Page 10 of 24
OG32.1 | Menopause — SDL Guide (Part 2)
Clinical Features and Symptoms of Menopause
The symptoms of menopause are conveniently classified by the time of their onset after the final menstrual period, reflecting the tissues most sensitive to early versus sustained oestrogen deprivation.
Short-term symptoms (first 2 years): Vasomotor symptoms — hot flushes (sudden onset of intense warmth over the face, neck, and chest, lasting 1–5 minutes, often followed by sweating and chills; frequency 6–10 per day in moderate-severe cases) and night sweats (nocturnal hot flushes disrupting sleep). Sleep disturbance, fatigue, mood changes (irritability, low mood, anxiety), poor concentration, and reduced libido. Irregular menstrual cycles during the perimenopause — initially shortened cycles, later prolonged amenorrhoeic intervals.
Medium-term symptoms (2–5 years): Genitourinary syndrome of menopause (GSM): vaginal dryness, dyspareunia, vulval pruritus, atrophic vaginitis; urinary frequency, urgency, recurrent UTIs, stress incontinence. These symptoms do not resolve spontaneously and worsen with time if untreated.
Long-term consequences (>5 years): Osteoporosis and fragility fractures (vertebral, hip, Colles'); cardiovascular disease (ischaemic heart disease, stroke — the leading cause of death in postmenopausal women); skin changes (thinning, reduced collagen); joint pains (arthralgias). Women with premature ovarian insufficiency (POI) face all these consequences decades earlier.
On examination, typical findings include: atrophic vaginal mucosa (pale, dry, with loss of rugae), reduced vaginal calibre, a friable epithelium that bleeds easily on contact, and labial shrinkage. The uterus is often small and the ovaries impalpable on ultrasound.
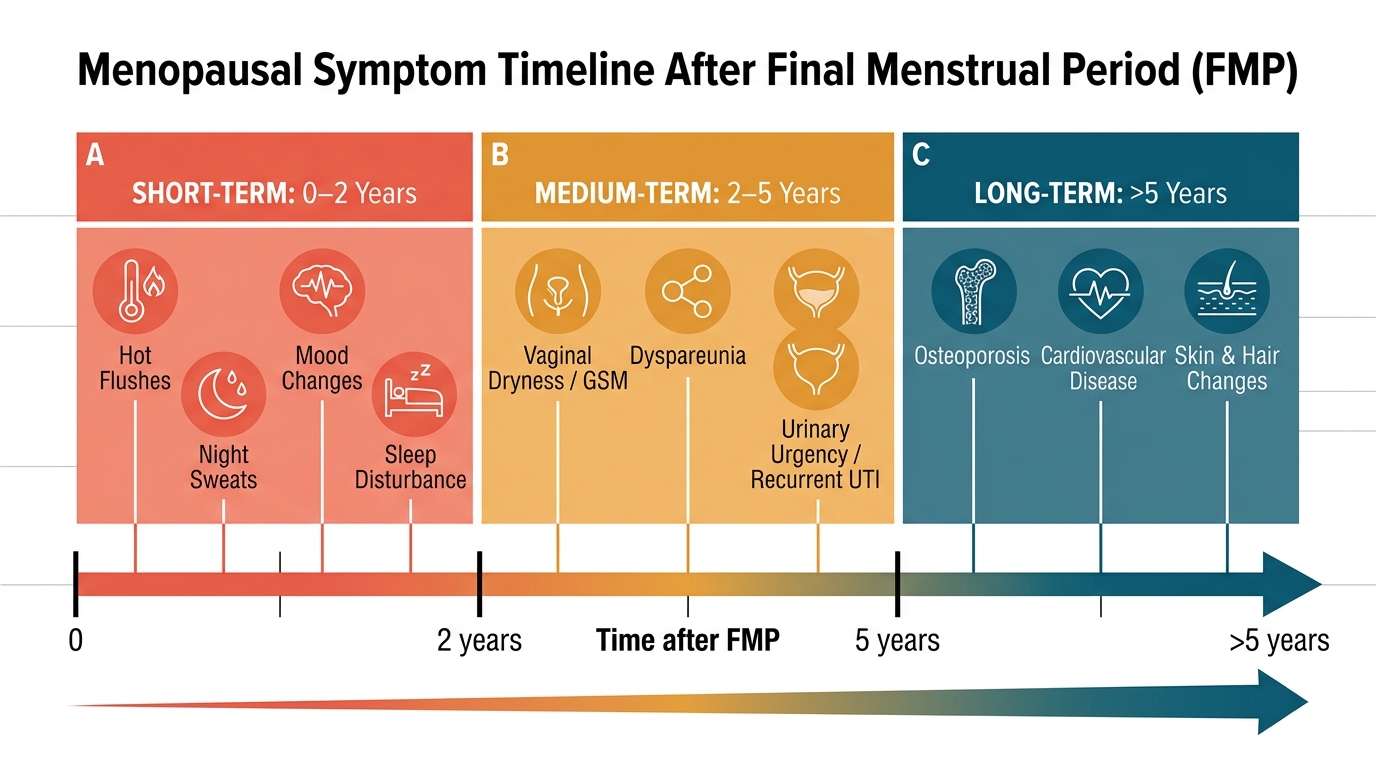
Menopausal Symptom Timeline by Phase After Final Menstrual Period
Investigation and Diagnosis
In most women aged 45–55 years with typical symptoms and irregular periods, menopause is a clinical diagnosis — investigations are NOT routinely required to confirm natural menopause. The diagnosis of the final menstrual period can only be made retrospectively after 12 consecutive months of amenorrhoea.
Investigations are indicated in the following specific situations: (1) Women under 45 years with suspected premature ovarian insufficiency or premature menopause — to confirm the diagnosis and exclude reversible causes. (2) Women on combined oral contraceptives or with a Mirena IUS in whom menstrual suppression makes clinical diagnosis unreliable. (3) Women with atypical presentations where other diagnoses (thyroid disease, hyperprolactinaemia, pregnancy) need exclusion.
Serum FSH: A level >30–40 IU/L on two occasions at least 4–6 weeks apart, in the appropriate clinical context, confirms menopause or POI. In the perimenopause, FSH fluctuates widely (can be normal on one test and elevated on another); a single measurement is unreliable. Serum oestradiol <100–200 pmol/L in symptomatic women supports menopause. Thyroid function tests (to exclude hypothyroidism mimicking fatigue, menstrual irregularity, and mood changes). Prolactin (to exclude hyperprolactinaemia causing amenorrhoea). Fasting lipids and glucose (cardiovascular risk assessment before starting HRT). DEXA scan (dual-energy X-ray absorptiometry) for bone mineral density measurement — indicated in women with POI, high fracture risk, before starting bisphosphonate therapy, and in women over 65 years: T-score ≤ −2.5 = osteoporosis; −1.0 to −2.5 = osteopenia.
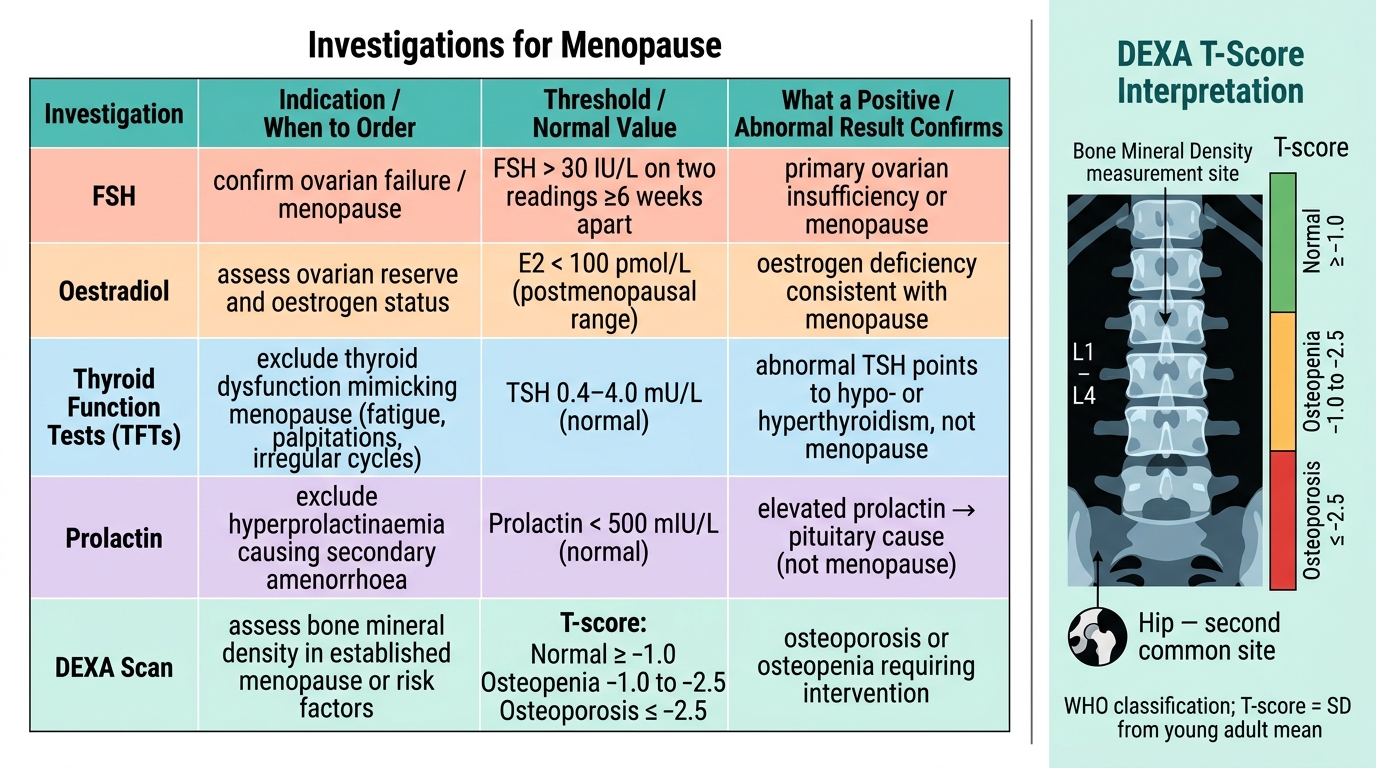
Investigations for Menopause: Indications, Thresholds, and Diagnostic Significance
Hormone Replacement Therapy (HRT) — Principles, Types, and Benefits
Hormone replacement therapy replaces the oestrogen (and where necessary progesterone) that the ovaries have stopped producing, relieving symptoms and preventing long-term complications. HRT is the most effective treatment for menopausal symptoms and is the first-line recommendation for women with moderate-to-severe vasomotor symptoms who have no contraindications.
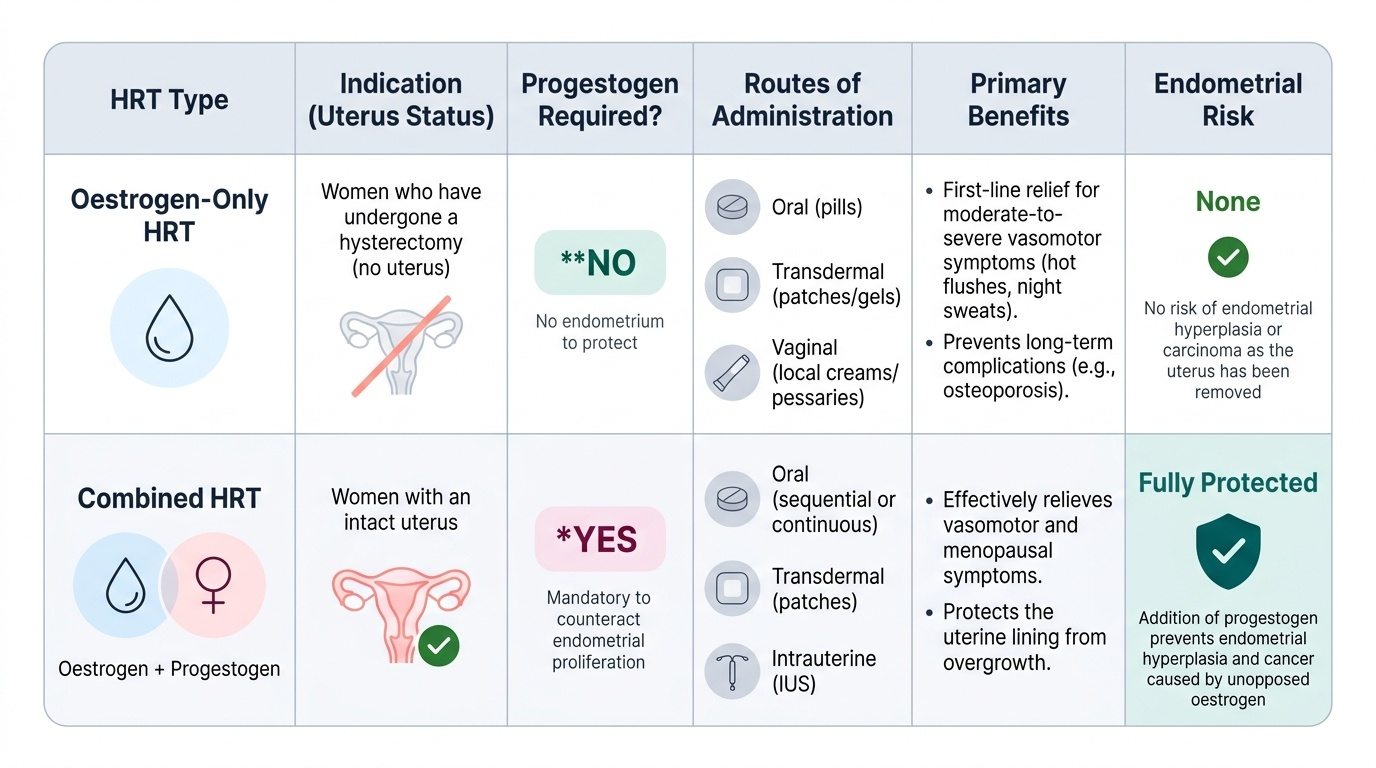
The fundamental principle governing HRT type is uterine status: women who have an intact uterus MUST receive combined HRT (oestrogen + progestogen), because unopposed oestrogen stimulates endometrial proliferation and causes endometrial hyperplasia and carcinoma. Women who have had a hysterectomy can safely receive oestrogen-only HRT without a progestogen, as there is no endometrium to protect.
Types of progestogen in combined HRT: Synthetic progestogens (medroxyprogesterone acetate — MPA, norethisterone) are associated with slightly higher breast cancer risk than natural progesterone. Micronised progesterone (Utrogestan) and dydrogesterone are closer to natural progesterone and carry a more favourable breast cancer risk profile; they are preferred in current practice. Combined HRT can be given in sequential mode (oestrogen daily + progestogen for 12–14 days per month, producing a regular withdrawal bleed — used in perimenopausal women who have not had 12 months' amenorrhoea) or continuous combined mode (both hormones daily — suitable for postmenopausal women, avoids withdrawal bleeds).
Routes of administration: Oral (convenient), transdermal (patches, gels, spray — avoids first-pass hepatic metabolism, lower VTE risk than oral, preferred in women with cardiovascular risk or migraine), and local/vaginal (topical oestrogen creams, pessaries, ring — for GSM, low systemic absorption, can be used indefinitely, safe even in most breast cancer survivors). Vaginal testosterone (low-dose) is an emerging option for hypoactive sexual desire.
Benefits of HRT: Relief of vasomotor symptoms (60–90% reduction in hot flush frequency), improvement of GSM, mood and sleep, prevention of osteoporosis (maintains BMD and reduces fracture risk), and — when started early (within 10 years of menopause or before age 60) — possible cardiovascular benefit (the 'timing hypothesis'). HRT is the standard of care for POI until age 50.
Provided image