Page 5 of 27
OG37.2-3 | Laparotomy and Hysterectomy Observation — SDL Guide
Learning Objectives
- Identify the clinical indications for gynaecological laparotomy and the different types of hysterectomy
- Describe the key pelvic anatomical structures — uterine ligaments, uterine artery, and ureter — that the surgeon must identify and protect
- Follow the sequential steps of a Total Abdominal Hysterectomy (TAH) as an informed observer
- Distinguish the vaginal hysterectomy approach and recognise the circumstances in which it is preferred
- Identify intraoperative findings and interpret the surgical decisions made during the procedure
- Recognise intraoperative complications — particularly ureter injury and haemorrhage — and observe the surgical team's response
- Document an observed hysterectomy accurately in the logbook
INSTRUCTIONS
Hysterectomy is the most commonly performed major gynaecological operation worldwide. As a final-year student, you are required to observe and assist in both laparotomy (OG37.2) and hysterectomy — abdominal and vaginal (OG37.3). This module prepares you to be an active, informed observer in the gynaecological operating theatre rather than a passive bystander. It covers the anatomy, the procedural steps, and the critical decision points you must be able to identify and discuss after each observed case.
References
- DC Dutta's Textbook of Gynaecology, 7th edition, Chapter 24 — Hysterectomy (textbook)
- Shaw's Textbook of Gynaecology, 16th edition, Chapter 20 — Surgical Operations (textbook)
- Te Linde's Operative Gynaecology, 12th edition — Abdominal and Vaginal Hysterectomy (textbook)
- FOGSI Good Clinical Practice Recommendation — Hysterectomy, 2018 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 42-year-old woman with multiple symptomatic uterine fibroids, menorrhagia causing haemoglobin of 7.2 g/dL, and pressure symptoms on the bladder is wheeled into the gynaecological theatre for a total abdominal hysterectomy. Her uterus on ultrasound is 18 weeks in size with at least six intramural and subserosal fibroids. As a medical student observing alongside the registrar, you stand at the right-hand side of the table. The consultant opens the abdomen through a midline vertical incision. Over the next 90 minutes you will watch the surgeon systematically divide each uterine ligament, clip and cut the uterine arteries — pausing to identify the ureter at each side — and finally close the vaginal vault. Every step requires anatomical knowledge to understand. This module gives you that knowledge.
WHY THIS MATTERS
Hysterectomy is performed for a wide range of gynaecological conditions — uterine fibroids, abnormal uterine bleeding, uterine prolapse, endometriosis, and gynaecological malignancies — and ranks among the most frequently performed operations in women globally. As a doctor you will counsel women before hysterectomy, manage postoperative complications, and in some settings act as the first assistant in the operation. The NMC CBME curriculum requires you to observe and assist in laparotomy (OG37.2) and hysterectomy (OG37.3). This module ensures that your time in the gynaecological theatre is educationally purposeful.
RECALL
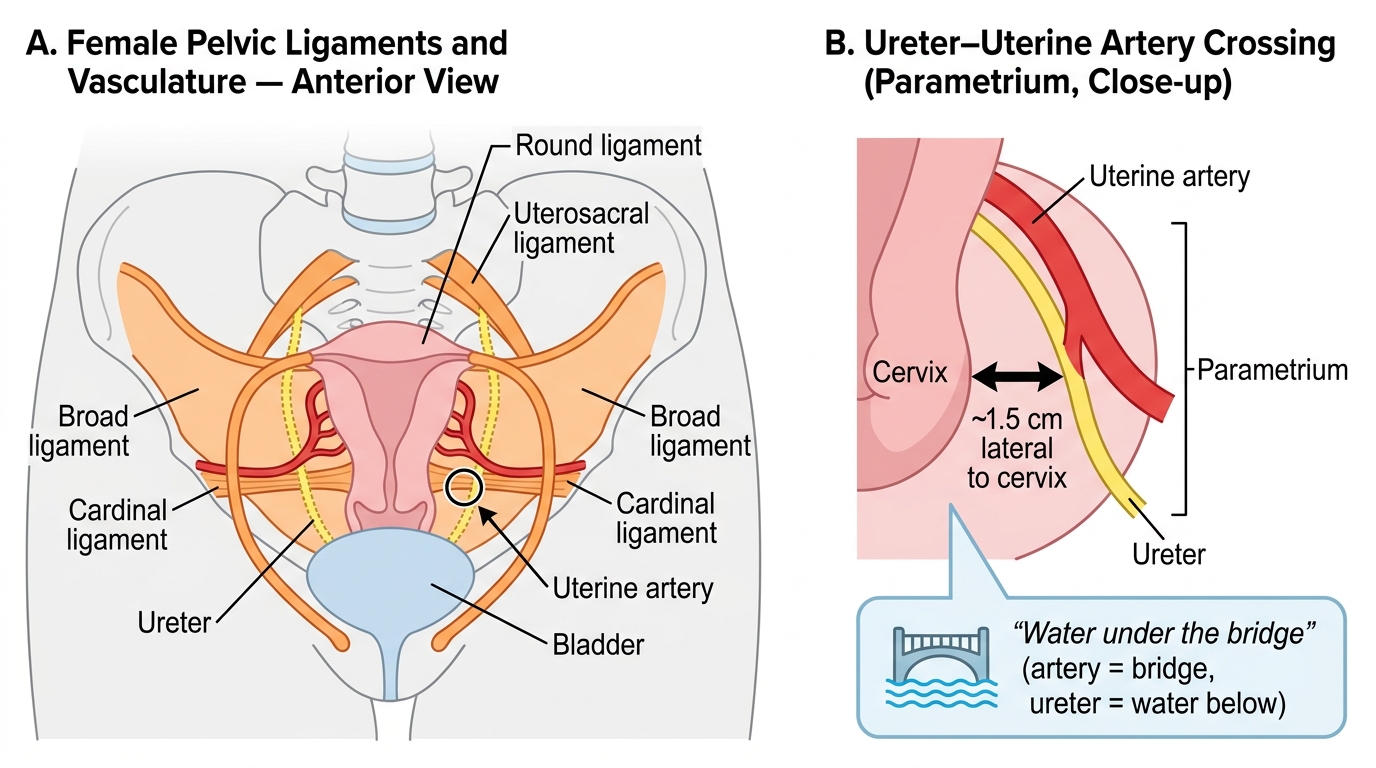
Before proceeding, take a moment to recall the key structures. The uterus is suspended in the pelvis by four pairs of ligaments: the round ligaments (maintain anteversion but are weak), the broad ligaments (a peritoneal fold, not true ligaments, containing tubes and ovaries), the cardinal (transverse cervical) ligaments (the main lateral supports), and the uterosacral ligaments (posterior supports). The uterine artery arises from the internal iliac artery and runs medially within the base of the broad ligament — critically, it crosses over the ureter at the level of the internal cervical os, approximately 1.5–2 cm lateral to the cervix. This 'water under the bridge' relationship is the single most important anatomical fact in hysterectomy. Also recall that the ureters descend along the posterior abdominal wall, cross the pelvic brim at the bifurcation of the common iliac artery, run in the base of the broad ligament, and enter the bladder trigone anteriorly.
Why Laparotomy and Hysterectomy? Indications and Surgical Planning
Understanding clearly why a patient is having surgery before you observe it makes every subsequent step interpretable and gives your observation a purposeful clinical frame. The surgeon's choice of approach — abdominal, vaginal, or laparoscopic — is itself a decision that reflects the indication, the uterine size, the patient's history, and the available expertise.
Gynaecological laparotomy may be exploratory (to diagnose an unknown pelvic mass, ectopic pregnancy, or ovarian torsion) or operative (to perform a procedure such as myomectomy, ovarian cystectomy, tubectomy, or hysterectomy). In emergency settings — ruptured ectopic, massive haemorrhage, torsion — the laparotomy is unplanned and the observer will see rapid decision-making under pressure. In elective settings, the abdomen is opened with a clear operative plan.
Indications for hysterectomy span benign and malignant pathology:
- Fibroids (leiomyomata): the most common benign indication; indicated when fibroids cause menorrhagia refractory to medical treatment, pressure symptoms, or distortion of the uterine cavity in a woman who has completed her family
- Abnormal uterine bleeding (AUB): when hormonal and conservative treatments fail and endometrial pathology is excluded or persistent
- Uterovaginal prolapse: VH is often preferred in this setting as it allows simultaneous pelvic floor repair
- Endometriosis / adenomyosis: when fertility is not desired and symptoms are refractory to medical treatment
- Gynaecological malignancy: cervical cancer (Wertheim's radical hysterectomy), endometrial cancer (TAH + bilateral salpingo-oophorectomy), ovarian cancer (part of cytoreductive surgery)
- Obstetric emergencies: post-partum hysterectomy for refractory PPH, uterine rupture, or placenta accreta spectrum
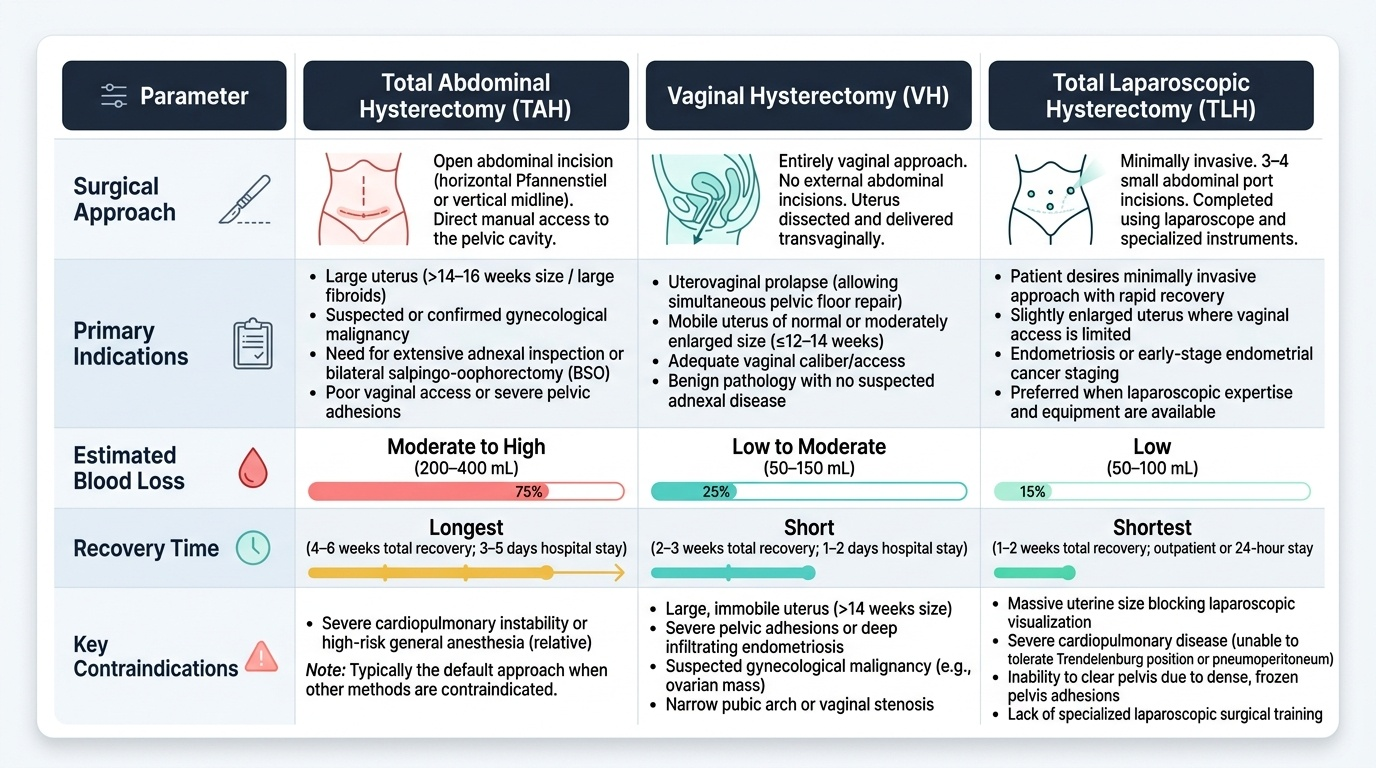
The surgical approach decision:
- TAH is preferred when the uterus is large (>14–16 weeks size), when adnexa need inspection or removal, when malignancy is suspected, or when vaginal access is poor
- VH is preferred when prolapse is present, the uterus is mobile and ≤12–14 weeks size, vaginal access is adequate, and there is no need for adnexal surgery
- TLH (Total Laparoscopic Hysterectomy) is increasingly common where laparoscopic expertise exists, offering faster recovery than TAH
Provided image
Relevant Pelvic Anatomy — What the Surgeon Must Identify
Hysterectomy is, above all else, a procedure defined by its anatomy. Every step in the operation is driven by the need to identify, secure, and protect a specific anatomical structure — and the sequence of those steps is not arbitrary but anatomically logical, designed to minimise bleeding and injury at each stage. As an observer, your task is not simply to watch hands and instruments: it is to track which structure the surgeon is working on, understand why that structure is being addressed at this point in the sequence, and identify the adjacent structures at risk. This interpretive frame transforms a confusing series of clamps and sutures into a comprehensible narrative. The pelvis contains a cluster of structures in close proximity — uterus, bladder, rectum, two ureters, uterine arteries, ovarian vessels — and each one requires the surgeon's active attention before any clamping or cutting at that step. The following guide to the key structures is what you should hold in mind as you observe.
The uterine ligaments are divided sequentially during hysterectomy, each contributing to the uterine suspension:
- Round ligaments are divided first in TAH; they are the 'road markers' that tell the surgeon where the broad ligament begins. Dividing them opens the broad ligament leaf for further dissection.
- Infundibulopelvic (IP) ligament (also called the suspensory ligament of the ovary): contains the ovarian vessels; divided if the ovaries are to be removed. The ureter runs close behind it — identifying the ureter before clamping the IP ligament is mandatory.
- Broad ligament: the peritoneal fold between the round ligament and IP ligament is opened to expose the uterine vessels and ureter within the base of the broad ligament.
- Uterovesical peritoneum: reflected downward to create a bladder flap (identical to CS); this exposes the anterior lower uterus and cervix.
- Uterine artery and veins: ligated at the level of the internal os, after the ureter has been displaced laterally. The classic teaching: 'doubly clamp, cut, and ligate the uterine vessels.'
- Cardinal ligaments (transverse cervical ligaments): the main lateral support of the uterus and cervix; divided in successive bites from lateral to medial, progressively skeletonising the cervix.
- Uterosacral ligaments: divided posteriorly, allowing the cervix and uterus to be separated from the upper vagina.
- Vaginal vault: the cervix is circumscribed at the level of the vaginal fornices, and the specimen is removed; the vault is closed with interrupted or continuous absorbable sutures.
The ureter is the most important structure to protect. Its course — crossing the pelvic brim at the iliac bifurcation, running in the base of the broad ligament medially, crossing under the uterine artery ('water under the bridge'), and entering the bladder trigone — makes it vulnerable at three critical steps: IP ligament clamping (if ovaries are removed), uterine artery ligation, and lateral clamp placement for cardinal ligaments. Watch the surgeon pause at each of these steps to identify or displace the ureter before clamping.
Uterine Ligaments and the Ureter–Uterine Artery Relationship
SELF-CHECK
During a TAH, the surgeon is about to ligate the uterine artery on the right side. Before placing the clamp, what anatomical structure must be identified and displaced laterally, and why?
A. The round ligament, because it may be accidentally ligated at this step
B. The ureter, because it crosses under the uterine artery approximately 1.5 cm lateral to the cervix and is at risk of being included in the clamp
C. The ovarian artery, because it may bleed retrogradely if not secured
D. The internal iliac artery, because uterine artery ligation requires its identification
Reveal Answer
Answer: B. The ureter, because it crosses under the uterine artery approximately 1.5 cm lateral to the cervix and is at risk of being included in the clamp
The ureter crosses below the uterine artery (water under the bridge) approximately 1.5–2 cm lateral to the cervix. Before applying the clamp to ligate the uterine artery, the surgeon must identify the ureter and displace it laterally to prevent inadvertent ureteric ligation or transection — the most feared complication of hysterectomy. The other structures are not at immediate risk at this specific step.
Gynaecological Laparotomy — What You Observe
A gynaecological laparotomy follows a systematic structure that the observer should be able to track from the moment the abdomen is opened. Whether exploratory or operative, the procedure has a logical sequence that the surgeon follows and that the informed observer can anticipate.
Abdominal entry. The most common incisions in gynaecological laparotomy are the midline vertical incision (xiphisternum to pubis or limited lower midline) and the Pfannenstiel transverse incision. The choice depends on the urgency, the size of the pathology, and whether upper-abdominal access may be needed. A large fibroid uterus or an ovarian mass of uncertain size typically requires a midline incision. Elective benign cases frequently use a Pfannenstiel incision for cosmetic and wound-strength advantages.
Systematic pelvic exploration. Once the abdomen is open, a self-retaining retractor (Balfour or O'Connor-O'Sullivan) is placed. The surgeon begins with a systematic inspection of the pelvic organs: the uterus (size, shape, surface fibroids), both ovaries and fallopian tubes, the posterior cul-de-sac (pouch of Douglas) for adhesions or endometriotic deposits, and the posterior surface of the uterus. In emergency laparotomy for suspected ectopic pregnancy, the surgeon will first look for blood in the pelvis (haemoperitoneum), identify the fallopian tubes bilaterally, and locate the affected tube. Watch how the surgeon uses a combination of direct vision and palpation to systematically map the pathology before beginning any resection.
Operative laparotomy decisions observed. If a fibroid is to be removed by myomectomy, the observer watches the surgeon inject dilute vasopressin into the myometrium (to reduce bleeding), make an elliptical incision over the fibroid, and enucleate it bluntly from its pseudocapsule. For an ovarian cystectomy, the surgeon incises the ovarian cortex over the cyst, dissects the cyst wall from the surrounding ovarian tissue using sharp and blunt dissection, and closes the ovary with interrupted absorbable sutures. In any operative laparotomy, note the haemostasis techniques used — clips, bipolar diathermy, suture ligation — and identify whether any drains are placed at the end.
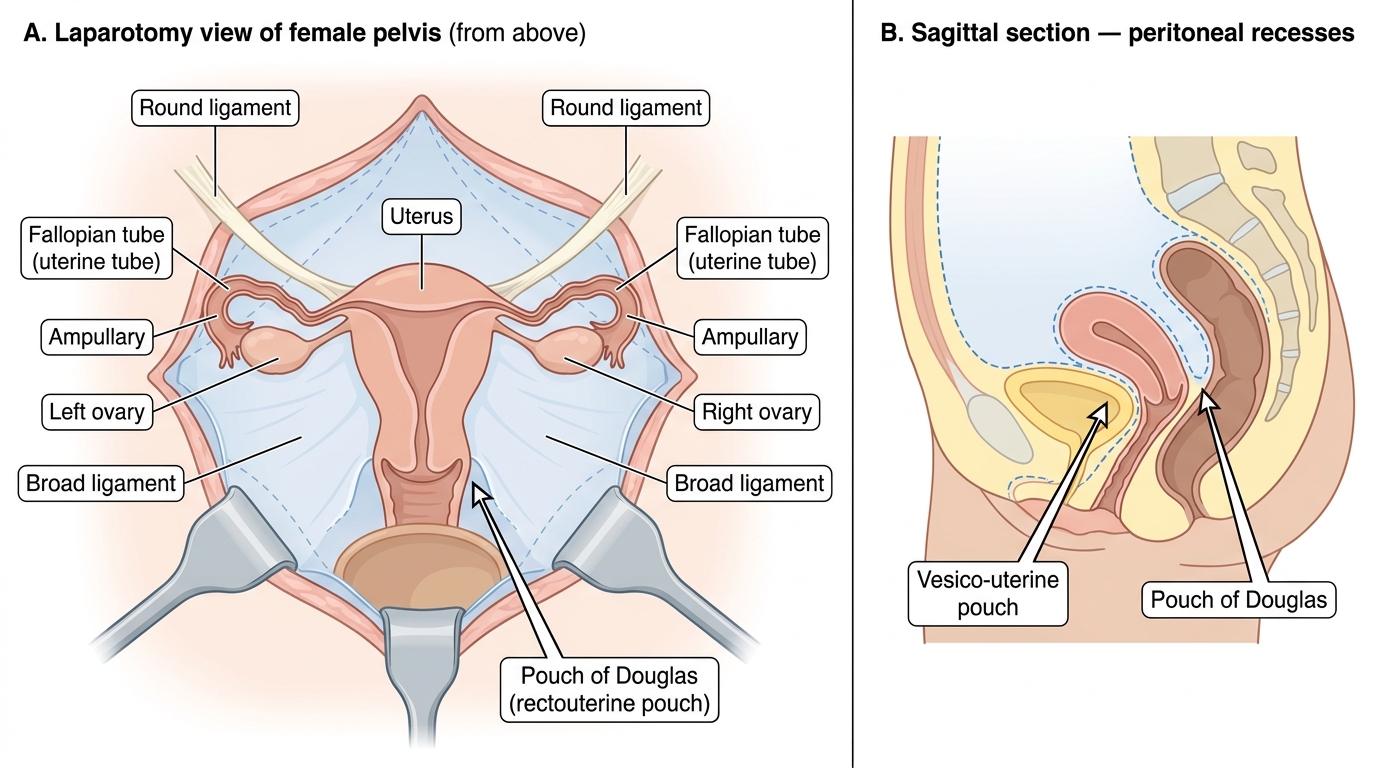
Pelvic Cavity as Seen Through a Laparotomy Incision