Page 6 of 24
OG31.1 | Uterine Prolapse — SDL Guide (Part 2)
Classification and POP-Q Staging
Prolapse has historically been graded by the traditional clinical system, but internationally the Pelvic Organ Prolapse Quantification (POP-Q) system (Bump et al., 1996, adopted by the International Continence Society) is the standard. POP-Q uses the hymenal ring as a fixed reference point (0), with measurements in centimetres above (negative values, inside) or below (positive values, outside) the hymen at maximum Valsalva. Nine specific anatomical points are measured.
The POP-Q stages are: Stage 0 — no prolapse; Stage I — most distal portion is more than 1 cm above the hymen (< −1 cm); Stage II — most distal portion is between −1 cm and +1 cm of the hymen (within 1 cm either side); Stage III — most distal portion is more than 1 cm beyond the hymen but less than or equal to total vaginal length minus 2 cm; Stage IV — complete eversion (most distal portion ≥ total vaginal length minus 2 cm). Stage II is clinically the threshold for symptomatic, visually apparent prolapse.
The traditional system, still widely used clinically, grades uterine descent as: 1st degree — cervix descends into the vagina but does not reach the introitus; 2nd degree — cervix reaches the introitus; 3rd degree (procidentia) — cervix comes outside the introitus. The associated vaginal wall descent is described separately as cystocele (anterior wall), rectocele (posterior wall), and enterocele (small bowel entering the rectovaginal pouch, bulging the upper posterior wall).
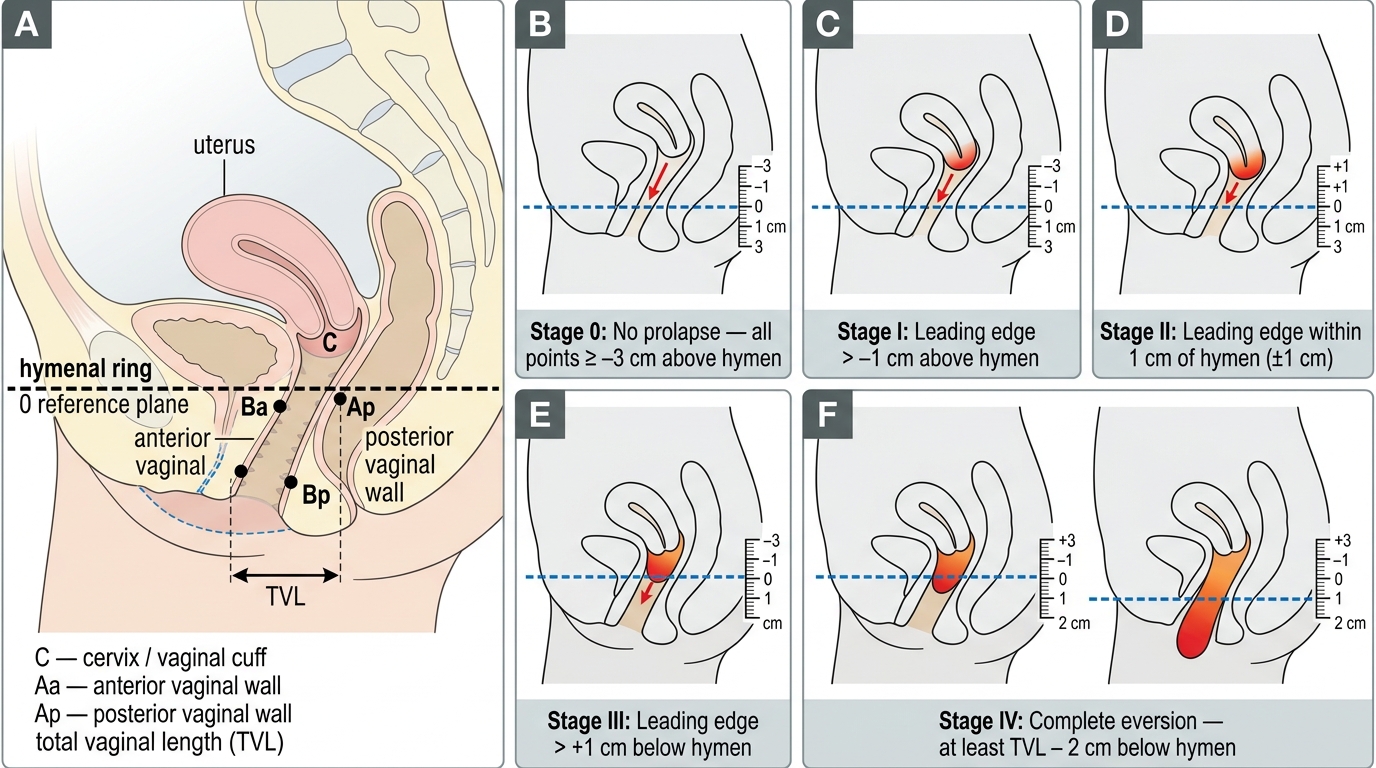
POP-Q Staging System for Uterine Prolapse (Stages 0–IV)
Diagnosis and Investigations
Diagnosis is primarily clinical. The patient should be examined in the dorsal lithotomy position initially, and then in the left lateral (Sims') position using a Sims' speculum — this allows the anterior and posterior walls to be assessed separately while the patient strains. The clinician retracts the posterior wall and observes the anterior wall for cystocele, then retracts the anterior wall to look for rectocele, and finally removes the speculum blade to observe uterine descent on Valsalva. The patient should ideally be examined with a full bladder to demonstrate stress incontinence.
Investigations: A mid-stream urine culture is routine (urinary tract infection is common with prolapse). Urodynamic studies — cystometry (bladder capacity, filling pressures, detrusor overactivity) and uroflowmetry — are indicated before any surgical repair to detect occult stress incontinence and detrusor instability that may be unmasked after repair. Renal ultrasound and serum creatinine are indicated if there is evidence of ureteric obstruction (hydronephrosis from chronic urinary retention in advanced prolapse). Pap smear should be taken, particularly if there is cervical ulceration or discharge. MRI pelvis provides anatomical mapping of pelvic floor defects and is useful in recurrent or complex prolapse before reoperation. Haemoglobin and general anaesthetic fitness investigations are required before elective surgery.
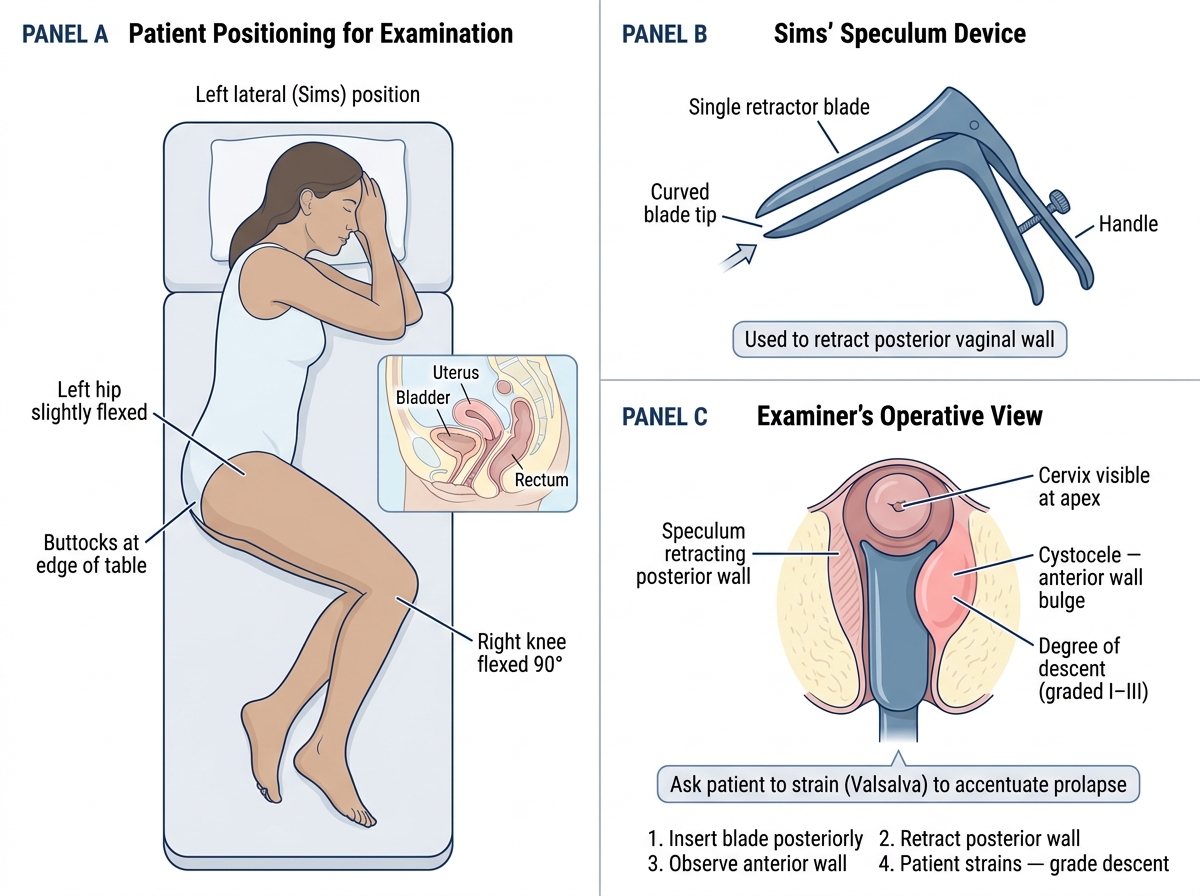
Sims' Speculum Examination for Prolapse Assessment
Management — Conservative and Pessary
Conservative management is appropriate for women who are not surgical candidates (elderly, medically unfit, or those who decline surgery), for mild-to-moderate prolapse (POP-Q Stage I–II), and as a temporising measure while awaiting surgery. General measures include weight reduction, treatment of chronic cough, management of constipation, and avoidance of heavy lifting. Topical oestrogen cream (in postmenopausal women) improves vaginal epithelial atrophy, reduces irritation, and strengthens connective tissues around a pessary or before surgery.
Pelvic floor muscle training (PFMT, Kegel exercises) is the first-line conservative treatment — systematic contractions of the levator ani (holding for 3–5 seconds, releasing, 10 repetitions, 3 sets daily, for at least 12 weeks) can reduce prolapse symptoms and stage in mild cases. Physiotherapy-supervised PFMT shows better outcomes than unsupervised.
Ring pessary is the most widely used mechanical device for uterine prolapse. It is a flexible silicone or PVC ring inserted into the vagina to sit at the level of the pelvic brim, mechanically supporting the prolapse. It is effective for Stage II–III prolapse and for women who decline or are unfit for surgery. Indications include: desire to avoid surgery, unfit for anaesthesia, desire for future pregnancy, prolapse in pregnancy. Contraindications include: active vaginal infection, non-compliant patient (cannot attend for follow-up), and severe pelvic floor atrophy where the pessary cannot be retained. The pessary should be changed every 3–6 months; complications include vaginal discharge, ulceration, and rare impaction. Other pessary types include shelf (Hodge), ring with support, and Gellhorn pessaries for more advanced prolapse.
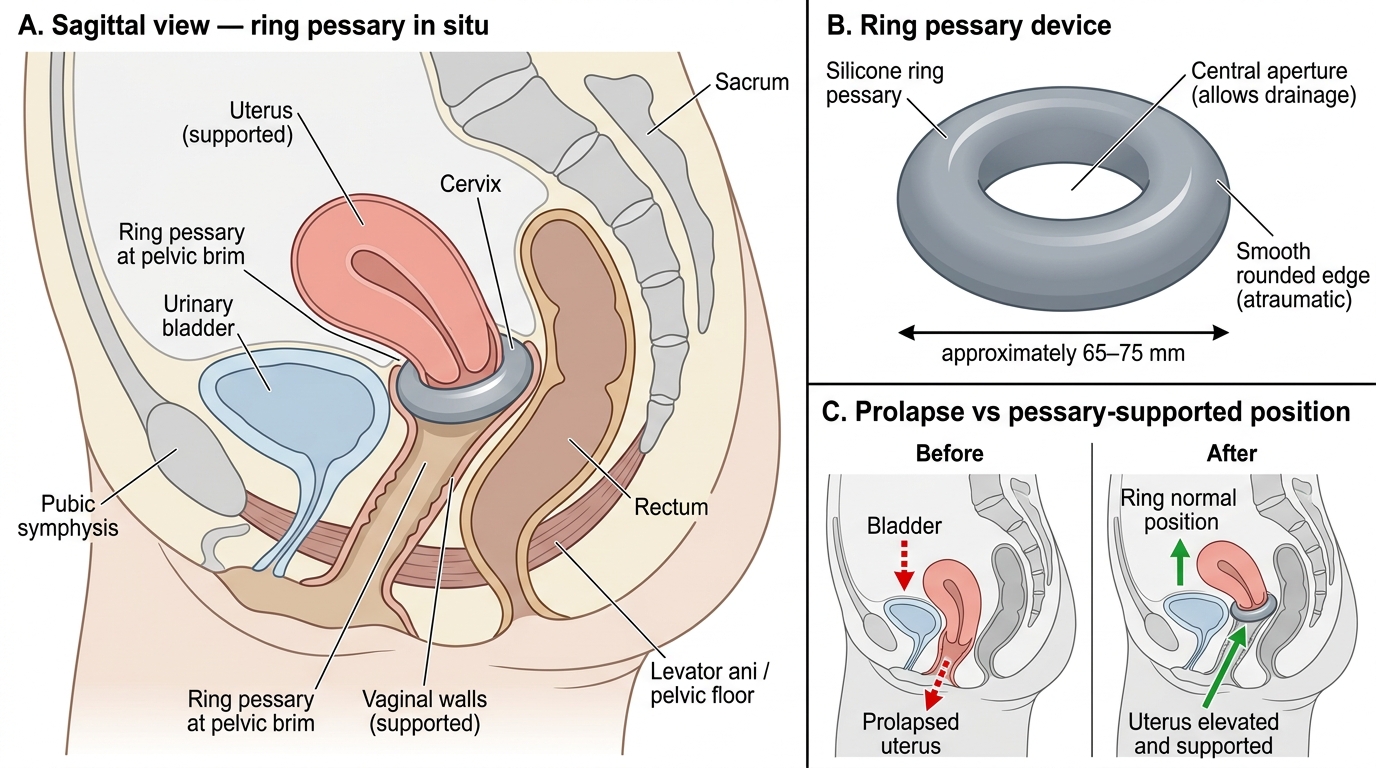
Ring Pessary Placement for Uterine Prolapse