Page 5 of 29
OG35.12-13,OG38.4 | Discharge, Referral and Medical Certification — SDL Guide
Learning Objectives
- Write a structured and complete discharge summary for an obstetric or gynaecological patient, incorporating all mandatory components
- Compose a clinically adequate referral letter to secondary or tertiary care, grading urgency appropriately and attaching required documents
- Assess the need for and issue correct medical certificates for maternity, sickness, fitness, or medicolegal purposes in OG practice
- Identify errors or omissions in a received discharge summary or referral letter and take appropriate corrective action
INSTRUCTIONS
Clinical documentation is the permanent record of a patient's care and a professional obligation under the NMC code of conduct. A poorly written discharge summary, an incomplete referral letter, or an incorrectly issued medical certificate can delay care, expose the patient to harm, and create serious medicolegal liability for the clinician. This module guides you through the structure, legal requirements, and supervised practice of the three core documentation tasks in obstetrics and gynaecology.
References
- Dutta DC. Textbook of Obstetrics. 10th ed. New Central Book Agency; 2023 (textbook)
- Shaw RW, Luesley D, Monga A. Shaw's Textbook of Gynaecology. 17th ed. Elsevier; 2019 (textbook)
- NMC Competency-Based Undergraduate Curriculum for MBBS, 2024 — Obstetrics and Gynaecology competencies OG35, OG38 (guideline)
- Medical Termination of Pregnancy (Amendment) Act 2021 and MTP Rules 2021 (legislation)
- Maternity Benefit Act 1961 (amended 2017) (legislation)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Dr Shalini has just completed a caesarean section for Mrs Anitha, a 28-year-old primigravida who presented with severe pre-eclampsia at 36 weeks. Two days later, Mrs Anitha is ready for discharge and will continue her anti-hypertensive medications under the supervision of her local PHC doctor. Dr Shalini hurriedly writes a brief discharge note: 'LSCS done. BP settling. Continue labetalol.' Six weeks later, Mrs Anitha is readmitted with hypertensive crisis — the PHC doctor had no record of the drug dose, had not been told about the expected timeline for tapering, and had missed the follow-up BP target. A complete discharge summary would have prevented this. In obstetrics and gynaecology, what you write follows the patient beyond the hospital door.
WHY THIS MATTERS
Every final-year MBBS student and intern is required to write discharge summaries, referral letters, and medical certificates as part of daily hospital work. These documents carry legal weight — they are admissible in court, relied upon by insurance companies, and used as the primary source of care information when a patient transitions between providers. Errors in documentation — an omitted medication dose, an unstated gestational age, an incorrectly issued maternity certificate — constitute negligence. Mastering these three document types during your clinical training is not optional: OG35.12, OG35.13, and OG38.4 are core NMC competencies assessed in your final clinical examinations.
RECALL
Before proceeding, retrieve what you already know. In your medicine and surgery postings you will have encountered discharge summaries — what were the standard headers? Recall the anatomy of an OG case record: what does the clerking template cover (presenting complaint, obstetric history, menstrual history, examination findings, investigation results, diagnosis, treatment plan)? Think about the Indian legal framework you touched on in community medicine: what Acts govern maternity leave, medical certification, and abortion documentation? Hold those frames in mind as we build on them with OG-specific requirements.
Why Documentation Defines Quality of Care
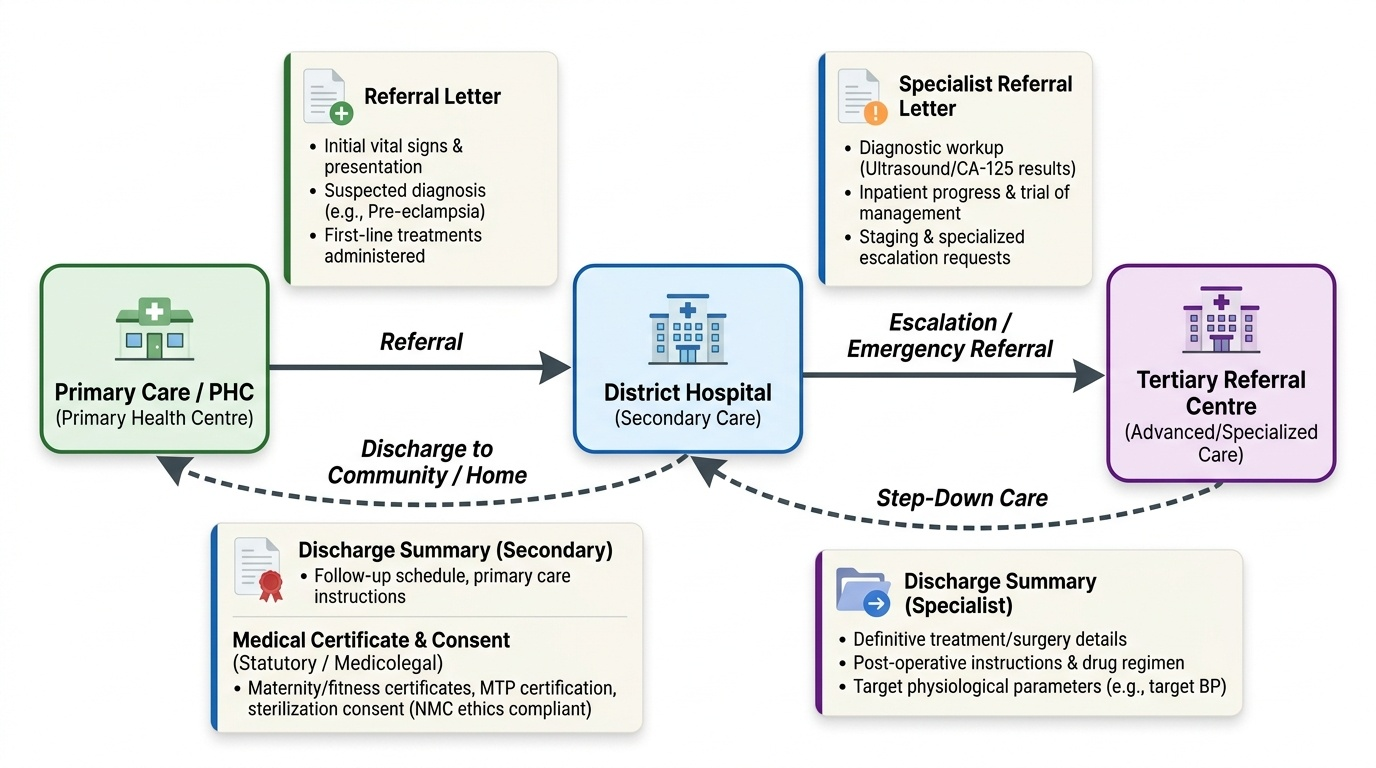
Clinical documentation is the single thread that connects a patient's care across providers, settings, and time. In obstetrics and gynaecology, where care transitions are common — from primary health centre to district hospital, from labour ward to postnatal ward, from tertiary referral back to the community — the quality of written communication directly determines whether the next clinician can continue safe care or must start again from scratch. Poor documentation is implicated in a significant proportion of adverse maternal outcomes in India. A patient discharged after treatment for severe pre-eclampsia without a clear record of her drug regimen and target blood pressure is at measurable risk of re-admission with uncontrolled hypertension. A woman referred for suspected ovarian malignancy without her ultrasound and CA-125 results faces unnecessary delay in definitive staging.
Documentation also carries a medicolegal dimension that is unique in medicine. The medical record is a legal document: it is the clinician's contemporaneous account of what was done and why. In litigation, the maxim 'if it isn't written, it wasn't done' is applied literally. OG practice generates a particularly high volume of documentation with legal implications — consent for sterilisation, certification for MTP, maternity and fitness certificates — and the standards for these documents are defined by statute, not merely convention.
Finally, documentation is a professional obligation under the NMC code of ethics and is assessed in OSCE, viva voce, and clinical examinations. Competency in documentation is therefore simultaneously a patient-safety imperative, a legal obligation, and an examination requirement.
Provided image
Principles of Clinical Documentation in Obstetrics and Gynaecology
Six governing principles apply to all clinical documentation in obstetrics and gynaecology, and mastering them before learning the specific formats prevents the errors that compromise patient care and medicolegal standing.
The first principle is accuracy: every fact in a clinical document must be verifiable from the case record. Do not write a diagnosis you cannot substantiate, a drug dose you have not confirmed, or a gestational age you have not calculated from a reliable dating scan or last menstrual period. In OG, gestational age is a cornerstone of every clinical decision — an error of even two weeks can change the legality of an MTP, alter the management of preterm labour, or invalidate a maternity certificate.
The second principle is completeness: a document that omits critical information is functionally worse than no document. The receiving clinician will either make assumptions (dangerous) or call for clarification (delays care). The most frequently omitted items in discharge summaries are medication doses and durations, follow-up targets, and red-flag symptoms warranting immediate return.
The third principle is timeliness: a discharge summary should be completed before or at the time the patient leaves the ward, not days later. A referral letter must be written before the patient leaves for the referral centre, so that it accompanies rather than follows the patient. Medical certificates must be issued on the date of examination.
The fourth principle is legibility and clarity: handwritten documents should be legible to someone who has never met the patient. Use standard abbreviations; define unfamiliar ones. Avoid jargon that the receiving provider (who may be a PHC medical officer or a patient herself) will not understand.
The fifth principle is confidentiality: clinical documents are private to the patient. They must be sealed or transmitted through secure channels. In medicolegal cases, disclosure rules differ (police, courts, and insurance companies have specific access rights). Never include information that is not clinically necessary.
The sixth principle is the medicolegal framework: all three document types are governed by a combination of common law principles, the Indian Medical Council / NMC code of ethics, and specific statutes. Medical certificates in particular have statutory requirements: the issuing doctor must have examined the patient, must be registered, and must issue on the prescribed form where one exists.
| Principle | Core Requirement | OG-Specific Consequence of Failure |
|---|---|---|
| Accuracy | All facts verifiable | Incorrect gestational age → invalid MTP certificate or wrong management |
| Completeness | No critical omission | Missing drug dose → uncontrolled postpartum hypertension |
| Timeliness | Written before discharge/referral | Late summary → PHC acts without information |
| Legibility | Readable by any provider | Illegible dose → dispensing error |
| Confidentiality | Secure transmission | Breach of patient privacy → NMC disciplinary action |
| Medicolegal framework | Statutory requirements met | Wrong form, unauthorised issuer → certificate legally invalid |
SELF-CHECK
A patient is being discharged after treatment for a ruptured ectopic pregnancy. The doctor completes the discharge summary two days after the patient has already left the ward, and hands it to the family to post to the PHC. Which principle of clinical documentation has been violated?
A. Accuracy only
B. Completeness only
C. Timeliness and confidentiality
D. Medicolegal framework only
Reveal Answer
Answer: C. Timeliness and confidentiality
Completing the summary after discharge violates timeliness (it should be written at or before discharge). Handing an unsealed summary to the family to post violates confidentiality (clinical documents must be transmitted through secure channels). Both principles are violated here.
Writing a Discharge Summary: Structure and Content
A discharge summary is a structured clinical communication document completed when a patient leaves an inpatient facility, providing the receiving provider (PHC doctor, specialist, or patient) with a complete and actionable account of the hospitalisation. In obstetrics and gynaecology, this is one of the most frequently written documents in daily practice, and its quality directly determines continuity of care for mothers, newborns, and gynaecology patients.
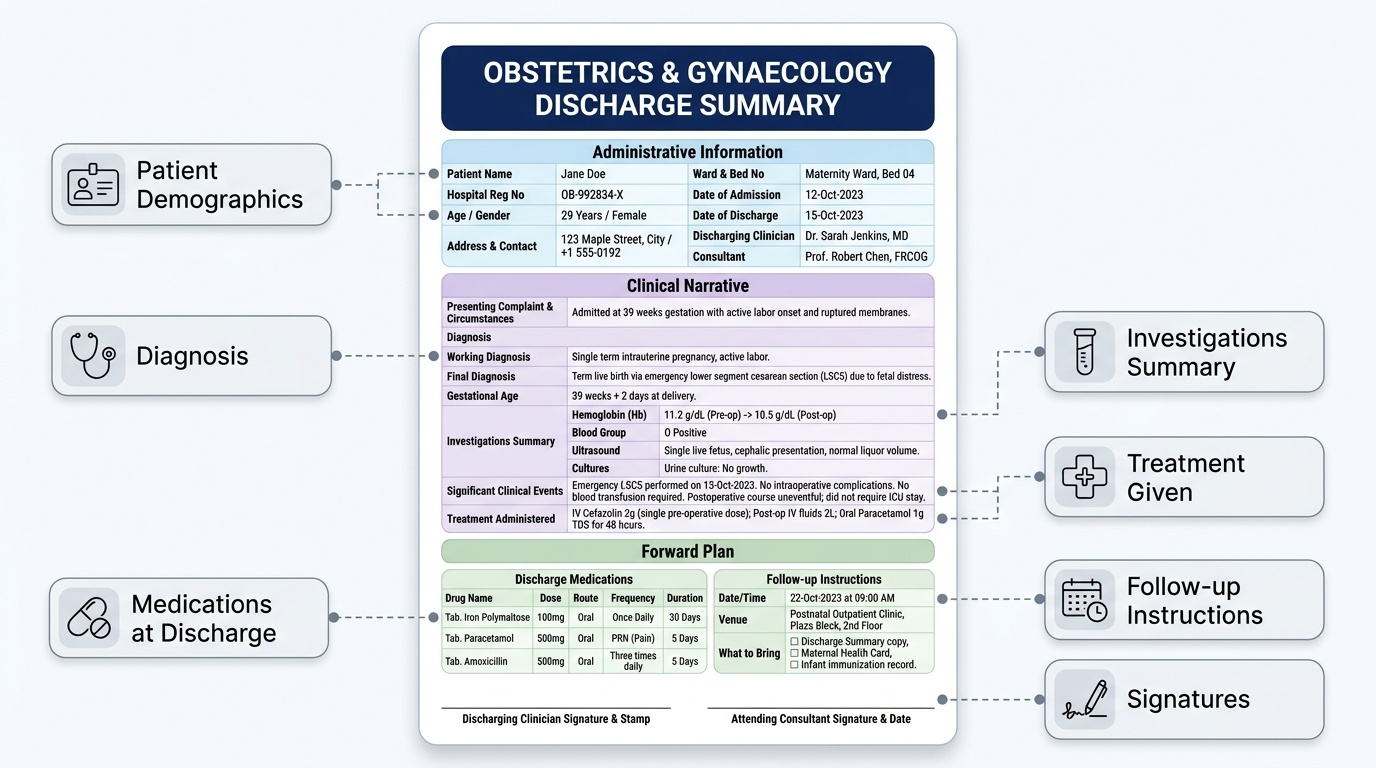
The mandatory components of an OG discharge summary are organised into three zones: administrative information, clinical narrative, and forward plan.
Administrative information includes the patient's full name, hospital registration number, age, address and contact number, ward and bed number, date of admission, date of discharge, and the name and designation of the discharging clinician and consultant. Missing any of these makes the document impossible to link to the correct patient in a future encounter.
Clinical narrative covers: (a) the presenting complaint and circumstances of admission; (b) the working and final diagnosis, including gestational age at admission and at delivery where applicable; (c) a summary of relevant investigations with results (haemoglobin, blood group, ultrasound findings, cultures where relevant); (d) significant clinical events during admission (surgical procedures, complications, blood transfusion, ICU stay); (e) treatment administered, including all medications with dose, route, and duration.
Forward plan covers: (a) medications at discharge — list every drug with dose, route, frequency, and duration; (b) specific follow-up instructions — date, venue, and what to bring; (c) measurable targets where relevant (e.g. 'blood pressure target <140/90; re-attend if systolic >160'); (d) red-flag symptoms requiring immediate return ('return if heavy vaginal bleeding, severe headache, blurred vision, or convulsion'); (e) restrictions or instructions (pelvic rest duration, wound care, breastfeeding support contacts); (f) for postnatal cases, neonatal details including weight, Apgar scores, immunisations given, and newborn screening results.
A common error is to write 'continue medications' without listing them. In a ward with high turnover, this is a handover failure. Every drug must be named, dosed, and timed.
Provided image
SELF-CHECK
A postnatal patient is being discharged on day 2 after an uncomplicated vaginal delivery. Her discharge summary lists 'Tab. Iron — continue for 3 months' and 'return to PHC in 6 weeks'. What critical information is missing?
A. The patient's blood group
B. The iron tablet dose and the specific follow-up date
C. The Apgar score of the newborn
D. The baby's feeding method
Reveal Answer
Answer: B. The iron tablet dose and the specific follow-up date
The forward plan requires every medication to be listed with dose, route, frequency, and duration. 'Tab. Iron — continue' is incomplete without the dose (e.g. ferrous sulphate 200 mg twice daily). 'Return in 6 weeks' should be a specific date or at minimum a calculated date range. The Apgar score and neonatal details are also important but the option that describes the most dangerous omission — medication incompleteness — is the iron dose.