Page 23 of 29
OG7.1 | Maternal Physiological Changes in Pregnancy — SDL Guide (Part 4)
Self-Assessment and Consolidation
Maternal physiological changes in pregnancy span every organ system and create a clinically distinct physiological state that must be treated as its own reference population. The following key principles consolidate the module content for application:
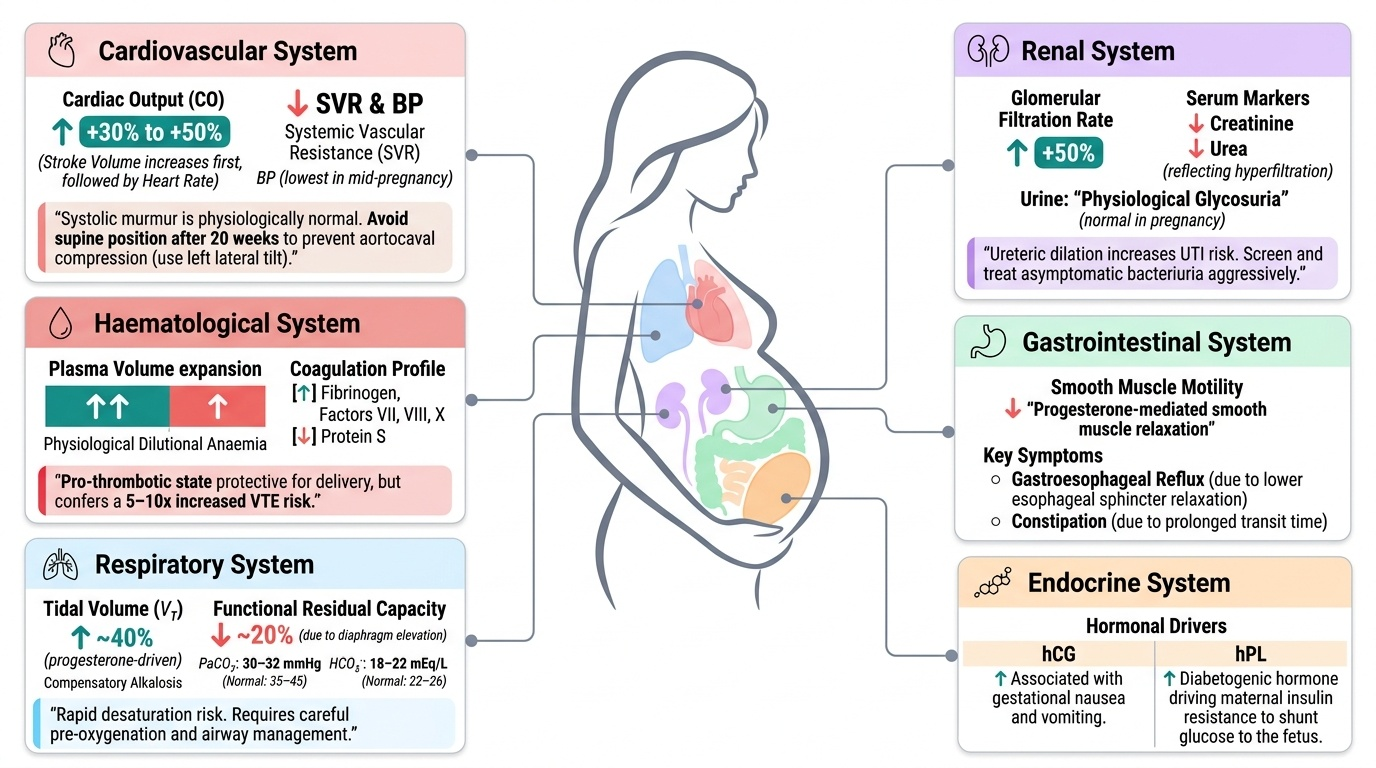
The cardiovascular system expands to deliver high-flow, low-resistance perfusion to the uteroplacental unit. Cardiac output rises 30–50% (stroke volume first, then heart rate); SVR falls; blood pressure drops physiologically in mid-pregnancy. A systolic murmur is expected. Aortocaval compression in the supine position after 20 weeks can reduce CO and cause fetal distress — use left lateral tilt.
The haematological system expands plasma volume more than red cell mass, producing physiological dilutional anaemia. The coagulation system becomes pro-thrombotic (↑fibrinogen, ↑factors VII/VIII/X, ↓protein S) — protective for delivery but conferring a 5–10-fold VTE risk.
The respiratory system increases tidal volume by ~40% (progesterone-driven), reduces FRC by ~20% (uterine diaphragm elevation), and maintains a state of compensated respiratory alkalosis (PaCO₂ ~30–32 mmHg, HCO₃⁻ ~18–22 mEq/L). Rapid desaturation risk necessitates careful anaesthetic management.
The renal system hyperfiltrates (GFR +50%), producing lower creatinine, lower urea, and physiological glycosuria. Ureteric dilation increases UTI risk — screen and treat asymptomatic bacteriuria.
The GI and endocrine systems are dominated by progesterone (smooth muscle relaxation → reflux + constipation), hCG (nausea/vomiting), and hPL (insulin resistance → GDM risk). Thyroid binding globulin rises, elevating total T₄ but not free T₄. Weight gain of 11.5–16 kg is appropriate for normal-BMI women.
The hormonal drivers form a coherent framework: progesterone (smooth muscle relaxation, respiratory stimulation, uterine quiescence), oestrogen (vascular growth, coagulation factor synthesis, uterine hypertrophy), hCG (corpus luteum maintenance, nausea), hPL (insulin resistance, fetal nutrient diversion), relaxin (joint laxity, renal vasodilation), and aldosterone (volume expansion).
Knowing what is normal in pregnancy — and at which gestational age — is the foundation of safe obstetric practice. The next module on antenatal care (OG8) directly applies these physiological baselines to screening and supplementation decisions.
Provided image
SELF-CHECK
A 32-year-old woman at 32 weeks gestation is found to have a serum creatinine of 0.85 mg/dL. The laboratory report flags this as normal (reference range 0.6–1.1 mg/dL). Which statement is most accurate?
A. This is truly normal — the lab reference range confirms it
B. This is borderline — repeat in 2 weeks
C. This is significantly elevated for pregnancy — GFR is likely impaired and warrants renal assessment
D. This is a laboratory error — creatinine cannot be this high in pregnancy
Reveal Answer
Answer: C. This is significantly elevated for pregnancy — GFR is likely impaired and warrants renal assessment
Standard laboratory reference ranges are calibrated to non-pregnant adults. In pregnancy, GFR increases ~50%, so serum creatinine should fall to 0.4–0.6 mg/dL. A value of 0.85 mg/dL — unremarkable by non-pregnant standards — represents significant GFR impairment in a pregnant woman and warrants evaluation for pre-eclampsia with renal involvement, underlying renal disease, or other pathology.