Page 10 of 27
OG37.4-5 | D and C with EA-ECC Observation — SDL Guide (Part 2)
Dilatation and Curettage (D&C) — Step-by-Step Observation
Following EUA, the D&C proceeds through a defined sequence of instrumentation. Each step builds on the anatomical information gathered in the EUA, and the observer who follows each step will understand why the instruments are used in this specific order.
Step 1 — Uterine sounding. A uterine sound (a thin, slightly curved metallic probe calibrated in centimetres) is gently inserted through the cervical os, directed according to the uterine position confirmed on EUA, until the fundus is lightly touched. The depth is read from the calibrations — this tells the surgeon the uterocervical length and the depth to which instruments can safely be inserted. Forcing the sound beyond the fundal length risks perforation. If the sound does not pass easily, gentle rotation and minimal force are applied; never force the sound.
Step 2 — Cervical dilatation with Hegar dilators. Hegar dilators are a matched set of smooth-tipped metallic dilators in incrementally increasing diameters (sizes 3 through 12 mm). The surgeon begins with the smallest size that fits snugly in the os and progressively inserts the next size in sequence, gently dilating the cervix with a rotational motion. The resistance of the internal os is felt as a distinct 'give' when each dilator passes through. The required final dilatation depends on the procedure: diagnostic curettage typically requires dilatation to 7–8 mm (Hegar 7–8); ERPC may require dilatation to 10–12 mm for suction curette insertion. Watch the surgeon avoid vigorous force — the cervix can lacerate if dilatation proceeds too rapidly.
Step 3 — Curettage. Once adequately dilated, the sharp curette (a metal loop with a sharpened edge, in sizes 1–7) is inserted to the fundal depth and drawn downward with firm pressure against the uterine wall in a systematic fashion: anterior wall, posterior wall, right lateral, left lateral, and fundal wall. The force required should be firm but not excessive; a characteristic 'gritty' sensation against the endometrial wall is normal. Excessive yield of tissue or absence of any gritty sensation are both informative — the former may indicate hyperplastic endometrium or products of conception; the latter may indicate an atrophic cavity.
Step 4 — Specimen collection. Curetting material is collected either on a gauze held at the cervical os or by aspiration. All tissue is placed into a specimen jar with appropriate fixative (formalin). The jar is labelled with the patient's details and the histology request form states the clinical indication, the relevant history (postmenopausal, tamoxifen use, LMP), and any relevant examination findings.
Suction curettage (for ERPC): When the procedure is an ERPC for retained products of conception, a Karman cannula or rigid metal suction curette connected to a vacuum source is used instead of or in addition to the sharp curette. Suction is gentler on the cavity walls and more efficient at evacuating soft products. A sharp curette is used afterward to confirm completeness of evacuation.
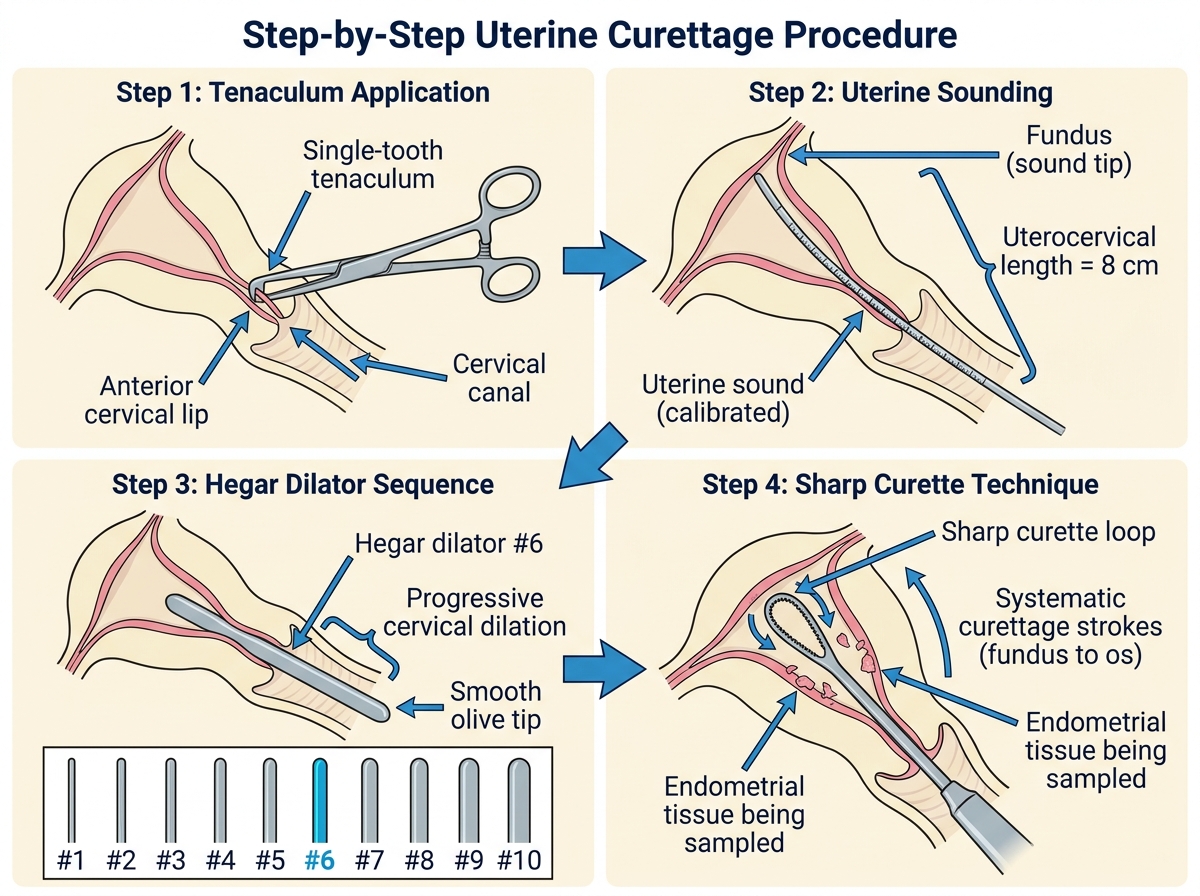
Figure: D&C Operative Sequence — Tenaculum, Sounding, Dilation, and Curettage
Endometrial Aspiration and Endocervical Curettage (EA-ECC) — Observation
Endometrial aspiration and endocervical curettage use smaller-calibre instruments and are often performed with less cervical dilatation than a full D&C. The technique and, critically, the ORDER of the procedures when both are performed together are what the observer must focus on.
Endometrial Aspiration (EA) with a Karman cannula (a flexible plastic suction cannula, typically 4–6 mm diameter) or a pipelle device (a thin flexible plastic tube with a piston that creates negative pressure by retraction) can sample the endometrium with minimal dilatation or even without formal dilatation in a parous woman with a patulous os. The cannula is inserted to the fundal depth confirmed by sounding, and aspiration is performed by rotating the device 360 degrees while moving it back and forth in the cavity to sample all walls. The aspiration specimen (endometrial tissue mixed with a small amount of blood) is collected into the cannula barrel and expelled into a specimen jar. The amount of tissue is often small — a thin strip of endometrium — but in experienced hands this is adequate for histological diagnosis in most cases.
Endocervical Curettage (ECC) uses a small-calibre Kevorkian curette (a ring curette with a small cutting edge) inserted only into the endocervical canal — NOT advanced beyond the internal os. The instrument is drawn downward along all four quadrants of the endocervical canal, and the scrapings are collected directly into a separate specimen jar. The endocervical specimen must be labelled and sent separately from any endometrial specimen.
Fractional curettage — the critical order: When both ECC and endometrial sampling are performed in the same session (e.g., for investigation of suspected endometrial carcinoma or staging of known carcinoma), the ECC MUST be performed FIRST, before any endometrial instruments are inserted. This is the 'fractional' element: the endocervical specimen is collected first, sealed and labelled, then the endometrial sample is obtained separately. If the endometrial curette is used first, blood and fragments of endometrial tissue will wash down into the endocervical canal, contaminating the ECC specimen and rendering it impossible to determine whether malignant cells are of endocervical or endometrial origin. Watch the scrub nurse ensure both specimen jars are labelled and sealed before the procedure is declared complete.
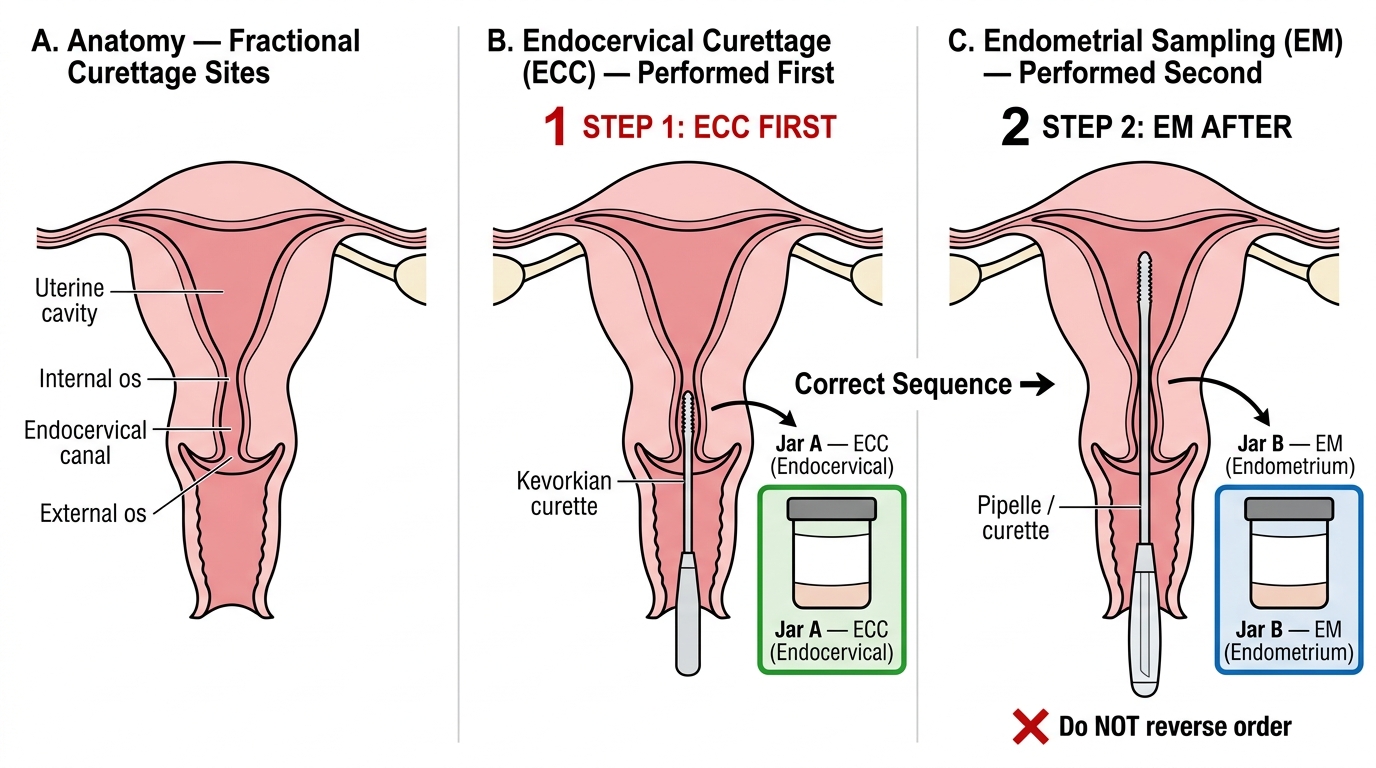
Fractional Curettage Sequence — ECC Before Endometrial Sampling
SELF-CHECK
A surgeon is performing EUA + D&C + ECC for a 54-year-old woman with postmenopausal bleeding and a thickened endometrium on ultrasound. What is the correct order of the procedures, and why?
A. Endometrial curettage first, then ECC — the endometrium is the primary concern
B. ECC first, then endometrial curettage — to prevent contamination of the endocervical specimen by endometrial tissue
C. Both simultaneously, as the order does not affect specimen interpretation
D. EUA only; ECC and endometrial sampling should be done separately at hysteroscopy
Reveal Answer
Answer: B. ECC first, then endometrial curettage — to prevent contamination of the endocervical specimen by endometrial tissue
In fractional curettage, ECC must be performed first, before any endometrial instrumentation. If the endometrial curette is used first, blood and endometrial fragments contaminate the endocervical canal, making it impossible to determine from the ECC specimen whether malignant cells originate in the endocervical canal (indicating cervical extension — higher stage) or are simply washed down from the endometrium. This distinction is clinically critical for cancer staging and treatment planning.
Interpreting Findings — Tissue Characteristics and Specimen Handling
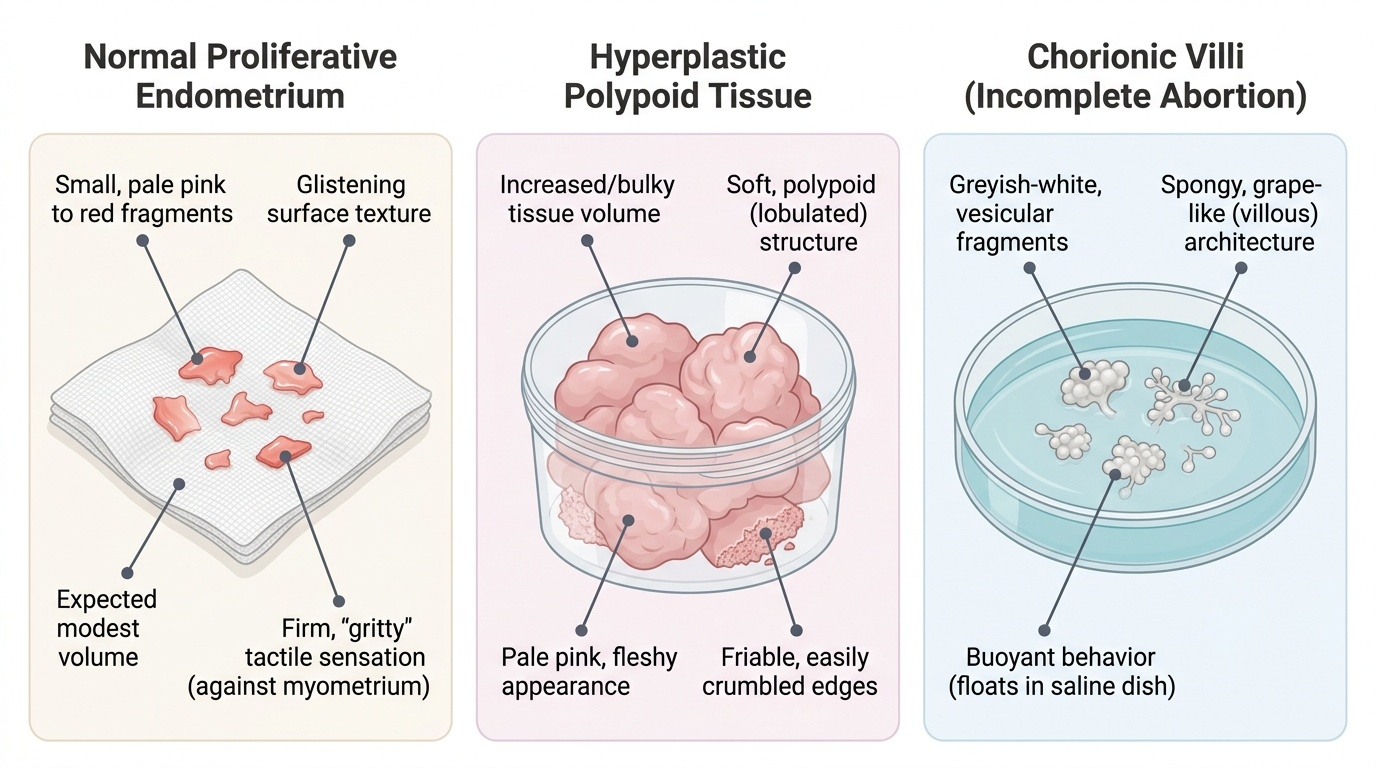
One of the most informative moments in a D&C or EA-ECC is the macroscopic examination of the curettings on the gauze or in the specimen jar. While definitive diagnosis requires histology, the experienced surgeon (and the observant student) can form a useful preliminary impression from the tissue characteristics, quantity, and texture of the material.
Normal proliferative or secretory endometrium appears as small, pale pink to red fragments of soft tissue, often with a glistening surface. In a premenopausal woman undergoing diagnostic curettage, a modest amount of such tissue is expected. The texture when drawn through the curette gives the characteristic 'gritty' sensation of healthy endometrium against a firm myometrial wall.
Endometrial hyperplasia typically yields an increased volume of soft, polypoid, pale pink material. The tissue may appear bulky and friable. Simple hyperplasia produces more tissue than normal; complex hyperplasia with atypia tends to produce easily crumbled, fleshy material. However, these are impressions only — the definitive diagnosis is histological.
Products of conception (incomplete abortion) are recognised by the characteristic greyish-white, vesicular appearance of chorionic villi — small, spongy, grape-like fragments that float in water or saline if tested (the 'float test'). The surgeon may confirm the presence of chorionic villi by placing some tissue in a saline dish and observing whether it floats in a characteristic pattern.
Endometrial carcinoma should be suspected if the curette returns a large volume of necrotic, friable, easily bleeding tissue. However, no macroscopic finding is pathognomonic and all specimens must be sent for histology without exception.
Specimen handling rules: All tissue from the uterine cavity goes into a labelled formalin jar. ECC specimens go into a SEPARATE jar labelled clearly 'ECC' or 'endocervical' to distinguish from the endometrial specimen. The histology request must state: patient name and date of birth, clinical indication, relevant history (LMP, menopausal status, hormone use), EUA findings, and any macroscopic specimen characteristics.
Provided image
SELF-CHECK
During a D&C for suspected incomplete abortion, the curette returns grey-white, vesicular, spongy fragments. The surgeon places some material into a bowl of saline. What is being tested, and what finding confirms the suspected diagnosis?
A. Testing for malignancy; malignant tissue sinks in saline
B. Testing for chorionic villi; villi float and assume a characteristic spongy pattern in saline, confirming retained products of conception
C. Testing for endometrial hyperplasia; hyperplastic tissue absorbs water and changes colour
D. Testing for fibroid tissue; fibroid fragments are firm and do not disperse in saline
Reveal Answer
Answer: B. Testing for chorionic villi; villi float and assume a characteristic spongy pattern in saline, confirming retained products of conception
The 'float test' identifies chorionic villi: when placed in saline, chorionic villi float and assume a delicate, arborescent (tree-like) pattern due to their spongy, fluid-filled villous structure. This confirms the presence of retained products of conception (trophoblastic tissue) and validates that the curettage was performed in the correct clinical context. Malignant tissue, fibroid fragments, and normal endometrium do not float in this characteristic pattern.