Page 7 of 24
OG28.3 | Ovulation Induction — SDL Guide
Learning Objectives
- Classify anovulatory infertility using the WHO three-group system and describe the characteristic hormonal profile of each group
- Explain the mechanism of action of letrozole and clomiphene citrate in inducing ovulation
- Describe the dose, regimen, and monitoring requirements for letrozole, clomiphene citrate, and gonadotrophins
- State the evidence basis for letrozole as first-line ovulation induction in PCOS (PPCOS II trial)
- Classify ovarian hyperstimulation syndrome by severity and describe the principles of prevention and management
INSTRUCTIONS
Anovulatory infertility — failure to ovulate — accounts for approximately 25–35% of female infertility and is among the most pharmacologically treatable causes. This SDL covers the spectrum of agents used to induce ovulation, from the outpatient oral regimens of letrozole and clomiphene to monitored injectable gonadotrophin cycles, with emphasis on drug selection, monitoring protocols, and the critical complication of ovarian hyperstimulation syndrome that every clinician managing these patients must be able to recognise.
References
- DC Dutta's Textbook of Gynaecology, 8th edition, Ch 18 (Ovulation Induction) (textbook)
- Shaw's Textbook of Gynaecology, 17th edition, Ch 23 and Ch 24 (textbook)
- Legro RS et al. Letrozole versus clomiphene for infertility in PCOS (NICHD PPCOS II). NEJM 2014;371:119–129 (journal)
- NICE Fertility Guideline CG156, updated 2017 — Ovulation induction section (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 26-year-old woman with PCOS and 14 months of primary infertility sits in your OPD. Her cycles are 45–70 days, she has hirsutism and acanthosis nigricans, her BMI is 29 kg/m², and her semen analysis is normal. She has already spent two months on metformin prescribed by a local doctor with no improvement in cycle regularity. She asks: 'My friend was given some tablets and got pregnant. What will you give me?' The next decision you make — which agent, at what dose, with what monitoring — will determine whether she conceives in the next 3–6 months or embarks on a prolonged and expensive treatment journey. This SDL equips you to make that decision correctly.
WHY THIS MATTERS
Ovulation induction is one of the most impactful pharmacological interventions in gynaecological practice: a woman who is not ovulating cannot conceive naturally, but the right drug at the right dose in the right patient produces a conceptus without any assisted reproduction technology. For a condition as prevalent as PCOS — affecting 5–10% of women of reproductive age — this represents an enormous clinical opportunity. At the same time, ovulation induction carries real risks: multiple pregnancy (twins, triplets) and ovarian hyperstimulation syndrome (OHSS), a potentially life-threatening complication in severe cases. Understanding the pharmacology, protocols, monitoring requirements, and complication management is not optional — it is a core clinical competency for anyone who will manage women with infertility.
RECALL
Recall from Physiology: the hypothalamic-pituitary-ovarian (HPO) axis operates on negative feedback. Oestrogen produced by developing follicles feeds back to the hypothalamus and pituitary to suppress GnRH and FSH secretion — this is the mechanism by which the dominant follicle suppresses further recruitment once it has established its lead. Also recall aromatase: the enzyme in granulosa cells that converts androgens (androstenedione, testosterone) to oestrogens (oestrone, oestradiol). This step is the target of letrozole. Recall also the classification of hypothalamic-pituitary-ovarian dysfunction: WHO Group I (hypogonadotrophic — low FSH, low LH, low oestrogen; brain not driving the ovary); WHO Group II (normogonadotrophic — normal or elevated FSH/LH, normal oestrogen; most PCOS patients); WHO Group III (hypergonadotrophic — elevated FSH, low oestrogen; depleted ovaries).
Clinical Presentation: When is Ovulation Induction Needed?
Ovulation induction (OI) is indicated whenever anovulation is the confirmed or contributing cause of infertility, and the problem is amenable to stimulation of the ovary to produce and release a dominant follicle. The clinical presentation varies significantly by the underlying cause of anovulation, and recognising the characteristic features of each group guides both the investigation and the choice of agent.
WHO Group I — hypogonadotrophic hypogonadism: these women present with amenorrhoea and the hormonal profile shows low FSH, low LH, and low oestradiol. The ovary is quiescent because the hypothalamic-pituitary drive is absent or severely reduced. Common causes include: hypothalamic amenorrhoea from significant weight loss (BMI <17.5 kg/m²), extreme athletic training, psychological stress (anorexia nervosa, elite gymnasts, long-distance runners), or structural hypothalamic lesions; Kallmann syndrome (congenital GnRH deficiency with anosmia); and pituitary hypogonadism (tumour, infarction, Sheehan syndrome). These patients require exogenous gonadotrophins because they lack the endogenous FSH needed to drive follicular development, and no oral agent works without pituitary responsiveness.
WHO Group II — normogonadotrophic anovulation: by far the most common group in clinical practice, accounting for ~85% of anovulatory infertility. The hallmark is polycystic ovary syndrome (PCOS), though hypothyroidism and hyperprolactinaemia — once treated — also fall into this functional category. In PCOS, the HPG axis is intact but dysregulated: FSH is normal or slightly low, LH is often elevated relative to FSH, and the excess intraovarian androgens from LH-driven theca cells arrest follicular development at the antral stage. These women respond well to oral agents because their HPG axis is functional.
WHO Group III — hypergonadotrophic hypogonadism: elevated FSH reflects the pituitary's futile attempts to stimulate a depleted or unresponsive ovary. The causes include premature ovarian insufficiency (POI), prior chemotherapy/radiotherapy, Turner syndrome, and surgical oophorectomy. Ovulation induction with standard agents is largely ineffective in this group; oocyte donation is the primary pathway to pregnancy.
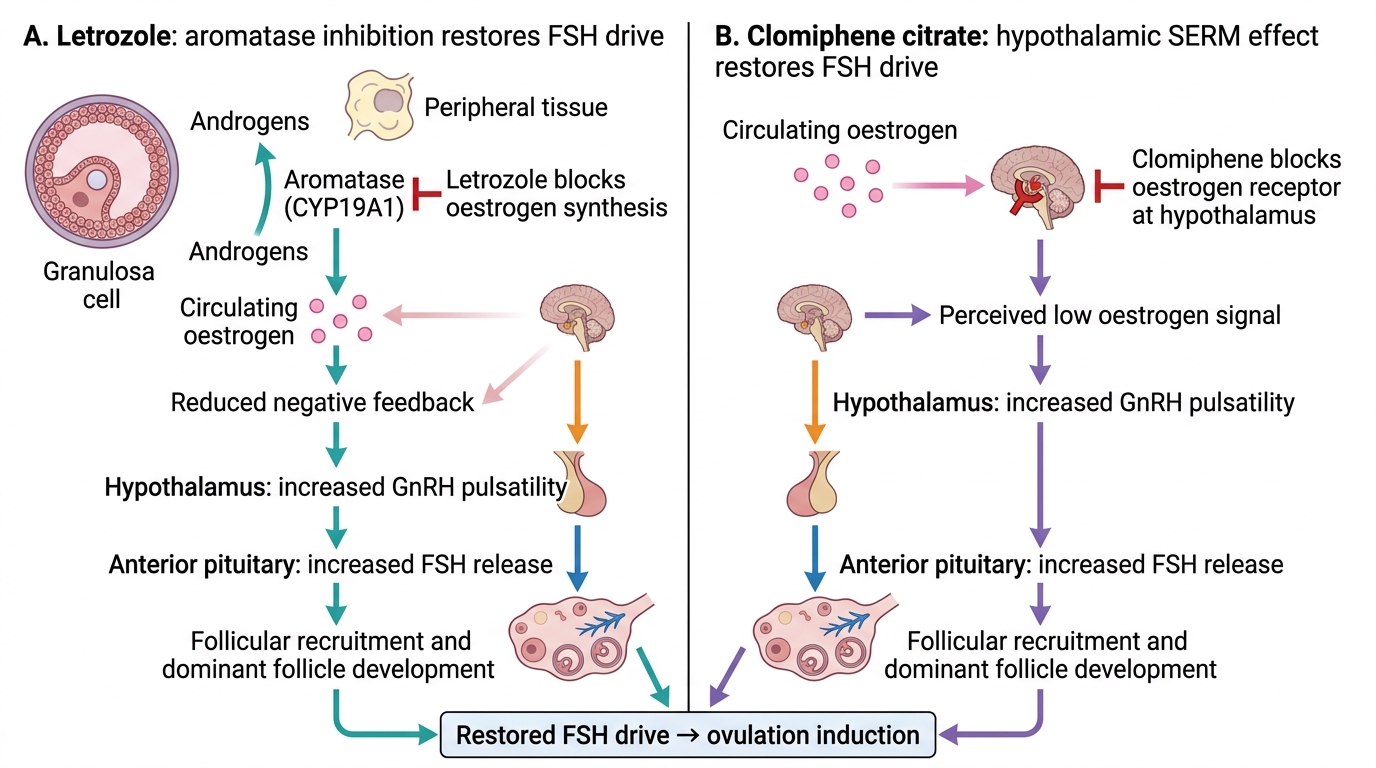
Restoration of FSH Drive by Letrozole and Clomiphene
Pathophysiology of Anovulation and the Rationale for Ovulation Induction
Understanding why each drug works — the step in the reproductive cascade it targets — is essential for rational drug selection and for explaining the treatment to patients. The central insight is that most anovulatory infertility in WHO Group II women arises from a failure of the normal FSH pulse to achieve sufficient amplitude to drive one follicle to dominance and ovulation, not from a complete absence of HPG axis activity. Both oral OI agents work by increasing the FSH signal, but through entirely different mechanisms.
Letrozole is a third-generation aromatase inhibitor that reversibly inhibits the aromatase enzyme (CYP19A1), which catalyses the conversion of androgens (androstenedione, testosterone) to oestrogens in granulosa cells, adipose tissue, liver, and other peripheral sites. By reducing peripheral and ovarian oestrogen synthesis, letrozole decreases the negative feedback on the hypothalamus and anterior pituitary, thereby increasing GnRH pulsatility and FSH release. The result is enhanced follicular recruitment in the early follicular phase. Critically, as the dominant follicle grows and resumes its own oestrogen synthesis, the negative feedback is gradually restored — this self-limiting mechanism reduces the risk of multi-follicular development compared to clomiphene, explaining the lower multiple pregnancy rate. Letrozole's half-life is approximately 45 hours; it is metabolised and cleared by the time significant follicular growth occurs (days 5–7 of the cycle), avoiding the persistent anti-oestrogenic effects that characterise clomiphene.
Clomiphene citrate is a selective oestrogen receptor modulator (SERM) that competes with endogenous oestrogen for binding to oestrogen receptors (ER) at the hypothalamus and pituitary. By occupying the receptor without full agonist activity, it prevents the negative feedback that oestrogen would normally exert, deceiving the hypothalamus into perceiving low oestrogen and increasing GnRH pulsatility — thereby driving FSH secretion. However, clomiphene's very long half-life (~5–7 days for its active isomers) means that it persists well into the follicular and periovulatory phases, where its anti-oestrogenic effects on the cervical mucus (making it thicker and less sperm-permeable) and endometrium (thin, less receptive) can paradoxically impair the very conception it was meant to facilitate. This peripheral anti-oestrogenic effect is one reason letrozole has better live birth rates despite similar ovulation rates.
Gonadotrophins (injectable FSH preparations — uFSH, rFSH — or hMG which contains FSH + LH activity) directly stimulate granulosa cell proliferation and follicular development, bypassing the hypothalamus and pituitary entirely. They are therefore effective in all three WHO groups (though futile in WHO Group III). The downside is the narrow therapeutic window: too little gonadotrophin and there is no response; too much and multiple follicles develop simultaneously, dramatically increasing the risk of multiple pregnancy and OHSS. Hence, gonadotrophin cycles require close monitoring by serial transvaginal USS and serum oestradiol measurements.
SELF-CHECK
A 30-year-old woman with PCOS is starting ovulation induction. Which of the following correctly describes the mechanism of action of letrozole?
A. It blocks oestrogen receptors at the hypothalamus, reducing negative feedback and increasing FSH
B. It inhibits the aromatase enzyme, reducing oestrogen synthesis and thereby increasing FSH
C. It directly stimulates the pituitary to produce more FSH regardless of oestrogen levels
D. It suppresses LH hypersecretion in PCOS by acting on the anterior pituitary
Reveal Answer
Answer: B. It inhibits the aromatase enzyme, reducing oestrogen synthesis and thereby increasing FSH
Letrozole is an aromatase inhibitor, not a SERM. It blocks the CYP19A1 aromatase enzyme, reducing conversion of androgens to oestrogens. The resulting fall in oestrogen reduces hypothalamic-pituitary negative feedback, causing a reflex rise in FSH that drives follicular development. Option A describes clomiphene citrate's mechanism (SERM at hypothalamus). Direct pituitary stimulation describes gonadotrophins. LH suppression is not letrozole's primary mechanism.
Ovulation Induction Agents: Regimens, Monitoring, and Selection
The selection of an ovulation induction agent depends primarily on the WHO group of anovulation, the woman's BMI and insulin resistance status, prior treatment history, and access to monitoring facilities. The following is the evidence-based algorithm for WHO Group II (PCOS), which constitutes the majority of clinical practice.
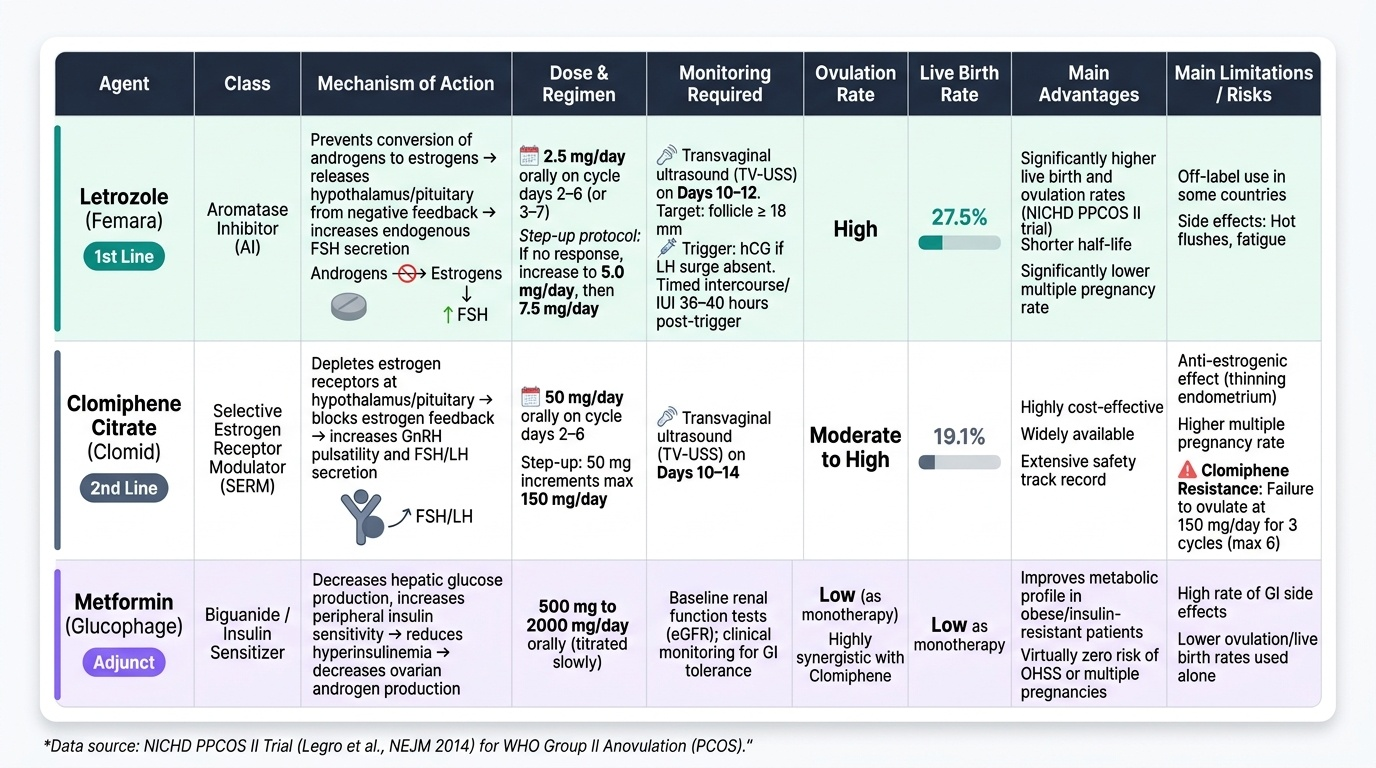
Letrozole is the first-line agent for ovulation induction in PCOS since the landmark NICHD PPCOS II trial (Legro et al., NEJM 2014), which randomised 750 anovulatory PCOS women to letrozole or clomiphene and demonstrated higher cumulative live birth rates (27.5% vs 19.1%), higher ovulation rates, and significantly lower multiple pregnancy rates with letrozole. Regimen: 2.5 mg/day orally on cycle days 2–6 (or days 3–7; either convention acceptable). If no ovulation response, increase to 5 mg/day in the next cycle, then 7.5 mg/day. Monitor by transvaginal USS on day 10–12 to confirm dominant follicle development (target ≥18 mm). Ovulation can be triggered with hCG 5,000–10,000 IU IM or 250 µg rHCG SC if the LH surge has not occurred spontaneously. Intercourse or IUI is timed 36–40 hours after trigger.
Clomiphene citrate remains widely used globally due to lower cost and wider availability, and is a reasonable second-line agent where letrozole is unavailable or not licensed. Regimen: 50 mg/day on cycle days 2–6; increase by 50 mg increments each cycle to a maximum of 150 mg/day. Ovulation response monitoring: USS on day 10–14. Clomiphene resistance is defined as failure to ovulate despite 150 mg/day for 3 cycles — at this point, adjunctive metformin should be considered (especially in obese/insulin-resistant women), or a switch to gonadotrophins. Maximum recommended duration of clomiphene therapy is 6 cycles.
Metformin as an adjunct improves ovulation rates in clomiphene-resistant PCOS women with obesity (BMI >30 kg/m²) by reducing insulin resistance and lowering hyperinsulinaemia — the key driver of excess androgen production in PCOS. Dose: 500 mg BD to 500 mg TDS, titrated over 4–6 weeks. Alone, it is less effective than letrozole for ovulation induction (Moll et al., NEJM 2006). Most evidence supports it as adjunct to clomiphene in resistant cases, or combined with lifestyle modification in obese PCOS.
Gonadotrophins (injectable FSH ± LH): indicated when oral agents have failed after adequate trial (3–6 cycles), or in WHO Group I women who lack pituitary responsiveness. Step-up protocol: a low starting dose (37.5–75 IU/day rFSH, injected subcutaneously) with dose increments every 7–14 days guided by USS monitoring, aiming for monofollicular development. Strict monitoring is mandatory: serial USS (every 2–3 days once follicle >10 mm) and serum oestradiol. Cycle cancellation criteria: if >3 dominant follicles (≥14 mm) develop simultaneously, the cycle should be abandoned to avoid OHSS and high-order multiple pregnancy.
Laparoscopic ovarian drilling (LOD): a surgical second/third-line option for clomiphene-resistant PCOS in which diathermy or laser punctures (typically 4–10 punctures per ovary, 600 J per puncture) reduce ovarian androgen production and restore cyclicity. Advantages: induces ovulation without multiple pregnancy risk, no OHSS; effects last up to 2 years. Disadvantages: requires general anaesthesia, carries surgical risk, and may cause ovarian damage if excessive.
Provided image
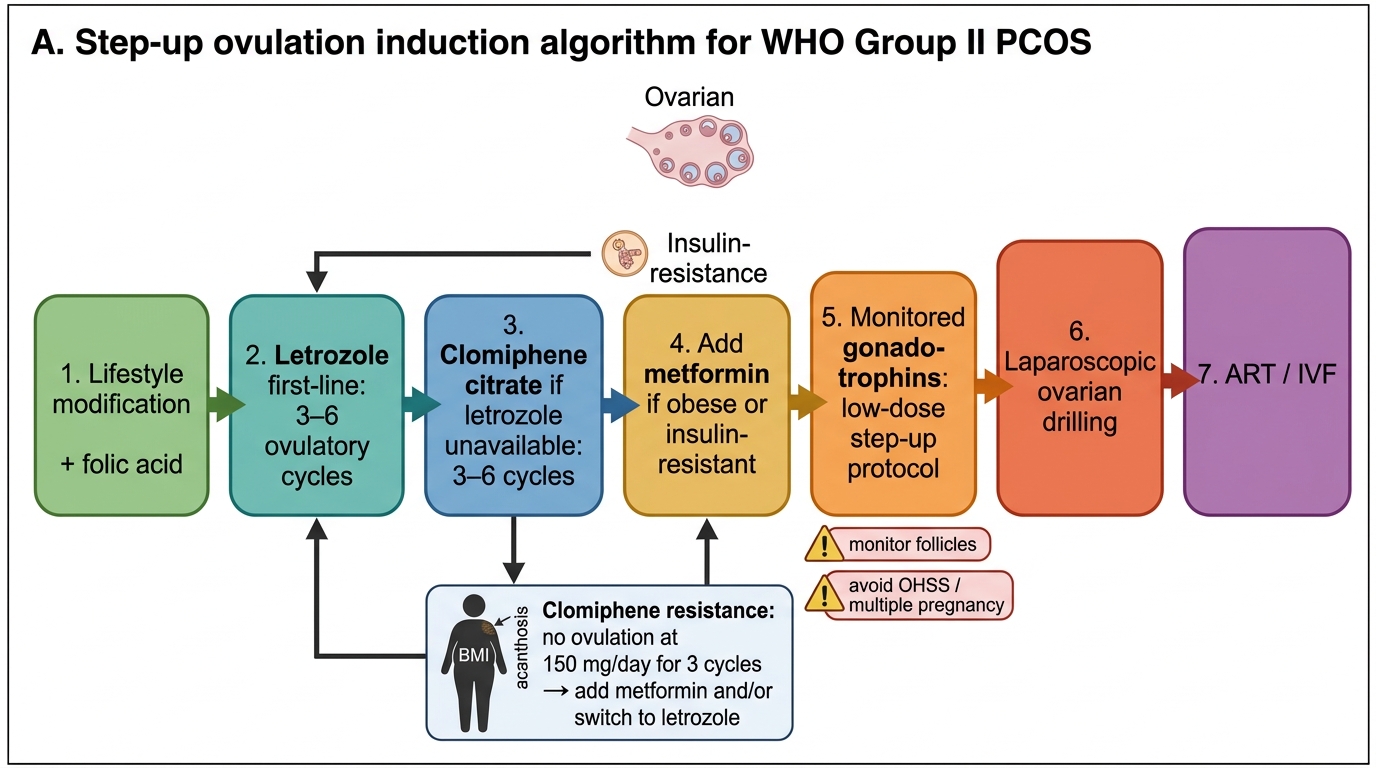
Step-up Ovulation Induction in WHO Group II PCOS
SELF-CHECK
A 28-year-old woman with PCOS has been on clomiphene citrate 150 mg/day for 3 cycles with confirmed anovulation on follicle tracking. Her BMI is 32 kg/m² and she has acanthosis nigricans. What is the most appropriate next step?
A. Continue clomiphene citrate at the same dose for 3 more cycles
B. Switch to injectable gonadotrophins immediately
C. Add metformin to her current regimen and/or switch to letrozole
D. Proceed directly to IVF without further oral agents
Reveal Answer
Answer: C. Add metformin to her current regimen and/or switch to letrozole
This is clomiphene resistance (failure to ovulate at maximum dose of 150 mg for 3 cycles). In an obese, insulin-resistant woman (BMI 32, acanthosis nigricans), adding metformin is the next appropriate step as it targets the underlying insulin resistance driving PCOS anovulation. Switching to letrozole is also appropriate if not yet tried. Continuing the same clomiphene dose is futile. Injectable gonadotrophins are a further escalation after oral agent failure. IVF is premature at this stage.