Page 17 of 24
OG30.2 | Hyper-Androgenism — SDL Guide
Learning Objectives
- Enumerate the causes of hyperandrogenism and classify them by source (ovarian, adrenal, exogenous, idiopathic)
- Assess the severity of hirsutism using the modified Ferriman-Gallwey scoring system and identify virilisation as a red-flag feature
- Select and interpret investigations to determine the cause of hyperandrogenism, including the role of 17-OHP and the ACTH stimulation test
- Outline the management of hyperandrogenism according to the underlying cause, including symptom-directed and cause-directed strategies
INSTRUCTIONS
Hyperandrogenism — excess androgen activity in a woman — is a common presentation in gynaecology, endocrinology, and general practice. Its causes range from the extremely common and benign (PCOS-related hirsutism) to the rare and serious (androgen-secreting tumour causing rapid virilisation). Distinguishing between these ends of the spectrum requires a systematic clinical and biochemical approach. This module builds on the PCOS SDL to give you a broader differential framework, equip you to score hirsutism objectively, and guide you through the investigation and management of each cause.
References
- DC Dutta's Textbook of Gynaecology, 8th ed., Ch. 27 (textbook)
- Shaw's Textbook of Gynaecology, 17th ed., Ch. 25 (textbook)
- ESHRE International Evidence-Based Guideline for PCOS, 2023 (guideline)
- Azziz R et al. The prevalence and features of the polycystic ovary syndrome in an unselected population. J Clin Endocrinol Metab 2004; 89:2745-2749 (journal)
- Speiser PW et al. Congenital Adrenal Hyperplasia. NEJM 2003; 349:776-788 (journal)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Priya, a 19-year-old college student, attends your gynaecology outpatient clinic distressed about progressive coarse hair on her upper lip, chin, and chest over the past eight months. She has always had slightly irregular periods, but recently they have become very sparse — only two in the last six months. Her older sister had PCOS. However, what strikes you most is that Priya's voice has noticeably deepened compared with a photograph she shows you from eighteen months ago, and her clitoris appears enlarged on examination. These findings concern you: this is not the gradual hirsutism typical of PCOS. You have twelve minutes before the next patient. How will you triage this presentation and decide how urgently Priya needs further investigation?
WHY THIS MATTERS
Hyperandrogenism is among the most frequently encountered endocrine presentations in gynaecological practice. The vast majority of cases — roughly 70-80% — are due to PCOS and are managed with lifestyle measures and oral contraceptives. However, a small but critical proportion represent serious pathology: androgen-secreting tumours of the ovary or adrenal gland that can double testosterone levels in weeks and cause rapid, progressive virilisation. The ability to distinguish the slow, familiar hirsutism of PCOS from the rapid virilisation of a tumour is a potentially life-saving clinical skill. Additionally, late-onset congenital adrenal hyperplasia (CAH) is a treatable genetic mimic of PCOS found in 4-8% of hyperandrogenic women — diagnosing it changes management entirely. This module ensures you can apply a systematic framework to any woman presenting with signs of androgen excess.
RECALL
Recall from the PCOS SDL that androgens in women derive from two main sources: the ovary (theca cells producing testosterone and androstenedione, stimulated by LH) and the adrenal gland (zona reticularis producing DHEAS and androstenedione, stimulated by ACTH). Both sources are subject to negative feedback, but different regulatory mechanisms. Recall also the role of 5α-reductase from your Biochemistry studies — this peripheral enzyme in hair follicles and skin converts testosterone to the more potent dihydrotestosterone (DHT), which acts on the androgen receptor to stimulate terminal hair growth and sebaceous gland activity. The sensitivity of individual hair follicles to DHT varies by body site, explaining the characteristic distribution of hirsutism (androgen-sensitive areas: face, chest, abdomen, inner thighs).
Clinical Assessment: Hirsutism, Virilisation, and Red Flags
The clinical assessment of a woman presenting with excess hair begins with a precise distinction between two concepts that are sometimes conflated: hirsutism and virilisation. Hirsutism is the growth of coarse, pigmented, terminal hair in an androgen-sensitive distribution in a woman — it is common, distressing, and usually due to relatively modest androgen excess. Virilisation describes a constellation of masculinising features reflecting sustained, markedly elevated androgen levels: it is a red flag that demands urgent investigation for an androgen-secreting tumour.
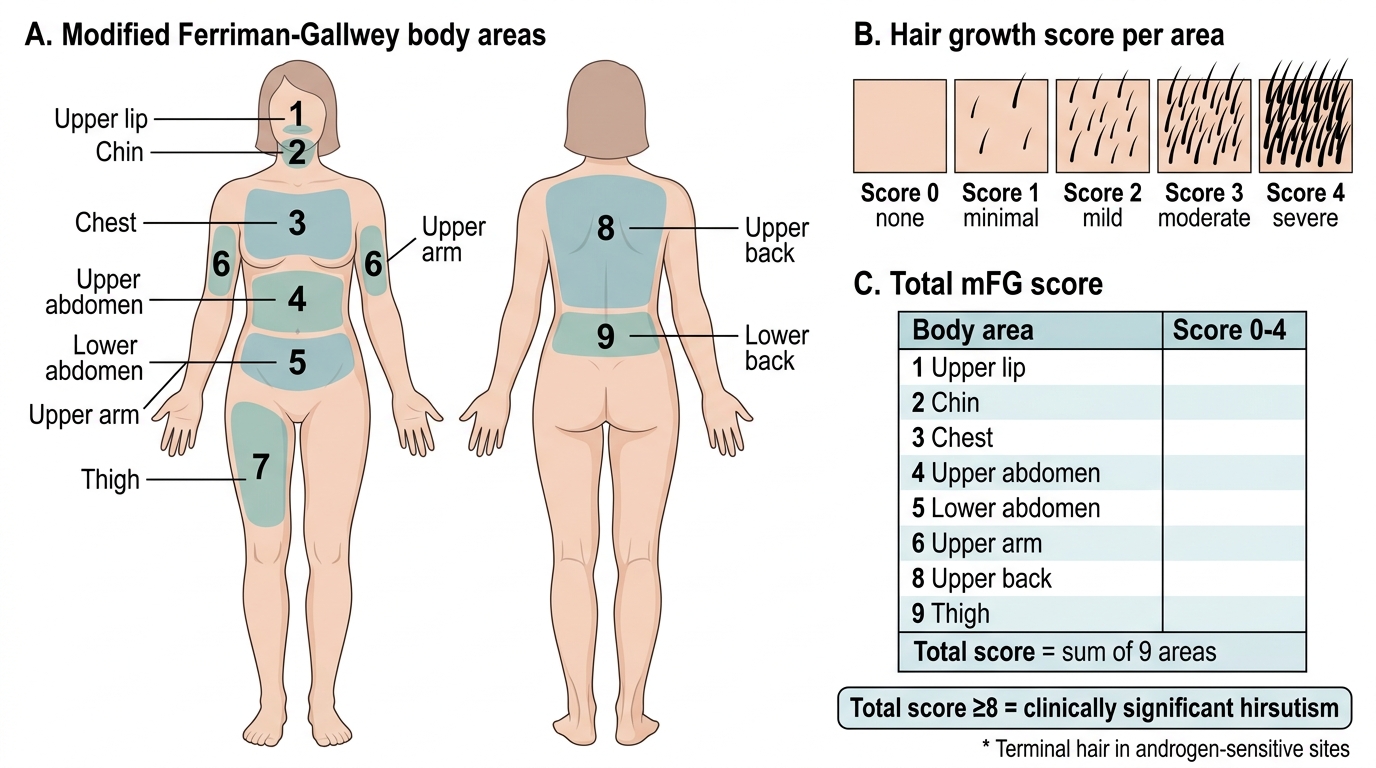
The standard tool for quantifying hirsutism is the modified Ferriman-Gallwey (mFG) score. It evaluates nine body areas — upper lip, chin, chest, upper abdomen, lower abdomen, upper arm, thigh, upper back, and lower back — each scored from 0 (no terminal hair) to 4 (frankly male pattern). A total score of ≥8 is the clinically accepted threshold for significant hirsutism. The mFG score serves several purposes: it provides an objective baseline, allows monitoring of treatment response over time, and helps differentiate ethnic variation in hair growth (some South Asian and Mediterranean women have higher baseline mFG scores without pathological androgen excess) from genuinely elevated androgen-driven growth.
Virilisation red flags — features that should trigger immediate investigation for an androgen-secreting tumour:
- Clitoromegaly (clitoral length >1 cm or clitoral index >35 mm²) — the most specific sign
- Deepening of the voice (laryngeal changes driven by high testosterone)
- Male-pattern alopecia (frontotemporal hair recession)
- Breast atrophy
- Increased muscle bulk and loss of female fat distribution
The tempo of onset is as important as the individual signs: PCOS-related hirsutism develops over years; androgen-secreting tumours typically cause rapidly progressive symptoms over months. Any woman with virilisation or symptom progression over less than 12 months requires urgent biochemical and imaging workup.
Modified Ferriman-Gallwey Scoring System
Pathophysiology of Androgen Excess
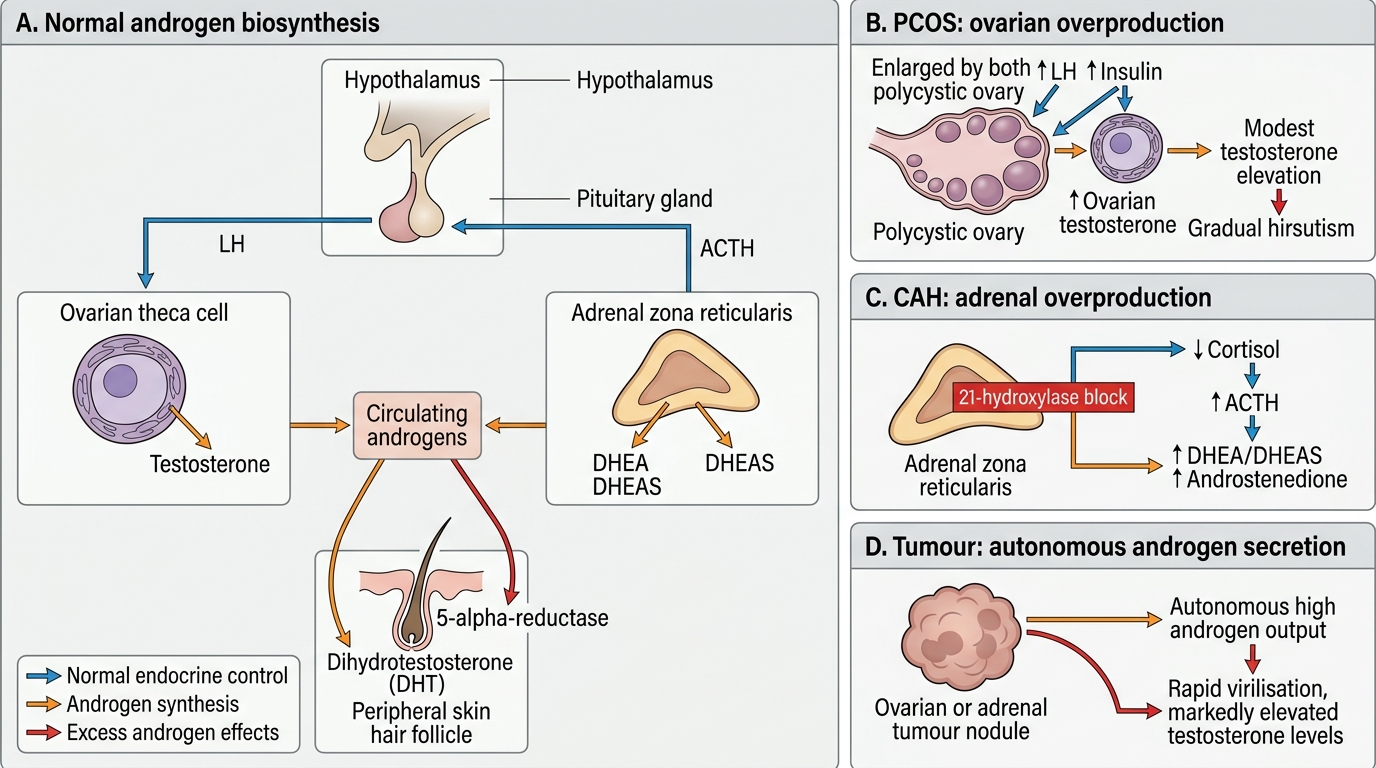
Understanding the pathophysiology of hyperandrogenism requires integrating the normal androgen axis with the points at which each disease disrupts it. In a normal reproductive-age woman, total testosterone is typically 15-70 ng/dL, with the majority bound to SHBG and albumin; only 1-3% is free and biologically active. DHEAS is almost exclusively adrenal in origin (normal 80-350 µg/dL). Androstenedione is produced roughly equally by ovary and adrenal.
At the level of the hair follicle, 5α-reductase type 1 and type 2 convert testosterone to dihydrotestosterone (DHT), which binds the androgen receptor with approximately five times greater affinity than testosterone itself. DHT stimulates the hair follicle to transition from the vellus (fine, unpigmented) to the terminal (coarse, pigmented) growth state in androgen-sensitive sites. In idiopathic hirsutism — where serum androgens are entirely normal — the pathology lies at this conversion step: increased skin 5α-reductase activity generates locally elevated DHT despite normal circulating testosterone.
At the level of the ovary, PCOS results from hyperinsulinaemia up-regulating CYP17A1 in theca cells, driving excess testosterone and androstenedione synthesis (reviewed in the PCOS SDL). An androgen-secreting ovarian tumour bypasses normal regulatory control entirely, producing testosterone autonomously and in large quantities.
At the level of the adrenal gland, late-onset CAH arises from partial deficiency of 21-hydroxylase (CYP21A2), the enzyme that converts 17-OHP to 11-deoxycortisol. The block causes 17-OHP to accumulate and be shunted into the androgen pathway (via CYP17A1), raising DHEAS and androstenedione. In Cushing syndrome, ACTH-driven adrenal hyperplasia stimulates both cortisol and androgen production. In adrenal carcinoma, unregulated tumour cells secrete large quantities of DHEAS and androstenedione.
Androgen Biosynthesis and Causes of Hyperandrogenism
Causes of Hyperandrogenism: A Systematic Approach
Organising the causes of hyperandrogenism by source — ovarian, adrenal, exogenous, or idiopathic — provides a clinically actionable framework. Each category has a characteristic biochemical signature that guides investigation. Because the treatment differs dramatically across categories, the most important initial task is identifying which compartment is driving the androgen excess.
1. Ovarian causes
PCOS is by far the commonest cause, accounting for 70-80% of women with hyperandrogenism. The clinical and biochemical features are detailed in the PCOS SDL. In brief: oligomenorrhoea + mild-to-moderate hirsutism + modestly elevated testosterone + insulin resistance + polycystic ovarian morphology on USG. Onset is insidious and gradual.
Androgen-secreting ovarian tumours — including Sertoli-Leydig cell tumours (arrhenoblastoma) and, rarely, granulosa-theca cell tumours with androgen activity — produce rapidly progressive virilisation. Testosterone is typically markedly elevated (>200 ng/dL). These tumours are rare (prevalence <0.2% of adnexal masses) but represent a gynaecological emergency because of the speed of virilisation and potential for malignancy.
2. Adrenal causes
Late-onset (non-classic) congenital adrenal hyperplasia (CAH) due to 21-hydroxylase deficiency is the most important single-gene cause to exclude. It is found in 4-8% of women presenting with hyperandrogenism (higher in Ashkenazi Jewish, Hispanic, and certain Mediterranean populations). Clinical presentation is indistinguishable from PCOS. The diagnostic signature is an elevated morning 17-OHP (>2 ng/mL in the follicular phase), confirmed by ACTH stimulation test.
Cushing syndrome (cortisol excess) from any cause — pituitary ACTH adenoma (Cushing disease), adrenal adenoma, or ectopic ACTH — produces weight gain, hypertension, striae, bruising, menstrual irregularity, and androgen excess. The distinguishing features are the cushingoid habitus (central obesity, moon facies, buffalo hump) and hypertension — features absent in PCOS.
Adrenal carcinoma is rare but important: very high DHEAS (>700 µg/dL) with rapid-onset virilisation strongly suggests adrenal origin.
3. Exogenous causes
Anabolic steroids, androgens used for gender-affirming hormone therapy, and some progestogens with androgenic activity (norethisterone, levonorgestrel at high dose) can cause iatrogenic hyperandrogenism. A careful drug history is essential.
4. Idiopathic hirsutism
In approximately 5-15% of women with hirsutism, serum androgens are entirely normal, menstrual cycles are regular, and polycystic ovarian morphology is absent. The mechanism is increased skin 5α-reductase activity. This is a diagnosis of exclusion and does not carry the metabolic or endometrial risks of PCOS.
⚑ AI image — pending faculty review (auto-QA score 3/10; best of 3 attempts)
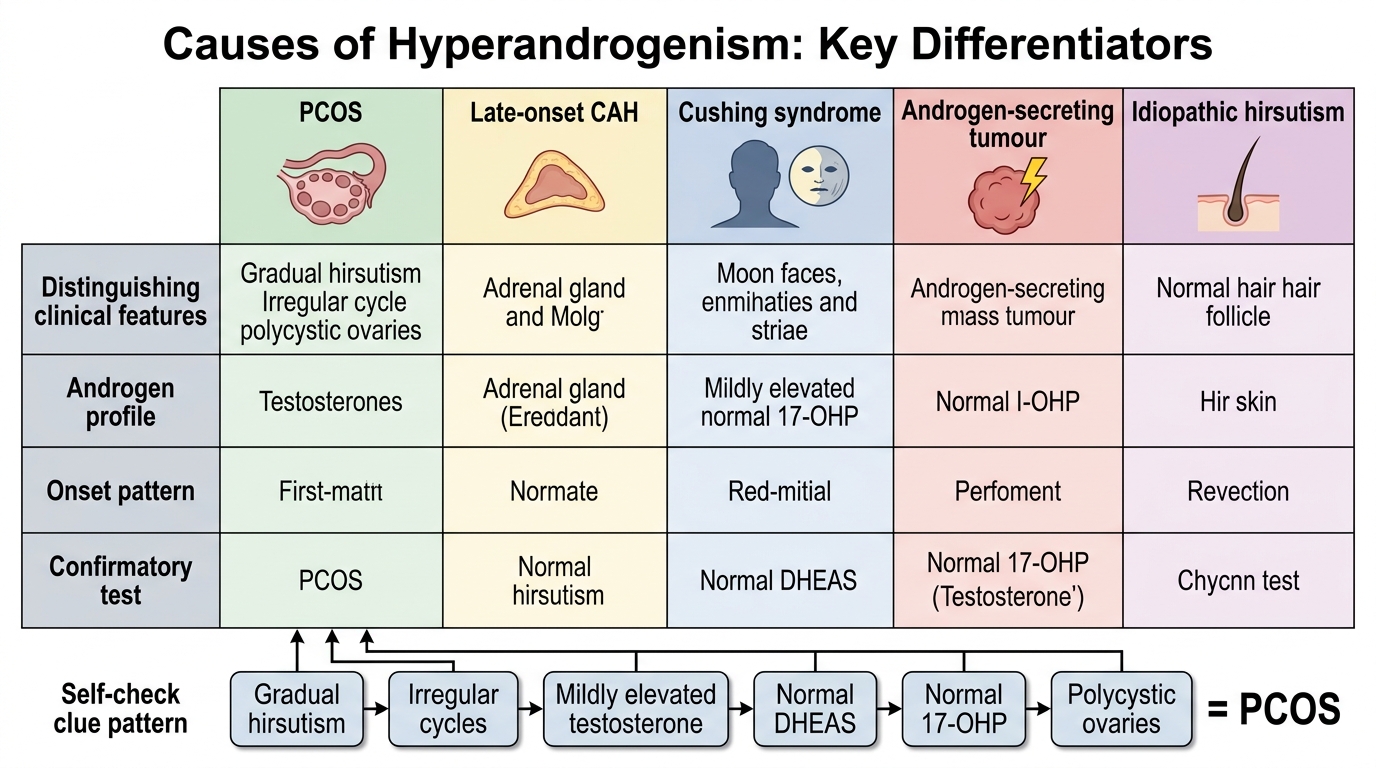
Differential Diagnosis of Hyperandrogenism
SELF-CHECK
A 23-year-old woman has had gradually increasing hirsutism over 3 years with irregular cycles. Her total testosterone is 95 ng/dL, DHEAS is 280 µg/dL, prolactin and TSH are normal, morning 17-OHP is 1.2 ng/mL. Ultrasound shows 24 follicles per ovary. What is the most likely diagnosis?
A. Late-onset congenital adrenal hyperplasia
B. Androgen-secreting ovarian tumour
C. Polycystic ovary syndrome
D. Idiopathic hirsutism
Reveal Answer
Answer: C. Polycystic ovary syndrome
This presentation meets Rotterdam criteria for PCOS: oligo-ovulation (irregular cycles), biochemical hyperandrogenism (elevated testosterone), and polycystic ovarian morphology (24 follicles per ovary ≥20 threshold). The gradual onset over 3 years, mildly elevated testosterone, normal DHEAS, and normal 17-OHP (rules out CAH) all point to PCOS. The normal 17-OHP excludes late-onset CAH. The follicle count and normal DHEAS argue against an adrenal or tumour cause.