Page 5 of 24
OG28.2 | Tubal Patency Assessment — SDL Guide (Part 2)
Interpretation of Findings
Accurate interpretation of tubal patency findings requires understanding the normal appearance, the spectrum of abnormalities, and the clinical significance of each finding — including which findings require confirmation before acting on them.
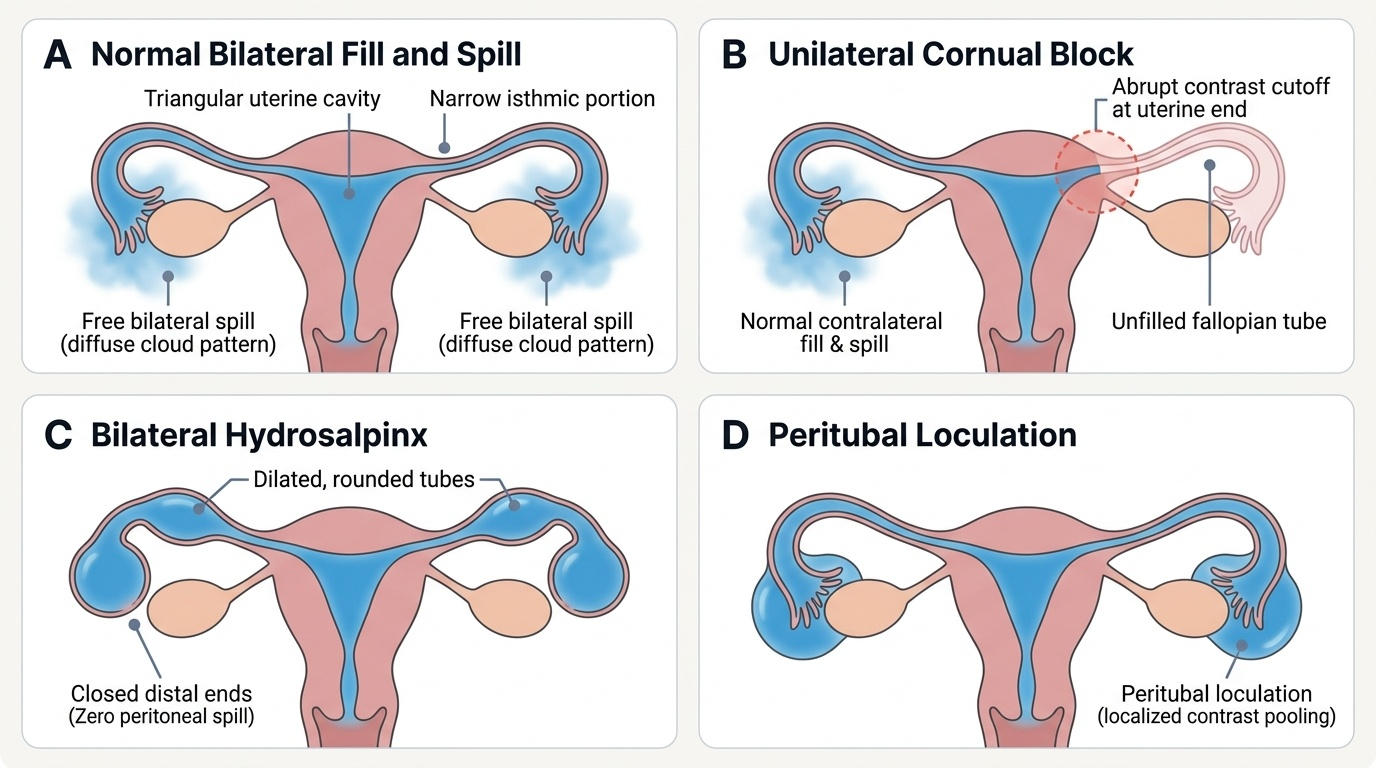
Normal findings on HSG: the uterine cavity appears as a triangular filling defect between the two cornua; contrast flows bilaterally along the length of each tube (the isthmic portion appears narrow and uniform; the ampullary portion widens progressively); contrast spills freely from the fimbriated ends to outline the peritoneal cavity, often forming a 'cloud' around the ovary. Both tubes must fill and both must spill to be reported as normal.
Proximal (cornual) tubal block on HSG: contrast does not enter the tube at the cornual junction — the filling defect is at the uterine end of the tube. As noted above, approximately 15% of apparent proximal blocks on HSG are false positives due to muscular spasm; these can sometimes be overcome by a larger volume of contrast or by repeating the study after antispasmodic premedication (hyoscine butylbromide). True proximal obstruction is confirmed at laparoscopy if dye does not enter the tube even under gentle pressure. Causes include intraluminal debris, endometrial polyp at the ostium, intrauterine synechiae, or salpingitis isthmica nodosa (SIN — nodular tubal wall thickening from fibrosis).
Distal tubal block / hydrosalpinx on HSG: contrast fills the tube but does not spill; instead, the tube appears dilated and rounded — the classic hydrosalpinx appearance. The absence of fimbrial detail and the dilated, smooth tube wall indicate that the distal end is sealed, most commonly from prior PID. A hydrosalpinx is clinically significant beyond infertility: its fluid is embryotoxic and if diagnosed before IVF, the affected tube must be treated (salpingectomy or proximal clipping) to avoid reducing implantation rates.
Peritoneal adhesions are not visible on HSG but cause characteristic findings at laparoscopy: restricted tube mobility, contrast spill into a localised pool rather than free peritoneal spread ('localised spill' or 'peritubal loculation'), or tethering of the fimbriae to the ovary or pelvic sidewall.
Intrauterine findings incidentally identified on HSG: a filling defect in the uterine cavity may represent a polyp, submucous fibroid, adhesion, or rarely a bicornuate/septate uterus. These require further evaluation by hysteroscopy for definitive diagnosis and treatment.
Provided image
SELF-CHECK
HSG in a 33-year-old infertile woman shows bilateral tubal filling with contrast, but both tubes appear uniformly dilated and there is no spill from either fimbriated end. What is the most likely diagnosis?
A. Bilateral proximal tubal block from cornual spasm
B. Bilateral hydrosalpinges from distal tubal occlusion
C. Normal variant — some tubes are wider than others
D. Salpingitis isthmica nodosa (SIN)
Reveal Answer
Answer: B. Bilateral hydrosalpinges from distal tubal occlusion
Bilateral tubal filling with contrast (ruling out proximal block) but no spill, combined with dilatation of the tubes, is the classic HSG appearance of bilateral hydrosalpinges. The tubes are filled but their distal ends are sealed — most commonly from prior PID. SIN causes nodular irregularity in the isthmic segment, not uniform dilatation. This finding has major management implications: both hydrosalpinges should be treated before IVF.
Restoration of Tubal Patency — Surgical Options
When tubal disease is confirmed, management depends on the site of obstruction, the severity of damage, the woman's age and ovarian reserve, and whether IVF is available and accessible. Surgery to restore tubal patency is most beneficial when the damage is limited and the remaining tube has functional potential; it is least beneficial — and IVF should be preferred — when tubal damage is severe, bilateral, or combined with peritubal adhesions and poor tubal function.
Tubal cannulation for proximal block is the treatment of choice for true cornual or isthmic obstruction confirmed at laparoscopy or HSG repeat. It is performed fluoroscopically (selective salpingography with cannulation using a flexible guidewire) or hysteroscopically. The guidewire is advanced along the tubal lumen to break down intraluminal debris or mild adhesions. Success in restoring patency occurs in approximately 75–85% of cases; intrauterine pregnancy rates of approximately 25–35% follow successful cannulation. It is an outpatient procedure with minimal morbidity.
Salpingostomy creates a new opening at the distal end of a hydrosalpinx by making multiple incisions at the sealed fimbrial end and everting the edges (cuff salpingostomy). This is performed laparoscopically. Post-operative tubal patency rates of approximately 50–60% are reported, but intrauterine pregnancy rates are much lower (~25–35%) because mucosal damage within the hydrosalpinx impairs ciliary function even after the tube is reopened. The risk of ectopic pregnancy after salpingostomy is significantly elevated (~15–20%). Salpingostomy is therefore reserved for mild-to-moderate unilateral hydrosalpinx in women who specifically wish to pursue natural conception or cannot access IVF.
Fimbrioplasty is performed for fimbrial agglutination or phimosis (partial closure) without a true hydrosalpinx — the fimbriae are preserved and freed from adhesions. Outcomes are better than salpingostomy because mucosal integrity is more likely to be preserved.
Salpingectomy or proximal tubal ligation/clipping is the procedure of choice for bilateral severe hydrosalpinges before IVF. The hydrosalpinx fluid contains cytokines (IL-1, TNF-α) and prostaglandins that are directly embryotoxic; retrograde reflux into the uterine cavity impairs endometrial receptivity. Multiple RCTs and a landmark Cochrane review confirm that salpingectomy or tubal occlusion before IVF significantly improves live birth rates in women with hydrosalpinx.
Microsurgical tubal anastomosis is performed for reversal of tubal sterilisation (in women who previously underwent tubal ligation and now desire fertility). Success is highest when: the remaining tube length is ≥4 cm, the woman is under 35 years of age, the method of sterilisation was clips or rings (preserving tube length), and the anastomosis is at the isthmus–isthmus or isthmus–ampulla level. Success rates can reach 60–80% for intrauterine pregnancy in optimal candidates.
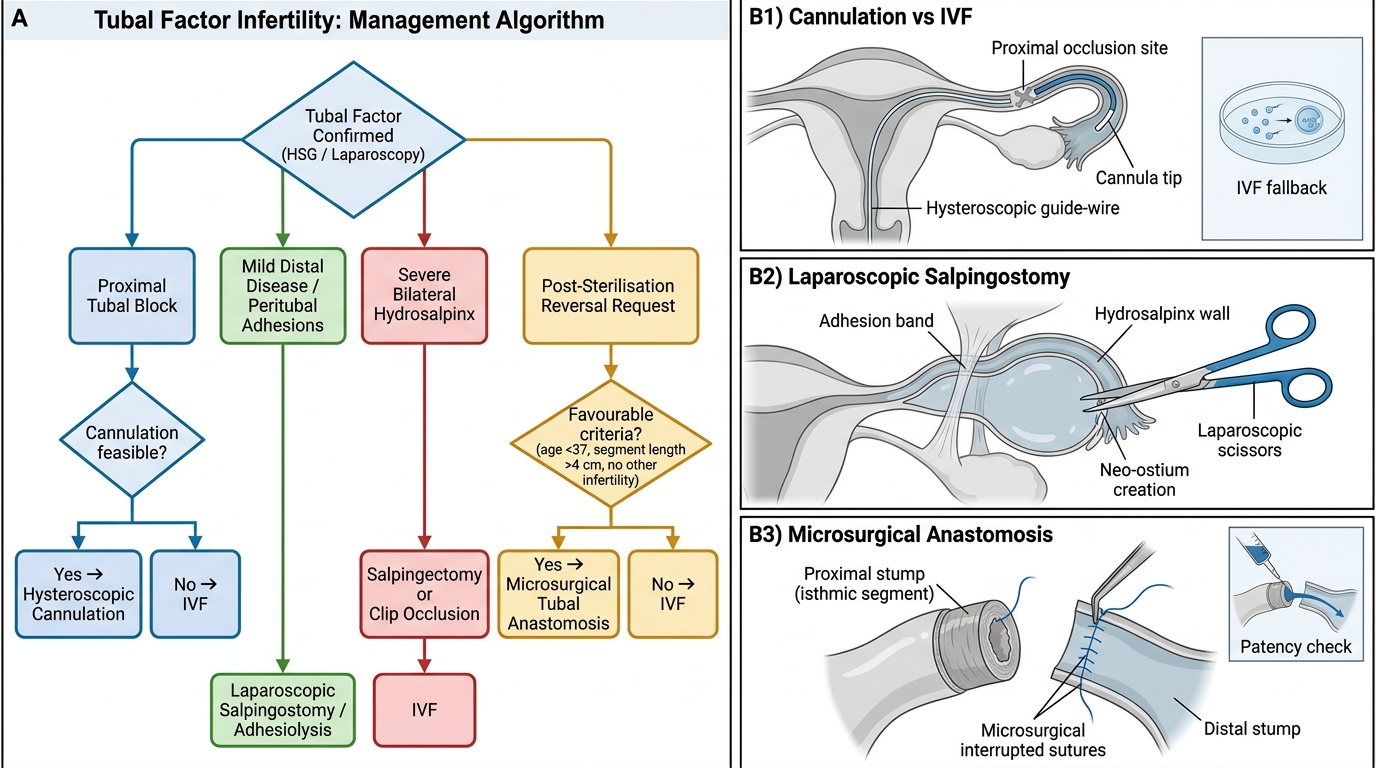
Tubal Factor Infertility: Clinical Decision Algorithm and Surgical Options
Self-Assessment and Practical Takeaways
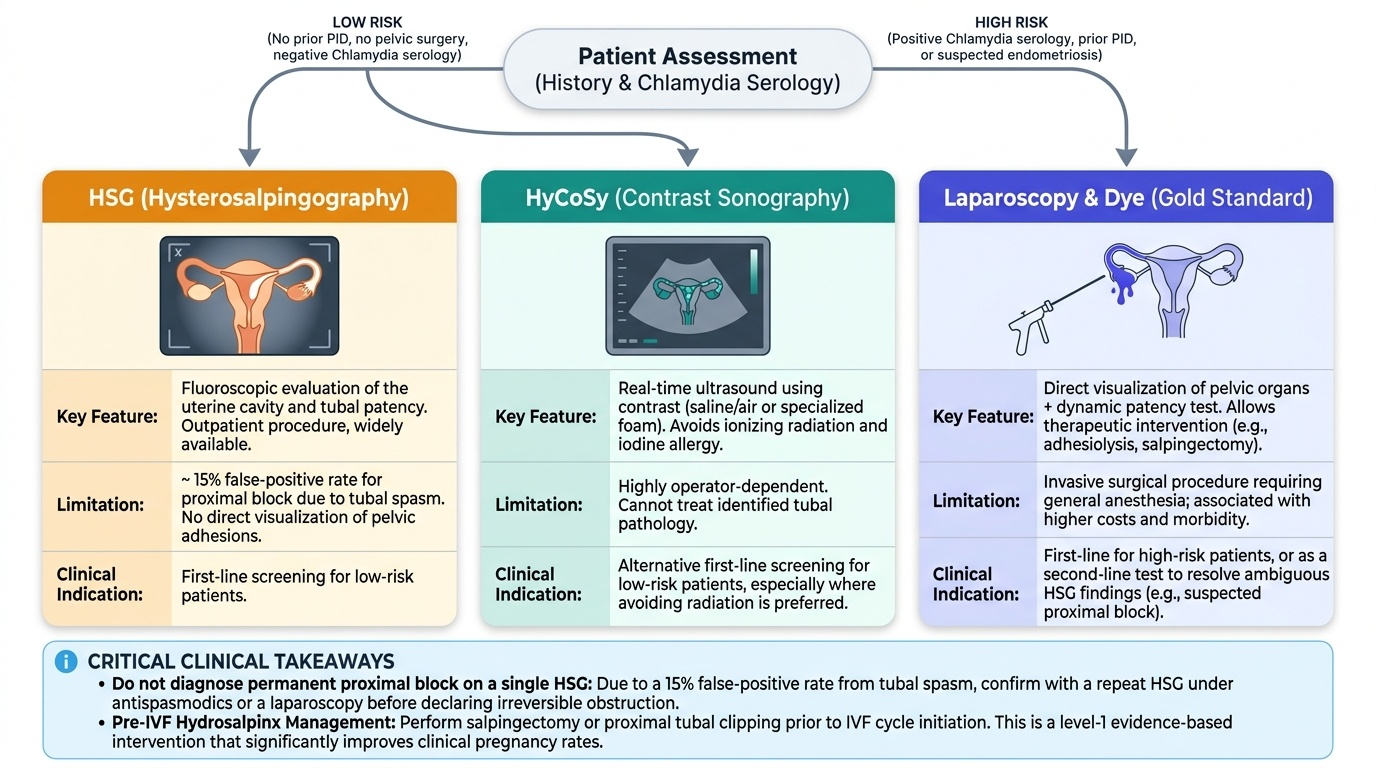
This SDL has taken you from the clinical indication for tubal assessment through the techniques of each modality, interpretation of findings, and the surgical options for restoration. A few consolidating points to cement your understanding before you test yourself. Tubal disease is diagnosed only by direct testing — no symptom reliably predicts it, and its absence from the history is not reassurance. The choice of test must match the clinical context: low-risk women with no prior PID or pelvic surgery can be offered HSG as an outpatient first step; women with positive chlamydia serology or a history of PID should go directly to laparoscopy, because the additional diagnostic yield of direct visualisation outweighs the extra morbidity of a general anaesthetic. Always remember that a proximal block on HSG should be interpreted with caution given the 15% false-positive rate from spasm; a second opinion via laparoscopy or repeat HSG under antispasmodic cover is appropriate before concluding that a tube is irreversibly obstructed. And the management of hydrosalpinx before IVF — salpingectomy or clipping — is one of the highest-yield interventions in reproductive medicine, with level-1 evidence supporting it.
Provided image
Test your recall:
- Gold standard for tubal patency: laparoscopy + chromopertubation (methylene blue)
- HSG false-positive proximal block rate: ~15%
- Indication for laparoscopy as first-line (over HSG): positive chlamydia antibody titre, prior PID, suspected endometriosis
- Treatment of hydrosalpinx before IVF: salpingectomy or proximal clipping
- Best candidates for tubal anastomosis: age <35, remaining tube ≥4 cm, clips/rings sterilisation
- Post-salpingostomy ectopic pregnancy risk: ~15–20% (higher than in general population)
SELF-CHECK
A 35-year-old woman is found to have bilateral hydrosalpinges on laparoscopy performed for infertility. She and her husband are planning IVF. What is the most appropriate management of the hydrosalpinges?
A. Proceed directly to IVF — the hydrosalpinges will not affect IVF success
B. Perform bilateral salpingostomy to restore natural fertility before considering IVF
C. Perform bilateral salpingectomy or proximal tubal ligation/clipping before IVF
D. Prescribe antibiotics and repeat laparoscopy in 3 months
Reveal Answer
Answer: C. Perform bilateral salpingectomy or proximal tubal ligation/clipping before IVF
Bilateral hydrosalpinges must be treated before IVF — the hydrosalpinx fluid is embryotoxic (contains cytokines and prostaglandins) and its reflux into the endometrial cavity reduces implantation rates by approximately 50%. Multiple RCTs show that salpingectomy or proximal occlusion before IVF significantly improves live birth rates. Salpingostomy is not appropriate here as it would not eliminate the embryotoxic fluid reliably, and at age 35 with bilateral severe disease, IVF is the preferred path over natural conception attempts.
CLINICAL PEARL
A proximal block on HSG is not a diagnosis until confirmed — it may be a spasm. The isthmic portion of the tube is rich in smooth muscle and can contract reflexively in response to the discomfort and contrast media pressure of an HSG, producing the appearance of a cornual block. Before counselling a woman that she has a blocked tube and referring for IVF, always verify with laparoscopy or a repeat HSG under antispasmodic cover. Conversely, a bilateral hydrosalpinx on HSG or laparoscopy carries an immediate management implication — it must be treated before IVF proceeds, not after failed cycles.