Page 5 of 18
OG27.1 | Sexually Transmitted Infections — SDL Guide
Learning Objectives
- Describe the aetiological agents and clinical features of the major sexually transmitted infections including syphilis, gonorrhoea, chlamydia, trichomoniasis, genital herpes, and chancroid
- Explain the concept and rationale of syndromic management as practised in India under NACO guidelines
- Apply the syndromic management flowcharts for genital ulcer disease and vaginal/urethral discharge syndrome
- State the recommended drug regimens for each major STI including pregnancy-safe alternatives
- Describe the differential diagnosis of genital ulcer disease and distinguish key clinical features
- Discuss the long-term implications of untreated STIs including PID, infertility, ectopic pregnancy, and neonatal transmission
- Outline prevention strategies including partner notification, condom promotion, and antenatal syphilis screening
INSTRUCTIONS
Sexually transmitted infections (STIs) are among the most common infectious diseases worldwide and carry consequences that extend far beyond the immediate illness — infertility, ectopic pregnancy, neonatal infection, HIV co-facilitation, and cervical cancer. India estimates over 6 million new STI cases annually. This module covers the major pathogens, their clinical presentations organised as syndromes, the NACO syndromic management approach, drug regimens, and long-term implications. The OG disease arc is used: clinical presentation → pathogenesis → diagnosis → management → self-assessment.
References
- NACO/MOHFW India: Guidelines for STI/RTI Management, 2014 (and 2021 update) (guideline)
- DC Dutta's Textbook of Gynaecology, 7th ed., Ch 20 (Sexually Transmitted Diseases) (textbook)
- Shaw's Textbook of Gynaecology, 16th ed., Ch 22 (Sexually Transmitted Infections) (textbook)
- WHO: Guidelines for the Management of Symptomatic STIs, 2021 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 22-year-old woman presents to the gynaecology outpatient department with a three-day history of a painful genital ulcer and significant inguinal lymph node swelling on the same side. She is sexually active with multiple partners and has not used barrier contraception consistently. On examination, there is a single, well-defined ulcer on the labia majora with an erythematous, indurated base and purulent exudate — it is exquisitely tender. A fluctuant right inguinal lymph node (bubo) is also noted. On the same day, a second patient — a 28-year-old woman referred from antenatal clinic — presents after her routine syphilis screen returned a reactive VDRL at 1:8 dilution. She is 20 weeks pregnant, has had no symptoms, and did not know she had been exposed. Both women have sexually transmitted infections, but they require very different management. How do you approach the genital ulcer — is it syphilis, herpes, or chancroid? And why is the asymptomatic seropositive pregnant woman the more dangerous case from a public health perspective? This module answers both questions.
WHY THIS MATTERS
Sexually transmitted infections represent a major global and national public health challenge. The WHO estimates 374 million new cases of curable STIs annually worldwide — including 129 million chlamydia, 82 million gonorrhoea, 7.1 million syphilis, and 156 million trichomoniasis cases. In India, NACO estimates over 6 million STI/RTI episodes per year. The burden is compounded by the fact that STIs are largely asymptomatic (particularly chlamydia and early syphilis), facilitating unrecognised transmission. For the clinician, STIs are important for several reasons: they cause direct morbidity (infertility, ectopic pregnancy, chronic pelvic pain); they facilitate HIV transmission (genital ulcers increase HIV transmission 3–5 fold); and untreated maternal infection causes serious neonatal morbidity (congenital syphilis, neonatal conjunctivitis from gonorrhoea, neonatal herpes encephalitis). India's NHM mandates antenatal syphilis screening for precisely this reason. In examination, STI syndromic management and genital ulcer differential diagnosis are high-yield, frequently tested topics.
RECALL
Before proceeding, recall your microbiological foundations. Treponema pallidum is a spirochaete — it cannot be cultured on routine media and is visualised by dark-field microscopy. Neisseria gonorrhoeae is a gram-negative intracellular diplococcus identifiable on gram stain of urethral discharge as kidney-shaped diplococci within neutrophils. Chlamydia trachomatis is an obligate intracellular bacterium — it requires living cells to replicate and cannot be grown on ordinary culture. Herpes simplex virus establishes latency in dorsal root ganglia after primary infection, causing recurrent outbreaks on reactivation. Trichomonas vaginalis is a flagellated protozoan, not a bacterium — this matters for treatment (metronidazole, not antibiotics). Recall the concept of opportunistic pathogens exploiting breached epithelium: genital ulcers from any cause increase susceptibility to HIV by disrupting the mucosal barrier. These foundations contextualise every aspect of STI diagnosis and management.
Clinical Presentation and Syndromic Approach
Sexually transmitted infections present in a limited number of recognisable clinical syndromes, and this pattern forms the basis of the syndromic management approach adopted by NACO (National AIDS Control Organisation) and the WHO. The syndromic approach was developed for resource-limited settings where laboratory diagnosis is unavailable, delayed, or costly — it allows treatment to be initiated at the very first clinical encounter, dramatically reducing loss to follow-up and ongoing community transmission. Rather than waiting for pathogen identification, the clinician uses the clinical syndrome together with epidemiological risk factors (number of partners, type of sexual contact, condom use, prior STI history, and whether the partner has symptoms) to prescribe a standardised regimen that covers all likely pathogens responsible for that syndrome. This approach was validated in multiple field studies across sub-Saharan Africa and South Asia showing that syndromic treatment at first visit reduces STI prevalence comparably to laboratory-confirmed treatment, with the added benefit of not losing the window of opportunity. India's NACO guidelines operationalise this through standardised flowcharts for five core syndromes.
The five NACO syndromes and their typical presentations:
1. Genital Ulcer Disease (GUD): one or more ulcers on the external genitalia, perineum, or perianal region. The character of the ulcer — painful vs painless, single vs multiple, indurated vs soft, clean vs purulent base — guides the differential.
2. Urethral Discharge Syndrome: mucopurulent or purulent discharge from the urethra in males; dysuria. Caused predominantly by gonorrhoea and/or chlamydia.
3. Vaginal Discharge Syndrome: abnormal vaginal discharge (amount, colour, consistency, odour), with or without vulval irritation. Caused by gonorrhoea, chlamydia, Trichomonas vaginalis, and bacterial vaginosis (the latter is not sexually transmitted but included in the syndrome).
4. Lower Abdominal Pain Syndrome (in women): pelvic pain, dyspareunia, cervical motion tenderness — suggesting ascending STI (PID). Covered in the PID module.
5. Inguinal Bubo Syndrome: tender inguinal lymphadenopathy ± fluctuance (bubo). Caused by LGV (Chlamydia L1-L3) or Haemophilus ducreyi (chancroid).
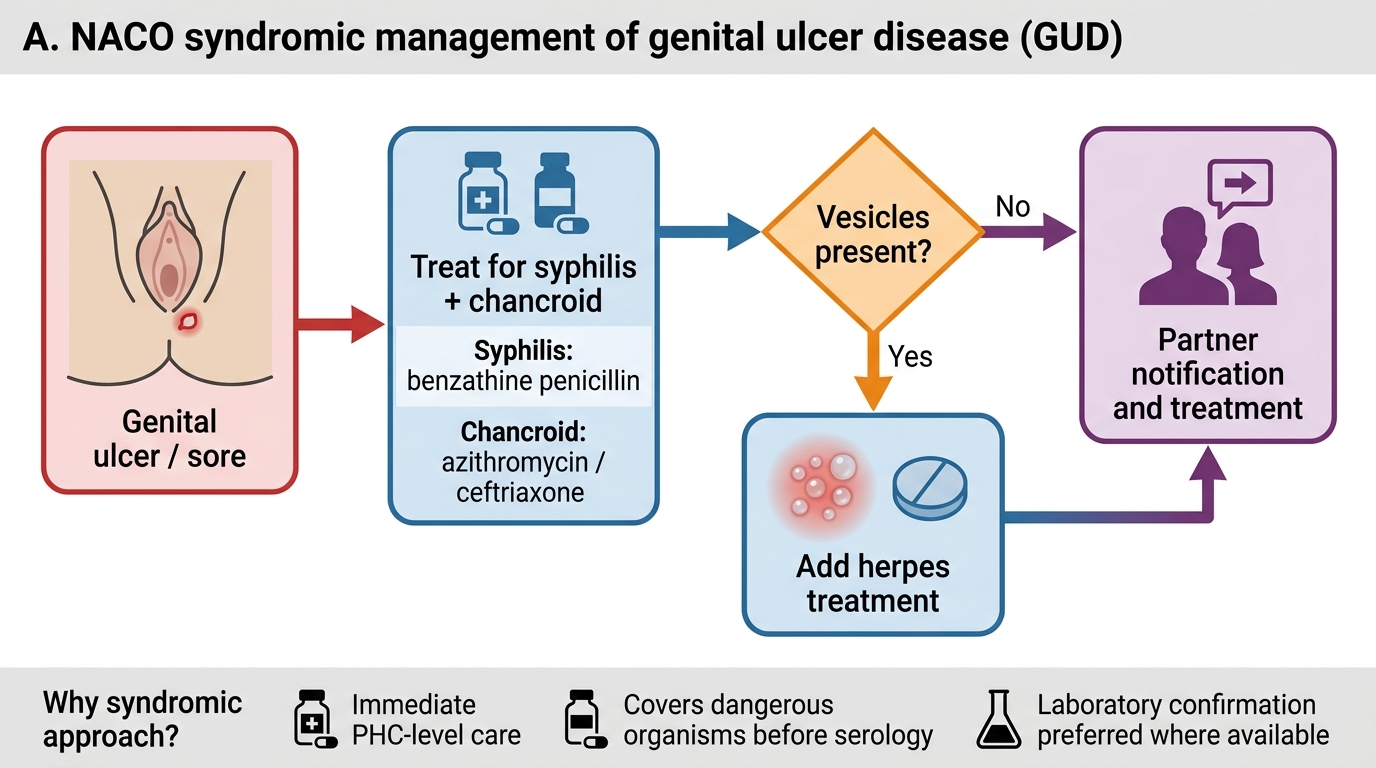
NACO Syndromic Management of Genital Ulcer Disease
The syndromic approach has significant advantages in the Indian context: it is immediately applicable at PHC level, it ensures treatment of the most dangerous organisms (particularly syphilis) without waiting for serology, and it mandates partner notification and treatment. Its limitation is over-treatment when the pathogen is known and sensitive to a narrower agent. The approach does not replace laboratory diagnosis where available — laboratory confirmation is always preferred for legal, epidemiological, and resistance-monitoring purposes.
Pathology and Pathogenesis of Key STIs
Understanding the pathogenesis of each major STI explains its clinical behaviour — why syphilis is painless and systemic, why chancroid is painful and localised, why chlamydia is so often silent, and why herpes recurs. The tissue damage mechanisms also explain the long-term sequelae, particularly the inflammatory scarring that leads to tubal occlusion and infertility.
Syphilis (Treponema pallidum): The spirochaete penetrates intact or abraded mucosa and disseminates via lymphatics and blood within hours of infection. Primary syphilis produces the classic chancre — a painless, indurated, clean-based ulcer with a firm, rolled edge, at the site of inoculation. It is painless because there is no acute inflammatory exudate; the immune response is delayed and cell-mediated. The chancre heals spontaneously in 3–6 weeks. Untreated, secondary syphilis follows (6–8 weeks later) with haematogenous dissemination: the classic maculopapular rash affecting palms and soles, condylomata lata, mucous patches, generalised lymphadenopathy, and constitutional symptoms. Latent syphilis follows (early latent <1 year from infection; late latent ≥1 year or unknown duration). Tertiary syphilis (gumma, cardiovascular, neurosyphilis) occurs in 30% of untreated cases years later. The VDRL/RPR are non-treponemal tests (measure non-specific cardiolipin antibody); TPHA/FTA-ABS are treponemal-specific confirmatory tests.
Gonorrhoea (Neisseria gonorrhoeae): Attaches to columnar epithelium via pili and surface proteins, then invades and triggers a brisk neutrophilic response — producing the characteristic mucopurulent discharge. Gram stain of the discharge shows gram-negative intracellular diplococci within PMNs. In women, the endocervix is the primary site; urethritis co-exists in most. Ascending spread to the endometrium and fallopian tubes causes PID, salpingitis, and eventually tubal occlusion and infertility. Ophthalmia neonatorum (neonatal conjunctivitis) is acquired during passage through an infected birth canal — a preventable cause of childhood blindness. The major contemporary challenge is antimicrobial resistance — N. gonorrhoeae has sequentially acquired resistance to penicillin, tetracyclines, fluoroquinolones (ciprofloxacin no longer recommended in India), and now emerging cephalosporin resistance makes dual therapy (ceftriaxone + azithromycin) mandatory.
Chlamydia (Chlamydia trachomatis serovars D-K): Obligate intracellular organism that invades columnar epithelium and replicates within host cells. Most infections are asymptomatic — making it the most prevalent bacterial STI globally and a major cause of silent PID and infertility. When symptomatic: mucopurulent cervicitis, urethral syndrome, or Bartholin's abscess. The elementary body (EB) is the infectious, non-replicating form; the reticulate body (RB) replicates intracellularly. LGV (serovars L1-L3) causes aggressive lymphadenitis and buboes.
Chancroid (Haemophilus ducreyi): Produces a painful (contrast with syphilis), soft, non-indurated ulcer with ragged, undermined edges and a dirty/grey/yellow purulent base — the classic 'soft sore'. The regional lymph nodes are tender and may suppurate to form a fluctuant bubo. The pain is a cardinal distinguishing feature from syphilitic chancre. Gram-negative coccobacilli in chains ('school of fish' pattern) on smear.
Trichomoniasis (Trichomonas vaginalis): Flagellated protozoan adheres to vaginal epithelium; the alkaline environment it produces (vaginal pH rises to >4.5) impairs normal Lactobacillus colonisation and facilitates bacterial vaginosis. Classic presentation: frothy, yellow-green, malodorous vaginal discharge with vaginal erythema and 'strawberry cervix' (colpitis macularis — punctate haemorrhages on the cervix, best seen on colposcopy). Motile trichomonads are seen on wet-mount microscopy.
Genital herpes (HSV-2, less commonly HSV-1): HSV-2 infects genital mucosal cells, replicates, and then establishes latency in sacral dorsal root ganglia (S2-S4). Primary infection is often the most severe: multiple painful vesicles that rupture to form shallow, exquisitely tender ulcers covering the external genitalia; systemic symptoms (fever, malaise, inguinal lymphadenopathy) are common. Recurrent episodes (reactivation) are milder and shorter. Shedding occurs even without visible lesions (asymptomatic shedding), which is a major transmission risk. Neonatal herpes acquired at delivery is a devastating complication.
Provided image
SELF-CHECK
A 30-year-old man presents with a single painless genital ulcer with a clean, indurated base and firm rolled edges. Which STI is the most likely diagnosis?
A. Chancroid (Haemophilus ducreyi)
B. Primary syphilis (Treponema pallidum)
C. Genital herpes (HSV-2)
D. Lymphogranuloma venereum (Chlamydia L1-L3)
Reveal Answer
Answer: B. Primary syphilis (Treponema pallidum)
The painless, indurated, clean-based ulcer with firm rolled edges is the classic primary syphilitic chancre. Chancroid (H. ducreyi) produces a painful, soft, non-indurated ulcer with a purulent/dirty base — contrasting directly with syphilis. Genital herpes causes multiple, shallow, very painful vesicles/ulcers. LGV typically causes a transient small ulcer that heals quickly, with prominent buboes as the primary presentation. Painless + indurated + clean base = syphilis until proven otherwise.
Differential Diagnosis and Investigations
The differential diagnosis of genital ulcer disease is one of the most clinically important and examination-relevant challenges in STI medicine. The correct diagnosis drives the correct treatment — and the treatments differ substantially across the aetiologies. Moreover, co-infection with more than one pathogen is not uncommon, particularly in high-prevalence settings, and missing a concurrent syphilis in a patient treated only for herpes is a serious error. The clinician's approach must be systematic: begin with the macroscopic character of the ulcer itself (painful or painless, single or multiple, indurated or soft, clean or purulent, base, edge, size), then assess the regional lymph nodes (tender or non-tender, fluctuant or firm, unilateral or bilateral), then consider the systemic features (fever, rash, constitutional symptoms suggesting secondary syphilis), and finally integrate the epidemiological context (travel history, partner symptoms, previous STIs). This clinical synthesis, combined with targeted investigations, allows accurate diagnosis and guides both pathogen-specific and syndromic treatment.
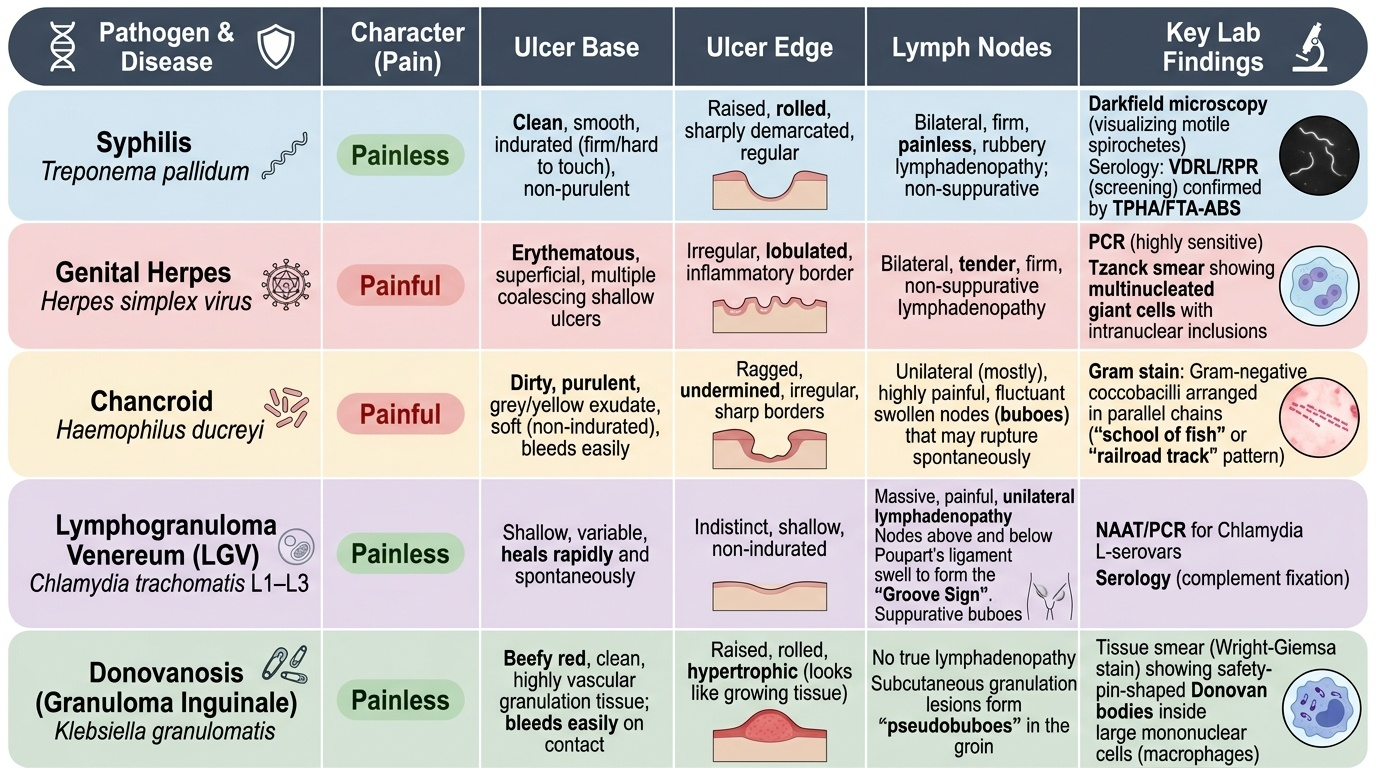
Clinical differential of genital ulcer disease — key distinguishing features:
| Feature | Syphilis | Herpes | Chancroid | LGV | Donovanosis |
|---|---|---|---|---|---|
| Pain | Painless | Very painful | Painful | Painless (ulcer) | Painless |
| Number | Usually single | Multiple | Single/multiple | Small, heals fast | Progressive |
| Base | Clean, indurated | Shallow, red | Purulent/necrotic | Variable | Beefy-red, bleeds |
| Edges | Firm, rolled | Irregular | Ragged, undermined | — | Raised |
| Lymph nodes | Rubbery, non-tender | Tender bilateral | Tender, bubo | Bubo (grooved sign) | Pseudobubo |
| Key lab | Dark-field/VDRL | Tzanck/PCR | Culture/PCR | C. trachomatis PCR | Donovan bodies |
Investigations for STI diagnosis:
- Syphilis: (a) Dark-field microscopy of serous fluid from the primary chancre — most sensitive for primary syphilis; (b) VDRL/RPR (non-treponemal screening tests — titres correlate with disease activity, used for treatment response monitoring); (c) TPHA / FTA-ABS (treponemal-specific confirmatory tests — remain positive for life, not used for monitoring treatment response). A reactive VDRL should always be confirmed with a treponemal test. VDRL can give biological false positives (pregnancy, autoimmune disease, malaria).
- Gonorrhoea: Gram stain of urethral discharge (gram-negative intracellular diplococci, sensitivity ~95% in males, lower in females). NAAT (PCR) is the gold standard — high sensitivity and specificity for both symptomatic and asymptomatic infection. Culture allows antimicrobial sensitivity testing — important for resistance surveillance.
- Chlamydia: NAAT/PCR (gold standard — most sensitive). Cell culture is possible but expensive and slow. Serology (complement fixation) for LGV.
- Trichomoniasis: Wet-mount microscopy of vaginal discharge — motile trichomonads with characteristic tumbling motility; sensitivity ~60-70%. NAAT is more sensitive (>95%). Vaginal pH >4.5 is supportive.
- Herpes: Tzanck smear — multinucleated giant cells with intranuclear inclusions (insensitive). Viral PCR of lesion swab is the most sensitive and specific. HSV-2 IgG antibody testing (serology) confirms past infection but cannot diagnose current episode timing.
- Chancroid: Gram stain ('school of fish' coccobacilli), culture on specialised media — technically difficult. Diagnosis often clinical + exclusion.
All patients with one STI should be screened for co-infections — particularly HIV, syphilis, and hepatitis B/C. An HIV test is mandatory for all STI patients as per NACO guidelines.
SELF-CHECK
A patient's VDRL returns reactive at 1:16 dilution. Which of the following is the correct next step?
A. Start benzathine penicillin G 2.4 MU IM immediately — VDRL is diagnostic
B. Confirm with a treponemal test (TPHA or FTA-ABS) before treating
C. Repeat the VDRL in 4 weeks — a single positive may be a false positive
D. Order dark-field microscopy to identify treponemes
Reveal Answer
Answer: B. Confirm with a treponemal test (TPHA or FTA-ABS) before treating
A reactive VDRL/RPR is a non-treponemal screening test that can give biological false positives (pregnancy, autoimmune disease, malaria, viral infections). The standard protocol is to CONFIRM a reactive non-treponemal test with a treponemal-specific test (TPHA or FTA-ABS) before diagnosing syphilis and treating. However, in a pregnant woman with a reactive VDRL, if a treponemal test is not immediately available, treatment should NOT be withheld pending confirmation — treat presumptively to prevent congenital syphilis (NHM antenatal protocol). Dark-field microscopy is used on primary ulcer exudate, not on serum.