Page 13 of 20
OG19.3 | Tubal Ligation Observation — SDL Guide
Learning Objectives
- Observe and describe the surgical steps of tubal ligation including modified Pomeroy, fimbriectomy, and laparoscopic occlusion techniques (OG19.3)
- Explain the clinical indications and the counselling requirements for female surgical sterilisation
- Identify the anatomical landmarks visible during tubal ligation and correlate these with the tubal anatomy
- Recognise intraoperative complications and describe the decision points a supervising surgeon makes during the procedure
- Apply the legal and ethical framework governing informed consent for permanent sterilisation in India
INSTRUCTIONS
Tubal ligation is one of the most widely used contraceptive methods globally and the most commonly used in India, where female surgical sterilisation accounts for approximately 37% of contraceptive use (NFHS-5). Unlike the other procedures in this cluster, the NMC competency for tubal ligation (OG19.3) is set at observe/assist level — you are expected to understand, witness, and assist with the procedure, not to perform it independently. This distinction reflects the surgical complexity of the operation and its permanent nature. This module prepares you to maximise the learning value of your theatre observation sessions and to understand the counselling, consent, and technical decisions the surgeon makes.
References
- DC Dutta's Textbook of Gynecology, 8th ed. Ch. 28 — Contraception; Sterilisation (textbook)
- Shaw's Textbook of Gynaecology, 17th ed. Ch. 27 — Family Planning and Sterilisation (textbook)
- WHO Selected Practice Recommendations for Contraceptive Use, 3rd ed. 2016 (guideline)
- CREST Study (US Collaborative Review of Sterilization) — 10-year cumulative failure rates by sterilisation method, Peterson 1996 (evidence)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 32-year-old woman, gravida 4 para 4, is on the operating list for postpartum tubal ligation 24 hours after her fourth normal vaginal delivery. She has been counselled during her antenatal period and has signed her consent form. As the junior doctor assisting in the theatre, you notice that she seems anxious and says: 'I'm worried — is this permanent? I just want to make sure I understand what happens.' The operating surgeon is scrubbing in. You have two minutes to address her concern correctly: acknowledge the permanence clearly, confirm that she still consents, and escalate appropriately if she has changed her mind. This scenario illustrates that the observe/assist role in tubal ligation is not merely technical — it requires you to understand the procedure fully enough to support the patient and the team, and to recognise when the ethical threshold of informed consent has not been met.
WHY THIS MATTERS
Female surgical sterilisation is the most commonly used contraceptive method in India, accounting for approximately 37% of married women using contraception (NFHS-5 2021). It is also the method with the most significant ethical and legal weight — it is permanent, and reversibility (salpingo-neostomy or IVF) is expensive, technically demanding, and not reliably successful. As a future clinician at any level of the health system, you will encounter patients who have undergone sterilisation, who are considering it, or who present with post-sterilisation complications (ectopic pregnancy, regret, failed procedure). Understanding the procedure — even at an observe/assist level — enables you to counsel patients correctly, identify complications, and contribute meaningfully to the surgical team during your theatre postings.
RECALL
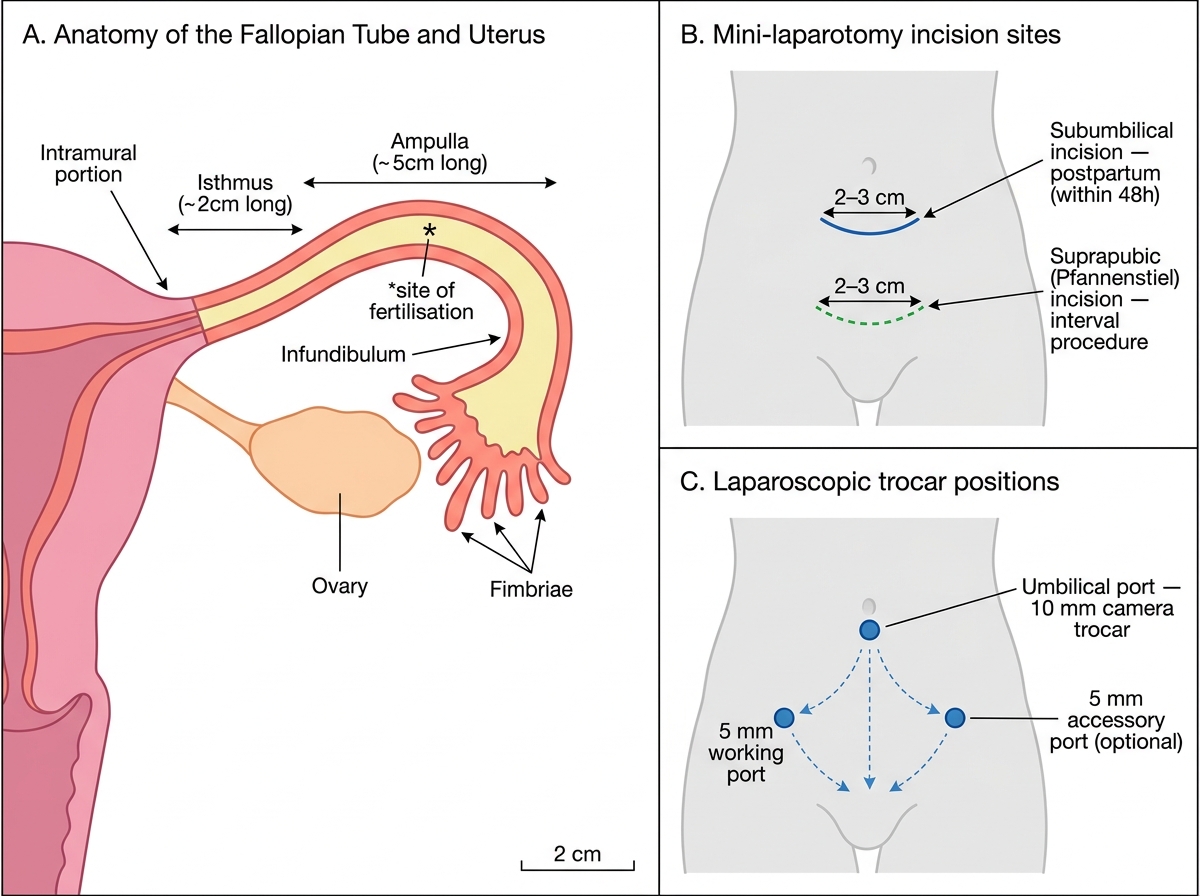
Recall the relevant anatomy before entering the theatre. The fallopian tube connects the lateral angle of the uterine cavity to the ovary; it is divided into four segments from medial to lateral: (1) intramural (within uterine wall), (2) isthmus (narrowest, nearest the uterus, 2-3 cm long — the segment occluded in modified Pomeroy), (3) ampulla (widest, 5-8 cm long — site of fertilisation), (4) infundibulum with fimbriae (finger-like projections that sweep the ovum from the ovarian surface). The tube is suspended in the free edge of the broad ligament (mesosalpinx), which contains its blood supply from the uterine and ovarian arteries. The uterus at 24 hours postpartum is enlarged and reaches the umbilicus — this is why postpartum sterilisation uses a subumbilical mini-laparotomy (the fundus is immediately below the incision) rather than the suprapubic approach used at interval sterilisation.
Clinical Indications and Counselling for Permanent Contraception
Tubal ligation is a method of permanent contraception, and its clinical indication is accordingly specific: it is appropriate for a woman who has completed her family and who, after thorough counselling on alternatives and the permanent nature of the procedure, makes a fully informed, voluntary, and autonomous request for sterilisation. This is not a clinical indication in the same sense as an antibiotic indication — it is an autonomous patient decision, and the clinician's role is to ensure that the decision is fully informed and free from coercion, to identify women at high risk of post-sterilisation regret, and to present reversible long-acting alternatives (IUCD, implant, vasectomy) so that permanent sterilisation is chosen with full knowledge of the options. The failure to counsel adequately is the most common cause of medico-legal liability in sterilisation in India.
Who requests sterilisation: Any woman aged 18 years or above (with no upper age limit) who has completed her desired family size, after counselling on alternatives. In India, the most common scenario is postpartum sterilisation at the time of delivery or within 48 hours, when the woman is already in hospital and highly motivated. Interval (non-postpartum) sterilisation is typically performed as a daycase or short-stay procedure.
Risk factors for post-sterilisation regret (counsel carefully — may benefit from reversible LARC instead):
- Age below 30 years at time of request
- Recent bereavement or family disruption
- Unstable marital relationship
- Sterilisation under pressure from partner or family
- No male children (particularly in settings with son preference)
- History of mental health conditions
Consent requirements in India: Informed voluntary consent must be in writing; the patient must be of sound mind and adult age (≥18 years); spouse consent is NOT legally required since the sterilisation programme guidelines were revised in 1975, but is conventionally sought as a counselling conversation. The Compensation Scheme for Sterilisation Failure (Government of India 2013) provides financial compensation when the procedure fails — this should be mentioned during counselling as evidence of government accountability, not to alarm the patient.
Counselling content: permanence (reversal is expensive and success rates are around 40-70% depending on technique and time elapsed); realistic failure rate (approximately 0.4% for modified Pomeroy over the first year; cumulative 10-year risk approximately 1.85% per CREST study); ectopic pregnancy risk if the procedure fails (ectopic risk is disproportionately elevated after sterilisation failure — approximately 7 times the baseline rate); anaesthetic risks (procedure requires regional or general anaesthesia); alternatives (IUCD, implant, vasectomy — less invasive, reversible, comparably effective).
Anatomy of the Fallopian Tube and Surgical Access Routes
The anatomy visible through the surgical incision or laparoscope during tubal ligation is directly determined by the route of access chosen, and each route has a characteristic field of view that the observer must learn to orient themselves in before the procedure begins. The two principal routes are mini-laparotomy (the more common approach in India, particularly for postpartum sterilisation) and laparoscopy (increasingly used for interval sterilisation in urban centres with laparoscopic equipment).
Mini-laparotomy anatomy: A small infraumbilical (postpartum) or suprapubic (interval) incision of 2-3 cm gives access to the anterior peritoneal cavity. The uterus is elevated with a uterine elevator (or a vulsellum on the cervix) to bring the fallopian tubes close to the incision. The fallopian tube is identified by its characteristic smooth white appearance (distinguishing it from the round ligament, which is more medial and cord-like, and the ovarian ligament, which runs from the ovary to the uterus). The isthmic portion — the narrow segment 1-2 cm lateral to the uterine cornu — is the standard site for most ligation techniques. The mesosalpinx (the peritoneal fold containing the tubal blood supply, branches of the uterine and ovarian arcades) runs inferior to the tube and must be handled carefully to avoid haemorrhage.
Laparoscopic anatomy: Two or three small port incisions (umbilical camera port plus one or two operating ports) allow passage of the telescope and operating instruments. The pelvis is viewed magnified from below; the uterus is manipulated by a uterine manipulator; the tubes are identified by their characteristic appearance and traced from the cornu to the fimbriae to confirm their identity before any occlusion.
Critical anatomical hazards the observer notes:
- Adhesions (from prior surgery, endometriosis, PID) may distort anatomy and require adhesiolysis before tubes can be safely identified
- The ureter runs close to the uterine vessels and must not be mistaken for or damaged during dissection
- The ovarian vessels in the mesovarium lie close to the tubal blood supply — inadvertent ligation risks ovarian ischaemia
Fallopian Tube Anatomy and Surgical Access Routes for Tubal Ligation
Techniques of Tubal Ligation: What the Observer Sees
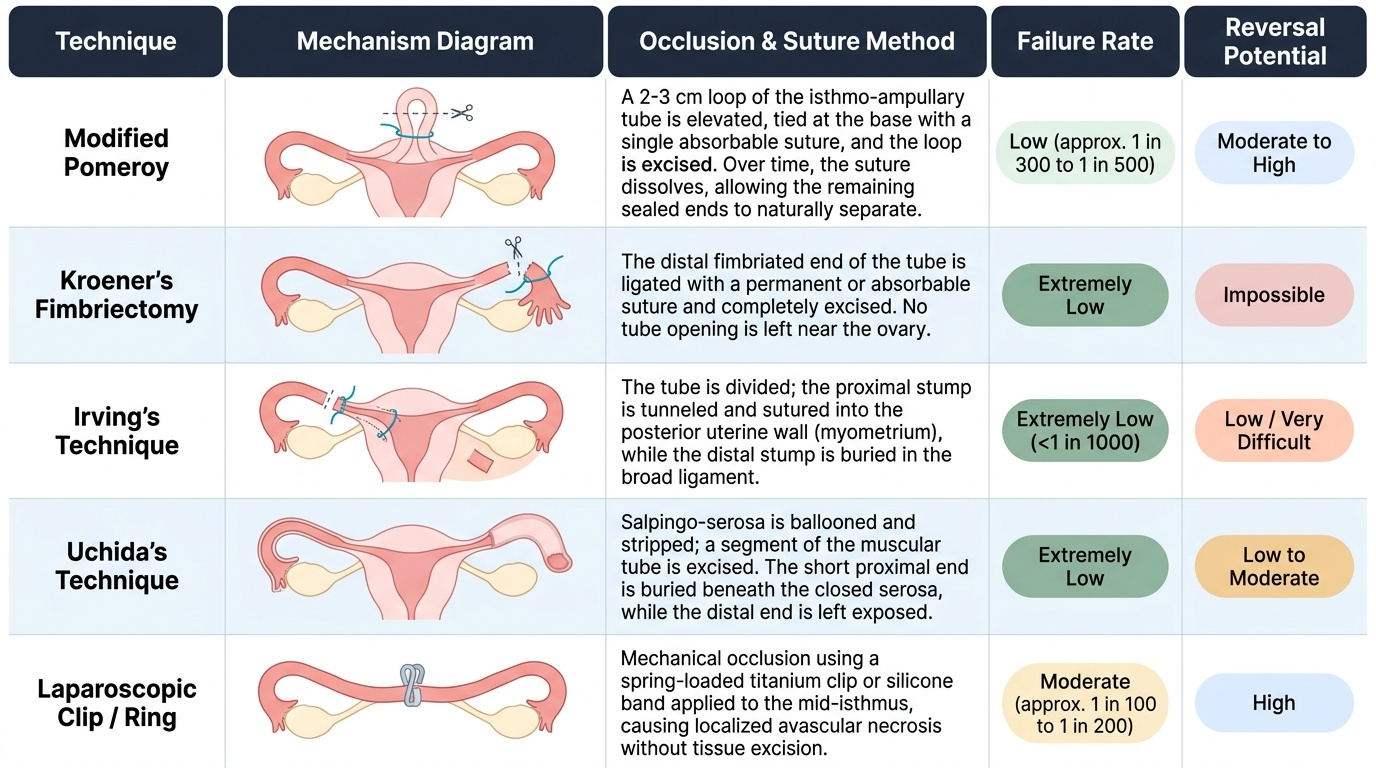
Multiple techniques of tubal occlusion have been described, each with different tissue handling, suture or mechanical requirements, and varying failure rates and reversal potential. As an observer, you should be able to identify which technique is being used from the operative steps you witness, and understand the anatomical and mechanical rationale for each technique. The most important distinction to internalise is between techniques that excise a segment of tube (modified Pomeroy, fimbriectomy, Uchida) and those that occlude the tube without excision (Irving, laparoscopic ring, clip), because this distinction determines both reversal potential and histological confirmation of the correct structure.
Modified Pomeroy technique (most common in India):
A 2-3 cm loop of the isthmo-ampullary portion of the tube is elevated; the base of the loop is ligated with a single absorbable suture (e.g., chromic catgut or polyglactin); the loop is excised; the specimen (showing tubal lumen on cut section) is sent for histology to confirm that the tube and not the round ligament was excised. As the absorbable suture dissolves over weeks, the two cut ends separate and are sealed by fibrosis — creating the characteristic 'gap' visible on reversal surgery. The observer should watch for: (1) confirmation of tube identity before ligating; (2) mesosal-phinx bleeding after loop excision (a suture or diathermy point to the bleeding vessel is applied); (3) the histological specimen being correctly labelled with right and left.
Fimbriectomy (Kroener's fimbriectomy): The distal fimbriated end of the tube is ligated and excised. Failure rate is very low (no tube to reopen) but reversal is impossible. Occasionally used when adhesions prevent isthmic access.
Irving's technique: The tube is divided in the isthmic portion; the proximal end is buried within a pocket in the myometrium; the distal end is buried in the broad ligament. This technique requires more surgical skill but has one of the lowest failure rates. The observer will see the creation of myometrial and broad ligament pockets.
Uchida's technique: Injection of saline or adrenaline under the tubal serosa causes separation of serosa from muscularis; the muscularis is excised while the serosa is preserved to create a peritoneal cover; low failure rate, good for reversal. The observer will see the distinctive submucosal injection step.
Laparoscopic techniques (Falope ring/silicone band, Filshie/Hulka clip, bipolar diathermy): Under laparoscopic vision, the isthmus is identified; either a silicone ring is applied using a ring applicator (visible as a tight constriction), or clips are applied, or bipolar diathermy coagulates a 3 cm segment of tube. Clip and ring methods have slightly higher failure rates than Pomeroy but are reversible; diathermy failure rate is very low but reversal is very difficult.
Provided image
SELF-CHECK
During a modified Pomeroy tubal ligation, the surgeon excises the tube loop and the specimen is sent to histology. Why is histological confirmation of the specimen important?
A. To check for pre-malignant changes in the fallopian tube epithelium
B. To confirm that the correct structure (fallopian tube) was excised and not the round ligament
C. To determine whether the patient needs HPV vaccination post-operatively
D. To grade the degree of tubal inflammation and plan antibiotic therapy
Reveal Answer
Answer: B. To confirm that the correct structure (fallopian tube) was excised and not the round ligament
The round ligament and the fallopian tube are adjacent structures with similar macroscopic appearance, particularly in a difficult surgical field (adhesions, obesity, previous surgery). Histological confirmation that the excised specimen contains tubal epithelium (ciliated columnar epithelium) and tubal muscularis confirms that the correct structure was excised. If only the round ligament was excised, the patient is not protected against pregnancy and would need a repeat procedure. This is not primarily about malignancy screening (A) or infection (D). HPV vaccination is unrelated to tubal surgery (C).