Page 13 of 29
OG35.4-6 | Focused Gynaecological Case Approach — SDL Guide
Learning Objectives
- Demonstrate a structured clinical approach to a patient presenting with a suprapubic or pelvic mass, including history, physical examination, differential diagnosis, investigation, and initial management
- Demonstrate a structured clinical approach to a patient presenting with vaginal discharge, distinguishing physiological from pathological causes and applying appropriate investigations
- Demonstrate a structured clinical approach to a patient presenting with genital ulcers, characterising the ulcer, constructing a differential diagnosis for STI-related and non-STI causes, and selecting appropriate investigations and syndromic or aetiological management
INSTRUCTIONS
Gynaecology is a specialty where the clinical presentation — a pelvic lump, an abnormal discharge, a genital ulcer — narrows the differential diagnosis significantly but does not establish it. The difference between a fibroid uterus and an ovarian malignancy, between bacterial vaginosis and early cervical carcinoma, between a syphilitic chancre and a herpetic ulcer, is made by a structured history, a systematic examination, and targeted investigations interpreted in context. This module builds that structured approach across three of the most common gynaecological presentations you will encounter in clinical practice.
References
- Dutta DC. Textbook of Obstetrics. 10th ed. New Central Book Agency; 2023 (textbook)
- Shaw RW et al. Shaw's Textbook of Gynaecology. 17th ed. Elsevier; 2019 (textbook)
- Jeffcoate N. Principles of Gynaecology. 8th ed. Hodder Arnold; 2008 (textbook)
- WHO. Guidelines for the Management of Symptomatic Sexually Transmitted Infections. 2021 (guideline)
- FOGSI. Clinical Practice Guidelines — Gynaecological Infections and Pelvic Mass. 2022 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Mrs Geeta, 38 years old, presents to the OPD with a 'lump in the lower abdomen' that has been growing slowly for a year. She also has heavy periods but has delayed seeking care because she was 'not sure if it was serious.' On inspection the lump is midline, firm, and non-tender. On bimanual examination it is uterine in origin, irregular, and the size of a 14-week gravid uterus. She asks: 'Is it cancer?' The answer depends on a systematic history (duration, menstrual impact, pain, urinary symptoms, family history), a structured examination (abdominal, bimanual, speculum), and focused investigations (ultrasound, FBC, CA-125 in the right context). Without that structure, the examination is a ritual; with it, the examination is the differential diagnosis. A second patient on the same afternoon presents with genital ulcers. Without a framework — pain, edge, base, lymphadenopathy, sexual history, systemic symptoms — the correct pathogen and the correct treatment are both a guess.
WHY THIS MATTERS
The three gynaecological presentations in this module — suprapubic lump, vaginal discharge, and genital ulcers — collectively account for a large proportion of all new gynaecology OPD attendances in India. Competency in structured case approach (OG35.4, OG35.5, OG35.6) is assessed in every format: OSCE (structured clinical examination), long case, short case, and viva voce. More importantly, structured case-taking is the skill that will protect your patients from diagnostic delay in any clinical setting you work in — whether a government hospital OPD, a private clinic, or a resource-limited rural setting where investigations may not be immediately available.
RECALL
Before proceeding, activate what you already know. From your anatomy posting: what organs occupy the pelvis? What is the anatomical relationship of the uterus, fallopian tubes, ovaries, bladder, and rectum? From your microbiology posting: what are the common sexually transmitted pathogens, and what are the key microscopy and culture techniques for each? From your community medicine posting: what is the VDRL test and what does a positive result mean? And from your surgery posting: how do you examine an abdominal lump systematically — site, size, shape, surface, consistency, edge, mobility, tenderness, relations? Hold these frameworks — they are the foundation on which the gynaecological case approach is built.
Why a Structured Case Approach Matters in Gynaecology
Gynaecological diagnosis is pattern recognition — but patterns are only visible if the examination is structured to reveal them. A clinician who examines a pelvic mass without a systematic plan may notice its size and position but miss the crucial features that distinguish a benign fibroid from an ovarian malignancy: surface irregularity, mobility from the uterus, bilaterality, associated ascites, or a firm fixed consistency. Similarly, a vaginal discharge assessed without a pH test and a wet-mount microscopy will be treated empirically when a specific diagnosis — and therefore a specific treatment — was entirely achievable at the bedside.
The structured case approach in gynaecology serves three clinical functions. First, it ensures completeness — by following a consistent framework, the clinician is less likely to omit a key element. Second, it generates a reproducible record: a structured history and examination note can be read and acted upon by any clinician who subsequently sees the patient. Third, it forces active hypothesis generation — rather than waiting for investigations to 'tell' the diagnosis, the structured approach builds a differential at each step and then selects investigations that will discriminate between the leading hypotheses.
In resource-limited Indian clinical settings, structured examination is especially important because investigations are not always available or affordable. The ability to construct a confident differential diagnosis from history and examination alone — and to select only the most discriminating investigation — is a practical skill that saves both patient cost and diagnostic delay. A clinician who has mastered the structured approach to a pelvic lump can manage a patient in a PHC or sub-district hospital with minimal investigation; a clinician who has not mastered it will investigate reflexively and still be uncertain.
The Gynaecological Case Approach: History → Examination → Differential → Investigation
Framework: History, Examination, Differential, and Investigation in OG
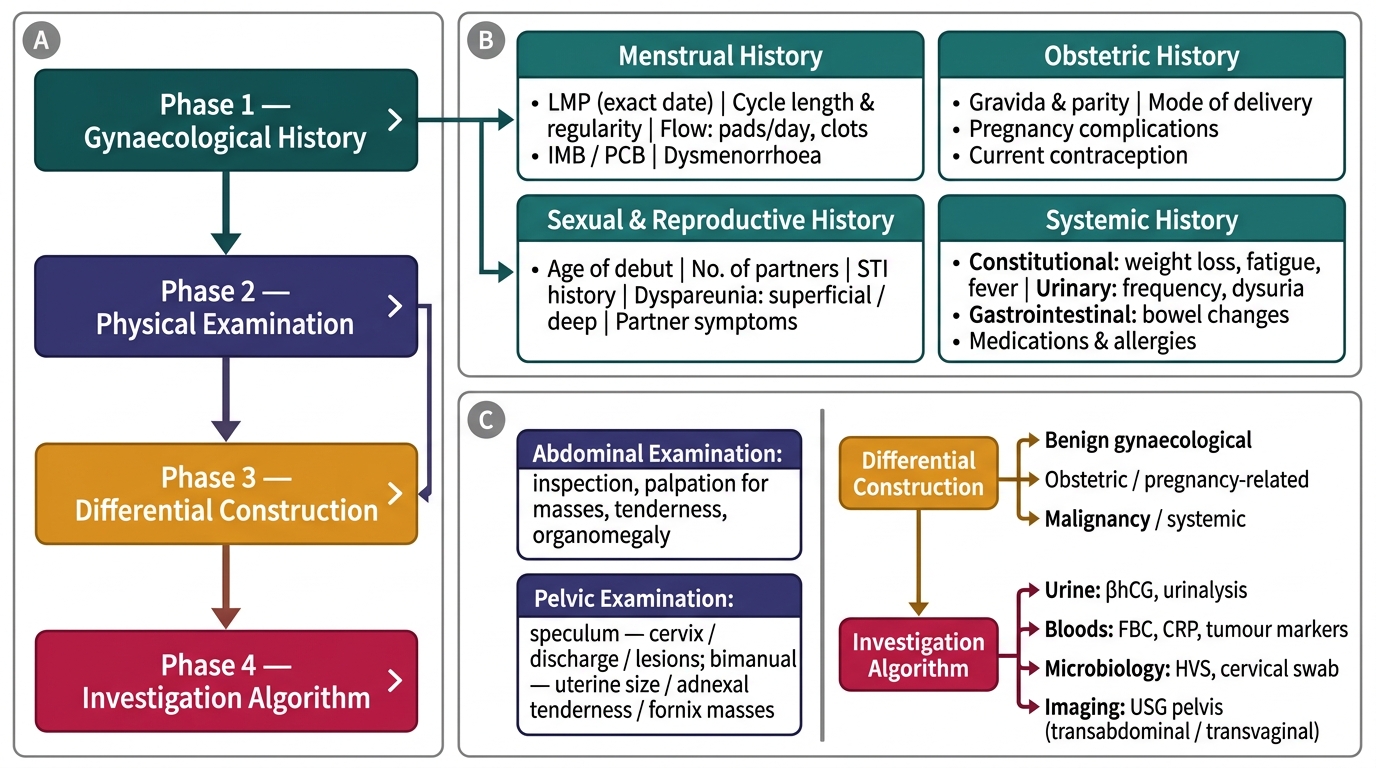
The gynaecological case approach follows a consistent four-phase structure regardless of the presenting complaint. Internalising this structure means that any new gynaecological presentation can be approached systematically from the first encounter.
Phase 1 — Gynaecological history: the OG-specific history has components not present in a general medicine history. The menstrual history must cover: last menstrual period (LMP) with exact date, cycle length and regularity, duration and amount of bleeding (number of pads/tampons per day, presence of clots), intermenstrual or post-coital bleeding, and dysmenorrhoea. The obstetric history covers: gravida and parity, mode of previous deliveries, pregnancy complications, and current contraceptive use. The sexual and reproductive history covers: age of sexual debut, number of partners, history of STI, dyspareunia (superficial or deep), and for the presenting complaint of discharge or ulcers, the full STI contact and symptom history of the partner. The systemic history covers: constitutional symptoms (weight loss, fatigue, fever — red flags for malignancy or infection), urinary symptoms (frequency, dysuria — related to pelvic mass or PID), and bowel symptoms (constipation, altered habit — suggestive of a posterior pelvic mass or colorectal involvement).
Phase 2 — Physical examination: begins with general examination for pallor, lymphadenopathy (inguinal nodes in genital ulcer cases; supraclavicular in ovarian malignancy), and abdominal examination using the surgical LUMP framework (site, size, shape, surface, consistency, edge, mobility, tenderness, relations). Per-speculum examination assesses the vaginal walls (rugosity, discharge character), the cervix (appearance, ectropion, bleeding on touch), and the cervical os. Per-vaginal (bimanual) examination assesses the uterus (size, position, consistency, mobility, tenderness) and the adnexae (masses, tenderness, thickening).
Phase 3 — Differential diagnosis construction: after history and examination, list the three most likely diagnoses with the key clinical features supporting each. This active differential forces the clinician to notice what is present and what is absent — a non-tender, irregular, firm mass in a 40-year-old suggests fibroid; the same mass with ascites and weight loss demands urgent ovarian malignancy workup.
Phase 4 — Targeted investigations: select only those investigations that will discriminate between the leading differential diagnoses. For a pelvic mass: pelvic ultrasound (transabdominal or transvaginal) is the first investigation. For vaginal discharge: vaginal pH, wet mount microscopy, and whiff test can be performed at the bedside in any OPD. For genital ulcers: dark-field microscopy or syphilis serology (VDRL + TPHA) for suspected primary syphilis; PCR or viral culture for HSV; syndromic management is appropriate when laboratory confirmation is not available.
SELF-CHECK
A 45-year-old woman presents with a 3-month history of post-coital bleeding and a grey-white watery vaginal discharge with an unpleasant odour. On speculum examination the cervix has an irregular, friable, cauliflower-like lesion that bleeds on contact. What is the most likely diagnosis and the most important immediate investigation?
A. Bacterial vaginosis; vaginal pH and wet mount
B. Carcinoma cervix; Pap smear only
C. Carcinoma cervix; colposcopy-directed biopsy and staging investigations
D. Cervical ectropion; reassurance and follow-up
Reveal Answer
Answer: C. Carcinoma cervix; colposcopy-directed biopsy and staging investigations
Post-coital bleeding, an abnormal discharge, and a friable cauliflower-like cervical lesion in a 45-year-old woman is carcinoma cervix until proven otherwise. A Pap smear alone is insufficient — the macroscopic appearance is suspicious enough to warrant direct biopsy, ideally colposcopy-directed. Staging investigations (chest X-ray, MRI pelvis, renal function) determine extent. Bacterial vaginosis and ectropion do not present with a friable lesion that bleeds on contact.
Case 1 — Suprapubic Lump: Examination, Differential, and Management
A suprapubic or pelvic lump is the presenting complaint when a patient or clinician notices a mass arising from the lower abdomen in the midline or iliac fossa. The structured approach to this presentation begins with the history — how long has the lump been present, is it growing, is it painful, is it associated with menstrual disturbance, urinary symptoms (urinary frequency from bladder compression), or bowel symptoms (constipation from posterior pelvic mass)? Constitutional symptoms (weight loss, anorexia, fever) raise the suspicion of malignancy or infection.
On abdominal examination, a pelvic mass is characterised by: arising from below (cannot get below the mass on palpation); dullness to percussion (solid mass or full bladder); and the direction of movement — uterine masses move side to side; ovarian masses may move more freely. Tenderness suggests infection (PID, tubo-ovarian abscess) or torsion of an ovarian cyst.
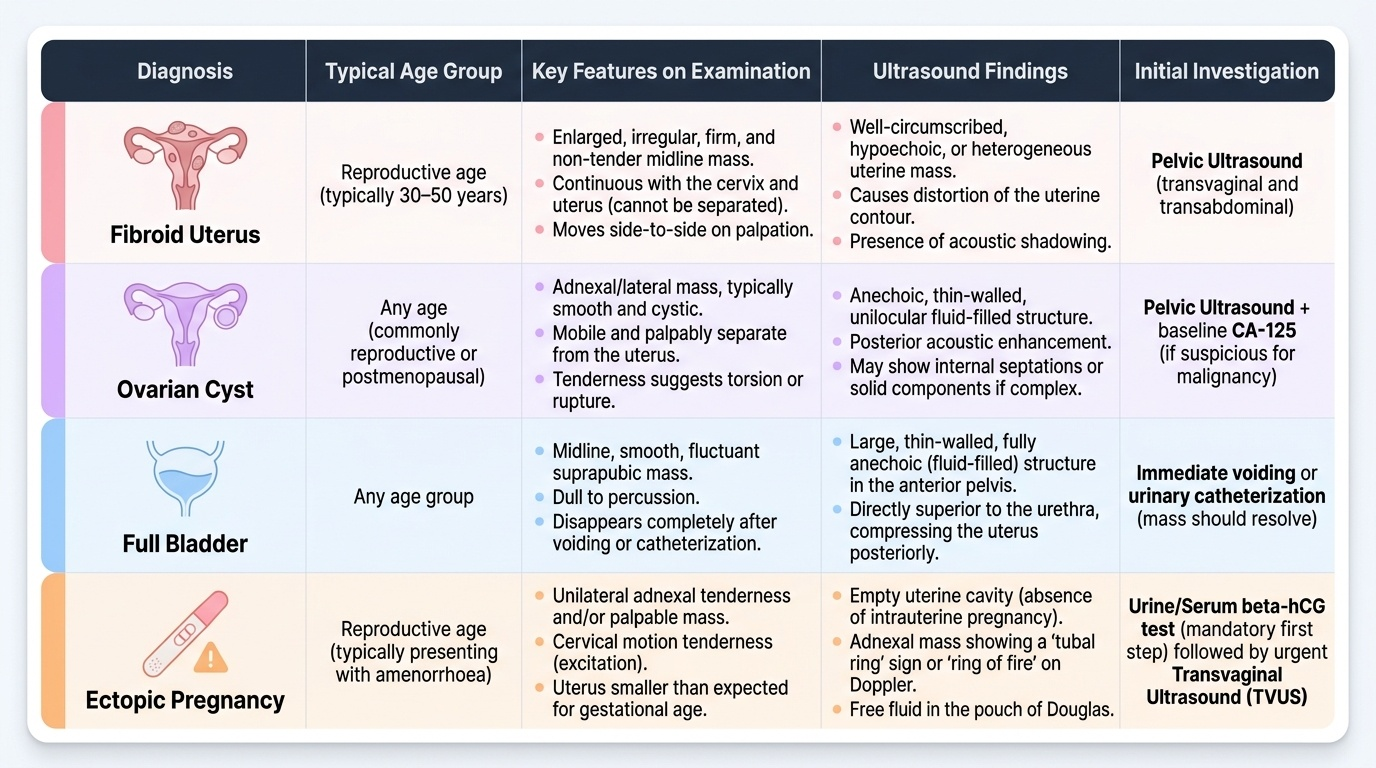
On bimanual examination, the key discriminating features are: Is the mass separate from or continuous with the uterus? A fibroid uterus is the uterus itself — enlarged, irregular, firm, non-tender; the mass cannot be separated from the cervix and uterus. An ovarian cyst is typically lateral, smooth, cystic, separate from the uterus, and mobile. A tubo-ovarian mass (from PID) is adnexal, tender, and often bilateral with uterine tenderness. A retroverted gravid uterus presents as a midline mass in a woman of reproductive age who may be amenorrhoeic — a pregnancy test is mandatory before any further evaluation.
The differential diagnosis of a suprapubic/pelvic lump in a woman includes:
- Fibroid uterus (leiomyoma): commonest cause; irregular, firm, non-tender, arises from the uterus; usually associated with menorrhagia
- Ovarian cyst or tumour: smooth or irregular; separate from the uterus; may be bilateral in malignancy
- Full bladder: midline, cystic, disappears after catheterisation — exclude before further investigation
- Retroverted gravid uterus / pregnancy: midline, soft; β-hCG and ultrasound mandatory
- Ectopic pregnancy: unilateral adnexal mass; pain; positive β-hCG; haemodynamic instability in rupture
- Pelvic inflammatory disease / tubo-ovarian abscess: adnexal; tender; fever; elevated WBC; history of STI
- Carcinoma of ovary or uterus: irregular, may be fixed, associated ascites, constitutional symptoms
Investigations: pelvic ultrasound (transabdominal/transvaginal) is the cornerstone; FBC (anaemia from menorrhagia, leukocytosis in PID); urine pregnancy test (exclude pregnancy always); CA-125 (elevated in epithelial ovarian cancer but also in endometriosis, PID — not specific; use in post-menopausal women with adnexal mass). MRI pelvis for surgical planning in fibroids; CT chest-abdomen-pelvis for ovarian malignancy staging.
Management is diagnosis-specific: fibroids — medical (GnRH analogues, tranexamic acid, oral contraceptives for symptoms) or surgical (myomectomy if fertility desired, hysterectomy if not); ovarian cysts — observation for functional cysts <5 cm in premenopausal women; surgical excision (laparoscopic or open) for persistent or large cysts; emergency surgery for torsion.
Provided image
SELF-CHECK
A 32-year-old woman presents with a right-sided lower abdominal lump. She is 6 weeks amenorrhoeic and has had mild lower abdominal discomfort. Her BP is 90/60 mmHg and pulse is 110/min. What is the priority diagnosis and the immediate management step?
A. Ovarian cyst; arrange elective ultrasound
B. Ruptured ectopic pregnancy; IV access, fluid resuscitation, serum β-hCG, and emergency surgical referral
C. Fibroid uterus with degeneration; analgesia and elective investigation
D. Appendicitis; surgical consultation and IV antibiotics
Reveal Answer
Answer: B. Ruptured ectopic pregnancy; IV access, fluid resuscitation, serum β-hCG, and emergency surgical referral
Amenorrhoea, right-sided adnexal lump, lower abdominal pain, and haemodynamic instability (BP 90/60, pulse 110) in a woman of reproductive age constitutes a ruptured ectopic pregnancy until proven otherwise. This is a surgical emergency. The priority is IV access, fluid resuscitation, urgent serum β-hCG, and immediate referral for emergency surgery (laparoscopy or open). Waiting for elective imaging in a haemodynamically unstable patient is dangerous.