Page 2 of 27
OG37.1 | Caesarean Section Observation — SDL Guide (Part 2)
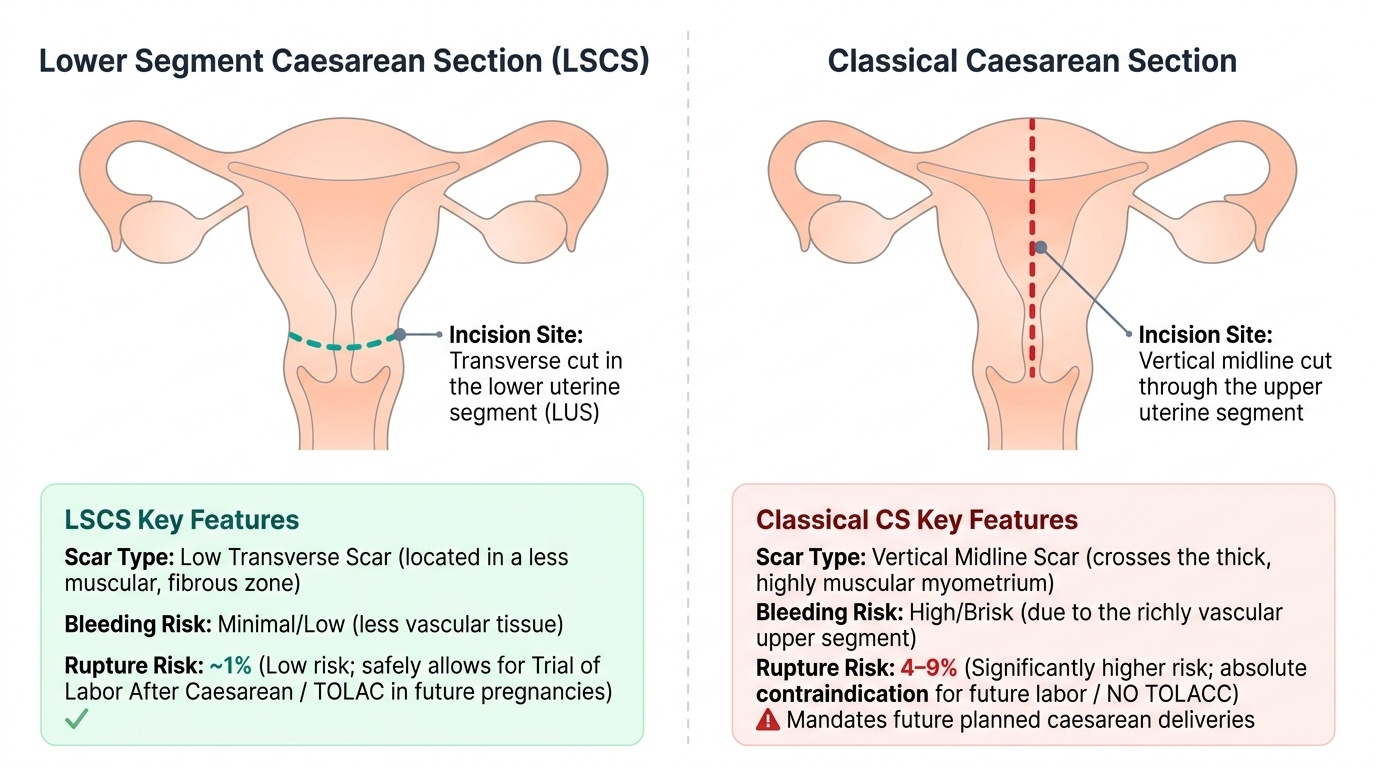
Classical Caesarean Section — When and How It Differs
The classical caesarean section is a far less common operation today, used in specific clinical situations where the lower uterine segment cannot be safely accessed or where rapid delivery demands it. Understanding its distinct features helps the observer appreciate the surgeon's choice when it is made.
The classical incision is a vertical midline incision through the upper uterine segment, extending from the isthmus superiorly toward the fundus. This incision traverses the thick, richly vascular upper segment myometrium and therefore bleeds more briskly than an LUS incision. More importantly, the classical uterine scar has a significantly higher risk of rupture in subsequent pregnancies — typically quoted as 4–9% compared to <1% for LSCS scars — which is why classical CS nearly always commits the woman to a future planned caesarean (no trial of labour after classical caesarean, TOLACC).
Indications for classical CS include situations where the LUS is inaccessible or inadequate:
- Dense bladder adhesions from previous surgeries that preclude safe bladder reflection
- Anterior placenta praevia with an extremely vascular lower segment
- Transverse lie with the back down and the LUS poorly formed (especially in preterm deliveries)
- Cervical carcinoma where lower-segment access would violate tumour margins
- Very preterm gestation (often <28 weeks) where the LUS has not formed
- Perimortem caesarean section where speed is paramount
The postero-fundal approach (De Lee incision) is a further variant, useful for posterior placenta praevia, but is rarely seen in practice. As an observer, if the surgeon makes a vertical uterine incision rather than the expected transverse lower-segment cut, it is worth noting the indication in your logbook — this is a higher-risk procedure with important implications for future obstetric management of the patient.
Provided image
SELF-CHECK
A 24-year-old primigravida is in active labour at 38 weeks with a fetal bradycardia lasting 6 minutes that does not resolve with position change or oxygen. The decision to perform an emergency CS is made. Which urgency category does this case fall into?
A. Category I — immediate threat to fetal life; target delivery within 30 minutes
B. Category II — fetal compromise but not immediately life-threatening
C. Category III — no compromise; delivery needed soon
D. Category IV — elective, at a time of choice
Reveal Answer
Answer: A. Category I — immediate threat to fetal life; target delivery within 30 minutes
A prolonged fetal bradycardia that does not resolve with conservative measures represents an immediate threat to fetal life — this is Category I CS. The target delivery time is within 30 minutes of the decision (NICE NG192). Category II applies to compromise that is concerning but not immediately life-threatening.
Intraoperative Findings and Decision Points to Watch
For an observer at a caesarean section, the ability to identify what the surgeon sees — and to understand the decisions being made in real time — is what separates purposeful observation from passive attendance. Several specific intraoperative findings and decision points recur regularly and are worth watching for.
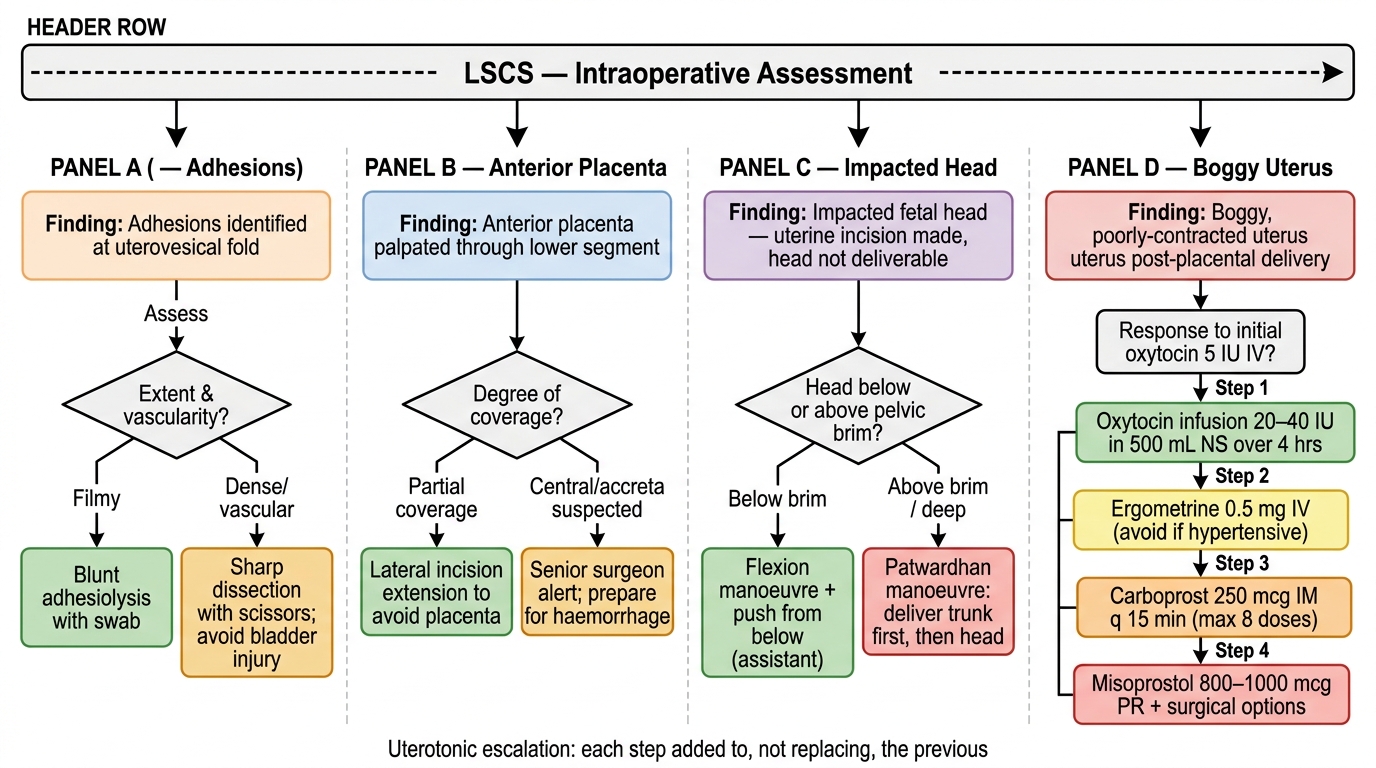
Adhesions and previous scar. In a woman with a previous CS (or previous pelvic surgery), the anterior abdominal wall layers and the uterovesical peritoneum may be densely adherent. Watch how the surgeon carefully dissects these away with a combination of sharp scissors and blunt separation. The bladder may be pulled up higher than expected, making the flap creation hazardous; you will see the surgeon advance more cautiously and potentially ask for a catheter check. Adhesiolysis at this stage can add 15–30 minutes to the operative time.
Lower segment assessment. Before making the uterine incision, the experienced surgeon briefly assesses the LUS: Is it well-formed and thin (as expected at term)? Is the placenta anterior and palpable through the LUS (a sign of placenta praevia or low-lying placenta — the surgeon may change the incision level or prepare for increased bleeding)? Is the lower segment paper-thin with bulging membranes (a nearly ruptured scar — speed becomes essential)?
Fetal head engagement and extraction technique. If the head is deeply engaged (moulded into the pelvis), the routine hand-under-the-head manoeuvre alone may not deliver it. Watch for the surgeon asking an assistant to push the head up from below through the vagina (disimpaction) or using Wrigley's forceps inside the uterus to lever the head up. These are normal tools for an impacted head at CS — do not be alarmed.
Uterine tone after delivery. Immediately after placental delivery, the uterus should contract and become firm. Watch and feel (from a distance) whether the uterus is firm, boggy, or bleeding. A boggy atonic uterus means the oxytocin has not yet taken effect or there is uterine atony — the surgeon will increase oxytocin rate, perform bimanual compression, or administer additional uterotonics.
Uterine closure inspection. Watch how the surgeon checks both lateral angles of the uterine incision (the 'corners') before and after suturing — these are the most common sites of incomplete haemostasis. The surgeon will typically apply angle sutures first to secure both lateral ends before the main closure run. Observe whether the uterine wall looks well-perfused (pink, contractile) as closure is completed.
Intraperitoneal inspection. Before closing the peritoneum and fascia, the surgeon inspects the ovaries, fallopian tubes, and the posterior uterine wall for unexpected pathology (fibroids, endometriosis, adhesions). A small fibroid noticed at the time of CS is typically documented and left in situ unless it obstructs the incision.
Intraoperative Decision Points at LSCS
SELF-CHECK
During an LSCS, after delivery of the placenta, the uterus is noted to be boggy and not contracting despite the administration of oxytocin 5 IU IV. The surgical field is filling with blood. What complication is the observer witnessing, and what is the FIRST-line uterotonic the surgeon will add?
A. Uterine atony causing primary PPH; first-line addition is ergometrine 0.5 mg IV
B. Uterine atony causing primary PPH; first-line addition is oxytocin infusion 20–40 IU in 500 mL over 4 hours
C. Uterine rupture; immediate perimortem hysterectomy
D. Uterine inversion; manual replacement
Reveal Answer
Answer: B. Uterine atony causing primary PPH; first-line addition is oxytocin infusion 20–40 IU in 500 mL over 4 hours
A boggy, non-contracting uterus after placental delivery with haemorrhage = uterine atony, the commonest cause of primary PPH. After an initial bolus of oxytocin, the next step is a high-rate oxytocin infusion (20–40 IU in 500 mL). Ergometrine is also used but is contraindicated in hypertension/pre-eclampsia — the safer first escalation is the oxytocin infusion. Uterine rupture presents differently (sudden loss of uterine contour, fetal parts outside the uterus).
Observing for Complications — Recognition at the Scrub Table
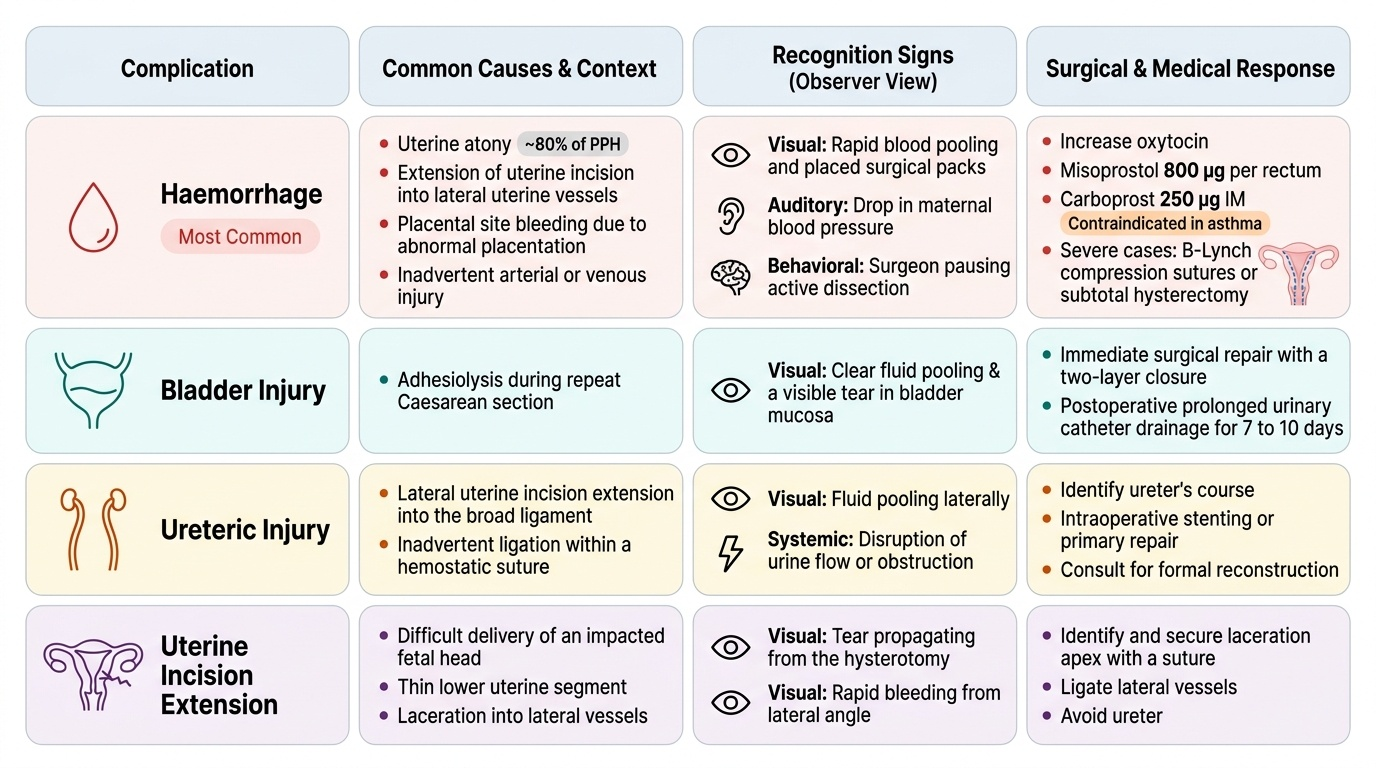
A student who knows what complications can arise — and what they look like — will spot them early, understand the surgeon's urgent responses, and be able to document them accurately in the logbook. The most important intraoperative complications at caesarean section fall into four categories: haemorrhage, urinary tract injury, uterine incision extension, and anaesthetic events.
Haemorrhage is the most common serious complication. Primary haemorrhage at CS most commonly arises from uterine atony (the uterus fails to contract after delivery — accounting for ~80% of PPH), but also from extension of the uterine incision into the lateral uterine vessels, from placental site bleeding with abnormal placentation (accreta, increta, percreta), and from inadvertent arterial or venous injury during entry. Signs the observer will notice: rapidly pooling blood in the retractors despite suction, increasing number of packs placed, the anaesthesiologist calling out a drop in blood pressure, or the surgeon pausing for haemostasis. The oxytocin infusion rate will be increased, additional uterotonics ordered (misoprostol 800 µg per rectum, carboprost 250 µg IM — noting that carboprost is contraindicated in asthma), and in severe cases the surgeon will apply B-Lynch compression sutures or proceed to subtotal hysterectomy.
Bladder injury is recognised by a sudden appearance of clear fluid in the surgical field (urine) or by a visible rent in the bladder mucosa. This typically occurs during adhesiolysis in a previous-CS patient. The repair involves two-layer closure of the bladder wall and prolonged catheter drainage postoperatively (7–10 days).
Ureteric injury is rare but serious; it typically occurs if the lateral uterine incision extends too far and a suture inadvertently includes the ureter. Recognition intraoperatively is difficult; many cases present postoperatively with urine leakage or obstructive uropathy.
Uterine incision extensions — lateral tearing of the uterine incision into the uterine vessels — occur when the fetal head is impacted or the uterine wall is thin. The surgeon will apply haemostatic sutures immediately at the lateral angles.
Anaesthetic complications are managed at the head end; the observer should watch for sudden hypotension (spinal block) managed with IV fluids, ephedrine, or phenylephrine, and for very rare events like high spinal block (respiratory distress) that require emergency management.
Provided image