain, fever, Rovsing's sign, nausea/vomiting; peritoneal signs
- Ovarian cyst accident (torsion, rupture, haemorrhage) — sudden severe unilateral pain
- Endometriosis — cyclical pain, dyspareunia, no fever
- Genital TB — chronic, no acute fever, infertility
- Urinary tract infection — dysuria, frequency, positive urine culture
SELF-CHECK
A 22-year-old sexually active woman presents with bilateral lower abdominal pain for 2 days. On examination she has uterine tenderness and cervical motion tenderness (CMT). Her WBC and CRP are normal. NAAT for gonorrhoea and chlamydia is pending. What is the correct next action?
A. Wait for NAAT results before prescribing antibiotics
B. Diagnose appendicitis and refer to surgery
C. Start empirical PID treatment immediately based on CDC minimum criteria
D. Admit for laparoscopy to confirm diagnosis before treating
Reveal Answer
Answer: C. Start empirical PID treatment immediately based on CDC minimum criteria
The CDC minimum criteria are met — CMT and uterine tenderness in a sexually active woman with no other cause identified — and empirical antibiotic treatment must begin immediately without waiting for microbiological results. Delay to confirm the diagnosis allows ongoing tubal damage. The risk of unnecessary antibiotics is far outweighed by the risk of undertreated PID. Laparoscopy is the gold standard for diagnosis but is not required before initiating treatment in straightforward clinical presentations.
Pathophysiology and Polymicrobial Aetiology
The pathophysiology of PID follows a predictable ascending sequence from the lower genital tract to the peritoneum, but the microbiology is more complex than any single-pathogen model suggests. Understanding both the route of spread and the polymicrobial nature of the infection is essential for choosing an antibiotic regimen that covers the full microbial spectrum.
Ascending infection mechanism: PID begins with colonisation of the endocervix by a sexually transmitted pathogen — most commonly N. gonorrhoeae or C. trachomatis. These 'initiating' organisms breach the cervical mucosal barrier and establish endocervicitis. Once the cervical barrier is disrupted, endogenous vaginal flora — including anaerobes (Bacteroides fragilis, Prevotella, Peptostreptococcus), aerobic gram-negative rods (E. coli), and facultative organisms (Gardnerella vaginalis, streptococci) — ascend into the uterine cavity and then into the fallopian tubes. This two-stage process — STI pathogen disrupts, endogenous flora amplifies — explains the polymicrobial nature of PID. In approximately 30–40% of cases, no STI pathogen is isolated from the upper genital tract at all; the infection is driven entirely by endogenous flora ascending through a compromised cervical barrier.
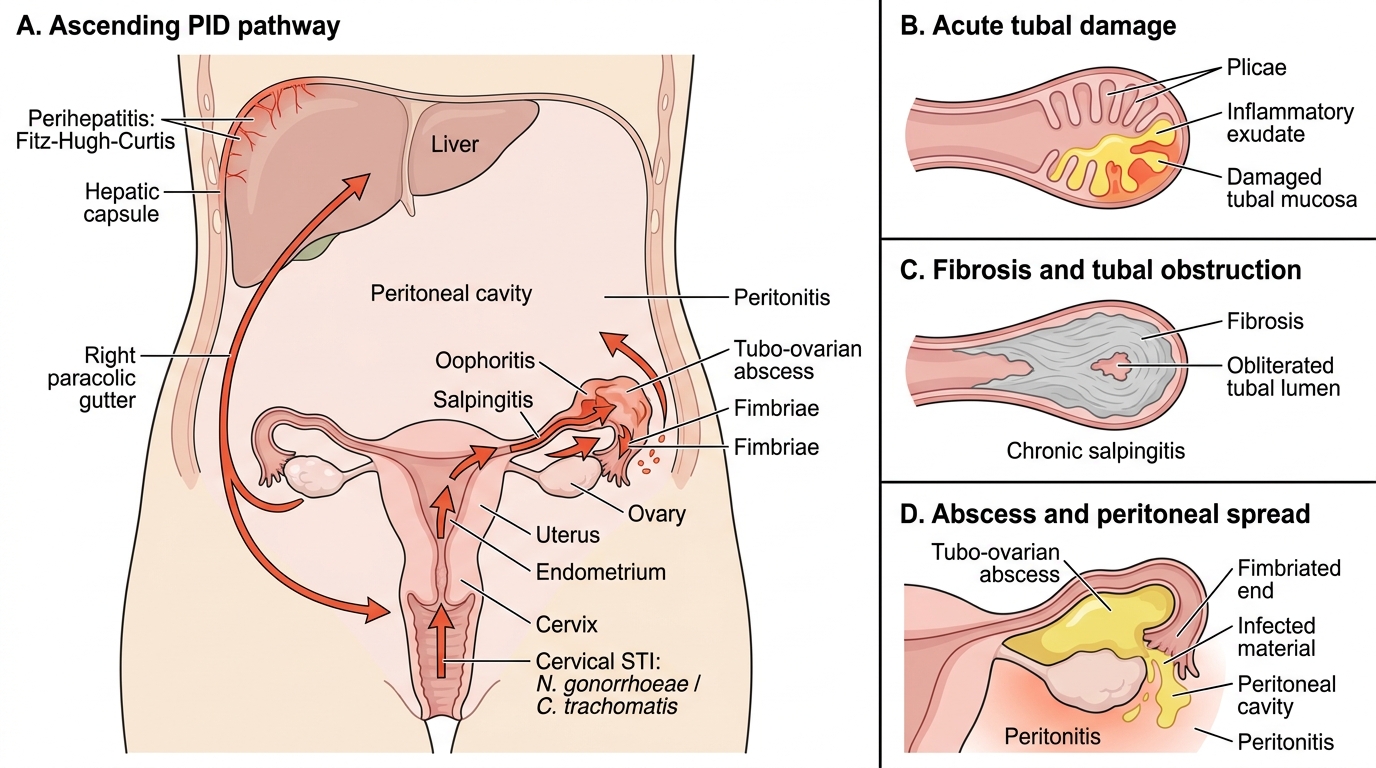
Ascending Pelvic Inflammatory Disease Pathway
Anatomical progression: Endocervicitis → endometritis (uterus) → salpingitis (fallopian tube) → oophoritis (ovary involvement from peritoneal exudate) → peritonitis (spillage of infected material from the tube's fimbriated end into the peritoneal cavity) → perihepatitis (Fitz-Hugh-Curtis) in a minority. The fallopian tube bears the brunt of the damage: its delicate mucosal folds (plicae) are destroyed by the inflammatory exudate, and the resulting fibrosis obliterates the tubal lumen.
Risk factors for PID:
- Multiple sexual partners or a new partner
- Age <25 years (columnar ectropion of the cervix is more extensive, increasing surface area vulnerable to STI pathogens)
- Previous PID (damaged cervical barrier and scarred tubes)
- Intrauterine contraceptive device insertion (especially within 3 weeks of insertion — the procedure can introduce vaginal flora into the uterine cavity)
- No barrier contraception
- Bacterial vaginosis (overgrowth of anaerobes that are the co-pathogens of PID)
Fitz-Hugh-Curtis pathogenesis: Infection spreads from the fallopian tube fimbriae into the peritoneal cavity, tracks up the paracolic gutters to the right subphrenic space, and reaches the hepatic capsule (Glisson's capsule). The resulting perihepatitis produces the characteristic 'violin-string' adhesions between the liver and the anterior abdominal wall — visible at laparoscopy. These adhesions can cause persistent RUQ pain even after the pelvic infection resolves.
SELF-CHECK
Which of the following best explains why PID treatment regimens must cover anaerobes in addition to gonorrhoea and chlamydia?
A. Anaerobes directly penetrate the cervical barrier and initiate PID independently
B. STI pathogens disrupt the cervical mucosal barrier, allowing endogenous anaerobes to ascend and amplify the infection — making PID polymicrobial
C. Anaerobic coverage prevents Fitz-Hugh-Curtis syndrome specifically
D. Anaerobes are only relevant in tubo-ovarian abscesses, not in uncomplicated PID
Reveal Answer
Answer: B. STI pathogens disrupt the cervical mucosal barrier, allowing endogenous anaerobes to ascend and amplify the infection — making PID polymicrobial
PID is a two-stage polymicrobial process: (1) STI pathogens (gonorrhoea/chlamydia) initiate infection and disrupt the cervical mucosal barrier; (2) endogenous anaerobes and facultative organisms from the vaginal flora ascend through the compromised barrier and amplify the infection in the upper genital tract. In 30-40% of cases no STI pathogen is found in the upper tract at all. This is why regimens must cover anaerobes (metronidazole or clindamycin) alongside gonorrhoea (ceftriaxone) and chlamydia (doxycycline). Anaerobic coverage is required for all PID, not just TOA.
Diagnosis and Investigations
The diagnosis of PID is primarily clinical, and the CDC has deliberately established a low threshold for empirical treatment precisely to prevent the harm of diagnostic delay. The risk of missed or delayed treatment — irreversible tubal scarring from hours of ongoing infection — far outweighs the risk of treating a woman empirically when another diagnosis turns out to be the cause. Laboratory and imaging investigations serve important but secondary roles: they increase diagnostic specificity where the clinical picture is ambiguous, identify the causative organisms for targeted therapy and epidemiological surveillance, assess disease severity and guide outpatient versus inpatient decisions, detect serious complications (particularly TOA that requires IV therapy and potential surgery), and crucially — exclude differential diagnoses that are surgical emergencies, above all ectopic pregnancy. No investigation supersedes the clinical minimum criteria as the trigger for treatment; a woman with CMT in the appropriate clinical context starts antibiotics even before swab results return. This framework is codified in the CDC 2021 guidelines.
CDC diagnostic framework (2021):
The framework distinguishes minimum criteria (trigger for empirical treatment) from additional criteria (increase specificity and support the diagnosis):
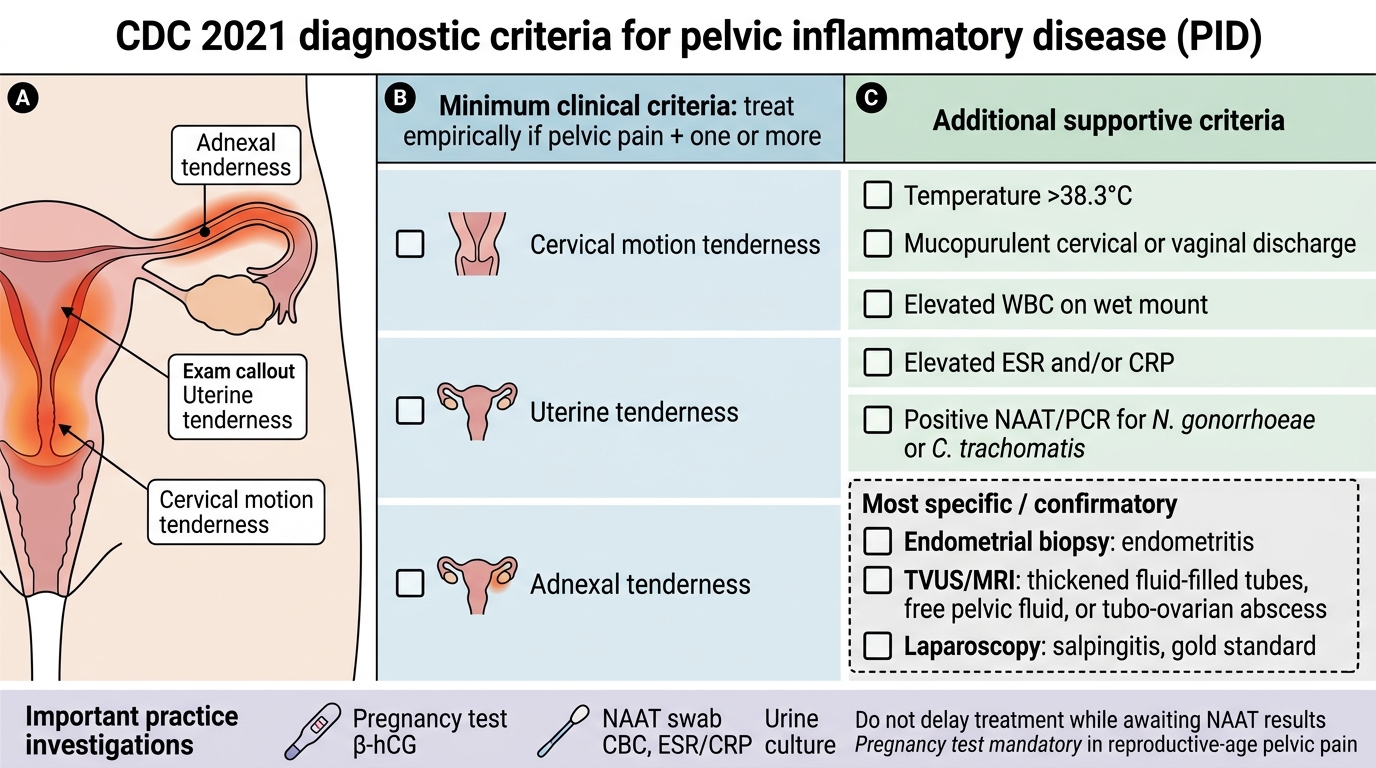
CDC 2021 Diagnostic Criteria for PID
Additional criteria that support the diagnosis:
- Temperature >38.3°C
- Cervical or vaginal mucopurulent discharge
- Elevated WBC on wet-mount of vaginal secretions
- Elevated ESR and/or CRP
- Laboratory documentation of cervical infection with N. gonorrhoeae or C. trachomatis (NAAT/PCR)
Most specific criteria (essentially confirmatory):
- Endometrial biopsy showing histopathological evidence of endometritis (plasma cells in the endometrial stroma on biopsy)
- Imaging (transvaginal ultrasound or MRI) showing thickened, fluid-filled fallopian tubes, free pelvic fluid, or a tubo-ovarian abscess
- Laparoscopy showing salpingitis — the gold standard for diagnosis of PID
Laboratory investigations in practice:
- NAAT/PCR for gonorrhoea and chlamydia from cervical or vaginal swab — positive result confirms an STI pathogen but treatment should not be withheld pending results
- Complete blood count (WBC usually elevated in moderate-severe PID; may be normal in mild cases)
- ESR and CRP — elevated; useful for monitoring treatment response
- Pregnancy test (serum/urine β-hCG) — mandatory in ALL women of reproductive age with pelvic pain to exclude ectopic pregnancy before treating as PID
- Urine culture — to exclude urinary tract infection
- Transvaginal ultrasound — to identify TOA (thick-walled complex adnexal mass with internal echoes), free fluid in the pouch of Douglas, and to guide aspiration if needed
Laparoscopy: The definitive diagnostic investigation — allows direct visualisation of red, oedematous, exudate-covered fallopian tubes (salpingitis), peritoneal fluid, and 'violin-string' perihepatic adhesions (Fitz-Hugh-Curtis). However, laparoscopy is NOT required before treatment in typical cases; it is used when the diagnosis is uncertain, when the differential includes surgical emergencies, or when severe PID (TOA) does not respond to antibiotics.