Page 18 of 27
OG37.7 | First Trimester MTP and Evacuation Observation — SDL Guide (Part 2)
Interpreting Products of Conception and Confirming Completeness
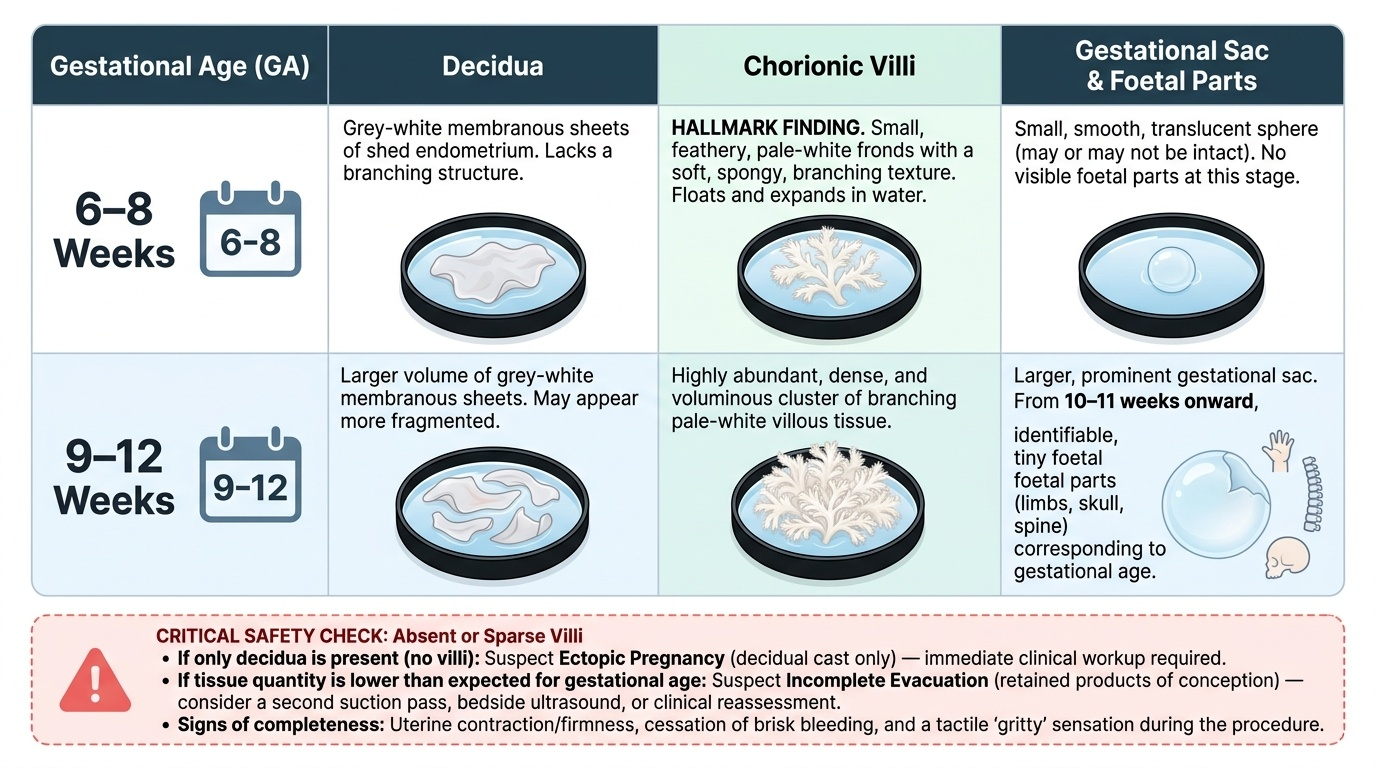
After the evacuation is completed, the surgeon — and the observing student — must examine the aspirated material to confirm that the uterine contents match the expected gestational age and that the evacuation is complete. This is a crucial safety step: incomplete evacuation (retained products of conception, RPOC) leads to continued haemorrhage, infection, and failed procedure. The examination takes place immediately in the procedure room, before the patient leaves the table.
The aspirated material is placed in a shallow tray with water or normal saline, which separates tissue types and allows visual identification. At 6–8 weeks, the expected findings include: chorionic villi — the hallmark finding, appearing as small, feathery, pale-white fronds with a soft spongy texture; decidua — grey-white membranous sheets of shed endometrium; and the gestational sac — a small, smooth, translucent sphere that may or may not be intact. At 9–12 weeks, villous tissue is more abundant, the gestational sac is larger, and from approximately 10–11 weeks onward, identifiable foetal parts (limbs, skull, spine) may be present, the size of which should correspond to gestational age.
The quantity of tissue is assessed against expected volume for gestational age. If villous tissue is absent or sparse relative to gestational age, the surgeon must suspect: (a) ectopic pregnancy — where no intrauterine POC will ever be obtained, and the suction material will show only decidua without villi (a decidual cast); or (b) incomplete evacuation with retained villi, necessitating a second pass or ultrasound guidance.
Clinical signs that confirm complete evacuation alongside POC examination include: reduction in uterine size and firmness, cessation of brisk haemorrhage from the os, and the gritty end-point sensation described above. If any doubt persists, bedside ultrasound — where available — directly visualises residual echogenic material in the uterine cavity.
Provided image
Observing the Procedure: Decision Points, Complications and Escalation
As a final-year student, you will observe rather than perform this procedure. Your structured observation should focus on recognising the decision points where the surgeon pauses, re-assesses, and either proceeds, modifies technique, or escalates. The ability to recognise complications early — even as an observer — is a core clinical skill that prepares you for independent practice and emergency management.
What to observe and why:
Pre-procedure check — you should see the surgeon confirm: uterine position on bimanual examination, gestational age agreement between dates and uterine size, a valid consent form, and a complete patient history (particularly asthma status, which affects use of certain uterotonics postoperatively, and anticoagulant use).
Uterine axis correction — watch for the tenaculum traction straightening the cervico-uterine angle before sounding. If the surgeon changes instrument direction mid-insertion and pauses, this may indicate an unexpected uterine flexion.
Signs of perforation — uterine perforation is the most feared intraoperative complication. The surgeon will notice: sudden loss of the gritty resistance of the decidua, the instrument passing deeper than the sounded depth, a sudden drop in intraoperative resistance, or entry of gas or bowel into the operative field. The patient may report sharp pain even under paracervical block, or vital signs may change. When perforation is suspected, the surgeon stops the procedure immediately and arranges either close observation (if a small midline perforation with no active bleeding) or emergency laparotomy (if bowel injury, vascular injury, or ongoing haemorrhage is suspected).
Signs of incomplete evacuation — if minimal or no villi are retrieved, or if the uterus fails to contract and firm up, the surgeon considers a second pass, ultrasound-guided re-evacuation, or overnight oxytocin infusion with re-assessment.
Post-procedure haemorrhage — a contracted uterus normally produces only modest post-procedure bleeding. Persistent brisk haemorrhage prompts consideration of: uterine atony (treated with oxytocin, ergometrine [contraindicated in hypertension], or misoprostol); cervical or vault laceration (needs inspection and suturing); retained products (repeat evacuation).
Infection — fever, offensive discharge, or uterine tenderness in the immediate post-operative period may indicate endometritis or septic abortion, particularly if evacuation was performed for a missed or incomplete abortion with pre-existing tissue necrosis.
| Complication | Intraoperative sign observed | Immediate response |
|---|---|---|
| Uterine perforation | Instrument depth > sounded depth; sudden loss of resistance | Stop procedure; call senior; consider laparoscopy/laparotomy |
| Incomplete evacuation | Sparse villi; uterus stays enlarged/boggy | Second pass; USS guidance; oxytocin; re-assess |
| Haemorrhage (atony) | Brisk bleeding post-evacuation; uterus soft | Bimanual compression; oxytocin |
| Cervical laceration | Bleeding from tenaculum site or cervical tear | Direct pressure; Allis forceps; suture if needed |
| Vasovagal syncope | Bradycardia, pallor, sweating during cervical dilation | Stop stimulation; IV atropine if needed |
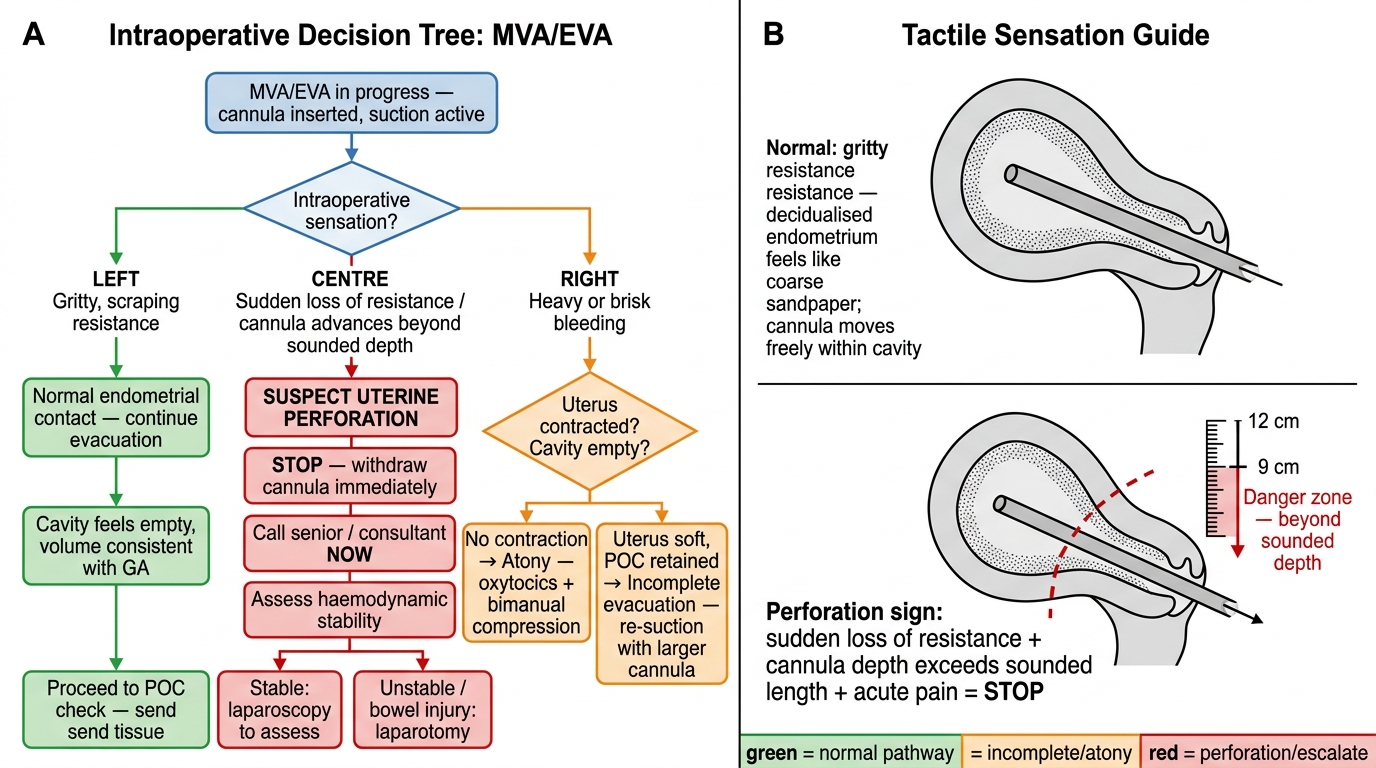
Intraoperative Decision Tree for MVA/EVA and Tactile Sensation Guide
SELF-CHECK
During MVA, the operator notices the cannula has passed to 12 cm depth (uterus sounded to 9 cm), and there is a sudden loss of the gritty sensation. The patient grimaces with pain. What is the most likely complication and the correct immediate action?
A. Vasovagal syncope — administer IV atropine and continue the procedure
B. Uterine perforation — stop the procedure immediately and call a senior
C. Cervical laceration — apply Allis forceps to the cervix
D. Incomplete evacuation — perform a second pass with a larger cannula
Reveal Answer
Answer: B. Uterine perforation — stop the procedure immediately and call a senior
The combination of cannula advancing beyond sounded depth, sudden loss of gritty resistance, and acute pain is the classic triad of uterine perforation. The immediate response is to stop the procedure immediately, call a senior, and evaluate for laparoscopy or laparotomy depending on whether bowel or vascular injury has occurred. Continuing the procedure risks enlarging the perforation and bowel injury.
CLINICAL PEARL
The gritty sensation is your safety feedback during evacuation. Experienced surgeons describe the feel of the cannula moving against the decidualised endometrium as like 'rubbing sandpaper.' When the uterus is empty, this sensation stops and a soft resistance is felt as the uterine walls appose each other — the evacuation is complete. Conversely, if the gritty sensation is never present from the outset, or if it disappears with the instrument going too deep, reconsider anatomy (retroflexed uterus) or perforation. This tactile feedback cannot be seen — it must be understood cognitively so you can recognise it when you eventually perform the procedure yourself.
SELF-CHECK
After an MVA, the surgeon places the aspirated material in water. She asks you: 'I see only membrane-like grey-white tissue, no feathery tissue at all — what does this suggest?' What is the most important differential diagnosis to exclude immediately?
A. Normal finding at gestations below 6 weeks
B. Ectopic pregnancy — this is a decidual cast without chorionic villi
C. Fibroid polyp — a non-pregnant uterus was aspirated
D. Incomplete evacuation requiring a larger cannula
Reveal Answer
Answer: B. Ectopic pregnancy — this is a decidual cast without chorionic villi
Absence of chorionic villi in aspirated material when an intrauterine pregnancy was expected must immediately raise the concern of ectopic pregnancy. In ectopic pregnancy, the uterine aspirate shows only decidua (grey-white membrane) without feathery chorionic villi — this is a decidual cast caused by the hormonal stimulation of the ectopic gestation. The surgeon must urgently arrange serum β-hCG measurement, transvaginal ultrasound, and laparoscopy if ectopic is confirmed.
Self-Assessment: MTP and Evacuation Knowledge Check
Having worked through the legal framework, the anatomy, the technique, and the complication recognition sections of this module, you are now in a position to consolidate your understanding through structured self-questioning. The goal of this section is not to recapitulate what you have read, but to confirm that you have internalised the reasoning that underpins each step — the kind of understanding that allows you to respond quickly and confidently when a senior asks you something at the bedside immediately after an observed procedure. Structured self-testing, particularly the act of retrieving information without looking back, is one of the most evidence-based strategies for durable learning (retrieval practice effect, Roediger & Karpicke). Attempt each question below before reviewing the module, and identify any gaps that require re-reading.
Key recall questions:
- What are the two gestational thresholds in the MTP Act 2021, and what changes at each threshold in terms of the number of RMPs and eligible categories?
- Why does uterine position (anteverted vs retroverted) matter before inserting a uterine sound or cannula?
- What is the difference between MVA and EVA in terms of suction source, portability, and gestational age range?
- What macroscopic feature of aspirated material confirms that intrauterine pregnancy tissue has been retrieved?
- What clinical and tactile signs indicate complete evacuation?
- What is the immediate management when uterine perforation is suspected during MVA?
Quick self-test: Without looking back, write down the two RMP thresholds under MTP Act 2021, the macroscopic appearance of chorionic villi, and two intraoperative signs of uterine perforation. Check your answers against the module content.