Page 1 of 30
OG8.1 | Antenatal Care Objectives and Risk Screening — SDL Guide
Learning Objectives
- Enumerate the objectives of antenatal care and explain how each objective reduces maternal and perinatal mortality
- Describe the WHO 2016 eight-contact ANC model and the minimum India MOHFW schedule, including the content of each visit
- Screen for high-risk factors in pregnancy using accepted obstetric, medical and social criteria
- Explain the concept of the inverted pyramid of care and apply it to justify risk-stratified referral decisions
- Counsel a pregnant woman on IFA supplementation, calcium supplementation, Td immunisation and danger signs
INSTRUCTIONS
Antenatal care (ANC) is the organised health-care delivered to a pregnant woman from conception to the onset of labour. Systematic ANC is India's single most powerful lever for reducing the 103 maternal deaths per 100,000 live births (SRS 2018–20) and the 28 neonatal deaths per 1,000 live births that persist despite significant progress. This module builds the cognitive and procedural scaffold you need to conduct structured ANC visits, identify pregnancies that are deviating from the normal trajectory, and match the level of care to the level of risk — the essence of the inverted pyramid of care.
References
- DC Dutta's Textbook of Obstetrics, 9th ed., Ch. 7 — Antenatal Care (textbook)
- Williams Obstetrics, 26th ed., Ch. 9 — Prenatal Care (textbook)
- WHO Recommendations on Antenatal Care for a Positive Pregnancy Experience, 2016 (guideline)
- MOHFW India, Operational Guidelines on Maternal and Newborn Health, 2022 (guideline)
- FOGSI Good Clinical Practice Recommendations — Antenatal Care, 2021 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Priya, a 22-year-old primigravida from a rural district in Rajasthan, presents to your peripheral health centre at 32 weeks of gestation. She has had no formal antenatal visit since her first trimester urine pregnancy test confirmed the pregnancy. Today her blood pressure reads 158/104 mmHg, she has 2+ proteinuria on dipstick, and she complains of a severe headache for the past two days. Her haemoglobin, checked for the first time today, is 7.2 g/dL. There is no record of Td immunisation, she has not received any iron-folic acid tablets, and she is unaware of fetal movement patterns. You are looking at a woman in whom severe pre-eclampsia and severe anaemia have developed silently — both potentially preventable with structured ANC. How many opportunities to detect this trajectory were missed, and what would a systematic antenatal surveillance programme have detected?
WHY THIS MATTERS
Antenatal care is the domain where preventive obstetrics and clinical medicine converge. As a final-year medical student and future clinician, you will conduct ANC in community postings, primary health centres, and district hospitals. The ability to enumerate ANC objectives, apply the visit schedule, screen for high-risk factors, and deploy the inverted pyramid framework is directly assessed in MBBS Professional examinations under competency OG8.1 (KH level — knowledge and how). More immediately, a well-conducted ANC contact can detect pre-eclampsia, severe anaemia, malpresentation, diabetes and IUGR weeks before they become emergencies — making this a life-saving clinical skill, not an administrative task.
RECALL
Before engaging with the ANC framework, bring to mind these foundations. From reproductive physiology (OG6): plasma volume expands by 40–50% in pregnancy, cardiac output rises by 30–40%, and glomerular filtration rate increases by 50% — these physiological changes underlie why normal pregnancy BP is lower than non-pregnant values and why proteinuria thresholds differ from the non-pregnant adult. From pregnancy diagnosis (OG7): gestational age is estimated by last menstrual period (LMP) using Naegele's rule (add 9 calendar months + 7 days, or add 1 year, subtract 3 months, add 7 days) and confirmed by first-trimester ultrasound (crown-rump length most accurate ≤13 weeks + 6 days). The expected date of delivery (EDD) and gestational age at any visit are foundational to knowing what the ANC visit schedule should include.
Why Antenatal Care Matters: The Clinical Case for Structured Surveillance
Antenatal care is a package of health-care interventions provided to a pregnant woman during gestation, with the dual purpose of promoting maternal and fetal wellbeing and detecting complications early enough to prevent morbidity and mortality. The case for structured ANC is built on epidemiological reality: in India, haemorrhage, hypertensive disorders and sepsis account for over 60% of maternal deaths, and the majority of these deaths are preventable when the underlying conditions are detected and managed before the acute event. The global Sustainable Development Goal (SDG) target 3.1 calls for a maternal mortality ratio (MMR) ≤70 per 100,000 live births by 2030; India's current MMR of approximately 103 (SRS 2018–20) means that ANC quality is a direct contributor to whether this target is met.
The formal objectives of ANC can be grouped into five domains, each addressing a distinct mechanism by which pregnancy outcomes are improved:
- To date the pregnancy accurately — establishing the gestational age at booking enables all subsequent assessments to be interpreted against the correct reference range, identifies post-term pregnancies requiring surveillance, and determines the optimal timing for anomaly screening.
- To screen for and manage complications — systematic recording of blood pressure, weight gain, urine protein, haemoglobin, blood group and indirect Coombs test, blood sugar (DIPSI/IADPSG), and STI screening (VDRL, HIV) allows early identification and treatment of pre-eclampsia, anaemia, gestational diabetes, isoimmunisation and congenital infection.
- To promote maternal nutrition and prevent deficiency states — iron-deficiency anaemia (Hb <11 g/dL) is present in ~45% of pregnant Indian women at delivery; daily IFA supplementation (60 mg elemental iron + 500 µg folic acid) and calcium supplementation (1.5–2 g/day for pre-eclampsia prevention in low-intake populations) are among the highest-yield preventive interventions globally.
- To provide immunoprotection — tetanus immunisation via Td schedule protects both mother and neonate from tetanus neonatorum, which remains a cause of preventable neonatal death in areas with low vaccination coverage.
- To prepare for childbirth and emergencies — birth preparedness counselling (identifying a skilled birth attendant, transport plan, blood donor, savings), danger sign education, and registration of the pregnancy in the health system all reduce the 'three delays' (decision, reaching facility, receiving care) that contribute to preventable maternal death.
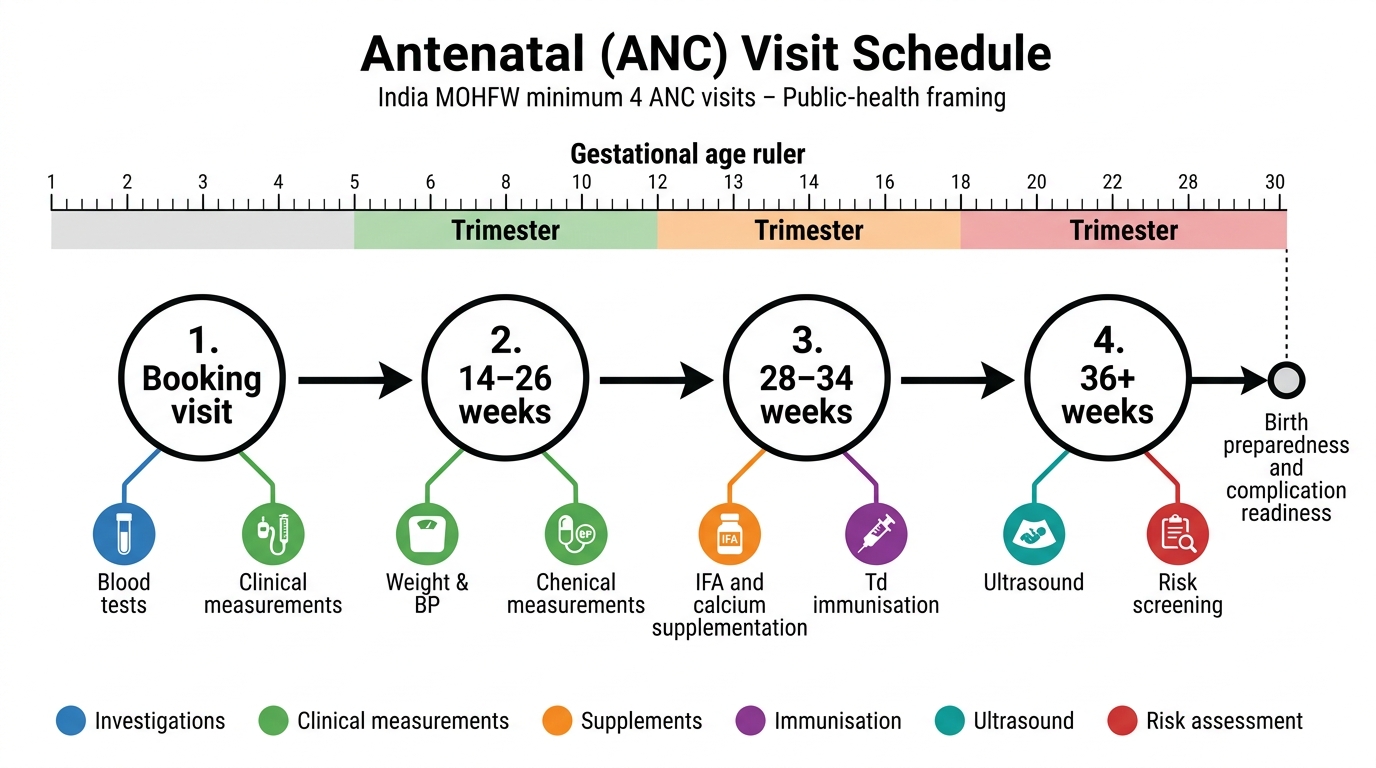
India MOHFW Minimum ANC Visit Schedule
ANC is therefore not a series of checkups but a structured clinical risk-management process embedded in a public health system. The five objectives above map directly to the content of each ANC visit and explain why every element of the visit exists.
SELF-CHECK
Which of the following best describes the primary purpose of the first ANC booking visit?
A. To prescribe iron tablets and give the first Td injection
B. To accurately date the pregnancy, establish a baseline, screen for risk factors and register the woman in the ANC system
C. To perform a detailed abdominal examination and document fundal height
D. To screen for gestational diabetes using DIPSI
Reveal Answer
Answer: B. To accurately date the pregnancy, establish a baseline, screen for risk factors and register the woman in the ANC system
The booking visit serves multiple objectives simultaneously: accurate gestational dating (LMP + first-trimester USG), baseline investigations (blood group, Hb, VDRL, HIV, urine), risk factor identification, and formal registration. IFA and Td are initiated at booking but are interventions, not the primary purpose. DIPSI screening is typically performed in the second trimester (24–28 weeks), not at the booking visit.
Governing Principles: Physiology of Pregnancy and the Inverted Pyramid
ANC surveillance is predicated on understanding which physiological parameters change in normal pregnancy, at what gestational age they change, and why deviations from normal carry clinical significance. This section articulates the governing principles that make each ANC assessment meaningful rather than ritualistic.
The haemodynamic changes of normal pregnancy — a 40–50% rise in plasma volume that exceeds the 20–30% rise in red cell mass, creating the physiological anaemia of pregnancy — mean that a haemoglobin of 10–11 g/dL in the second trimester may be normal, whereas the same value in a non-pregnant woman would be mildly anaemic. Distinguishing physiological haemodilution from true iron-deficiency anaemia (Hb <11 g/dL by WHO criteria in pregnancy) requires knowledge of this trajectory. Similarly, gestational hypertension and pre-eclampsia are defined relative to the expected fall in blood pressure during the first and second trimesters (BP typically reaches its nadir at 20–24 weeks); a BP of 140/90 mmHg after 20 weeks is abnormal precisely because it exceeds the normal gestational range.
The inverted pyramid of care is the conceptual framework that structures ANC delivery in a resource-limited health system. It recognises three epidemiological truths: (1) the majority of pregnancies (~70–80%) will be uncomplicated and require only basic surveillance; (2) a minority (~20–30%) will develop complications requiring additional investigation or specialist care; and (3) a very small proportion (<5%) will require intensive or tertiary-level management. The pyramid is 'inverted' because care should be initiated at the widest, most accessible level (community/subcentre/PHC) for all women, with the population narrowing at each successive tier as risk stratification filters those who need escalated care upward.
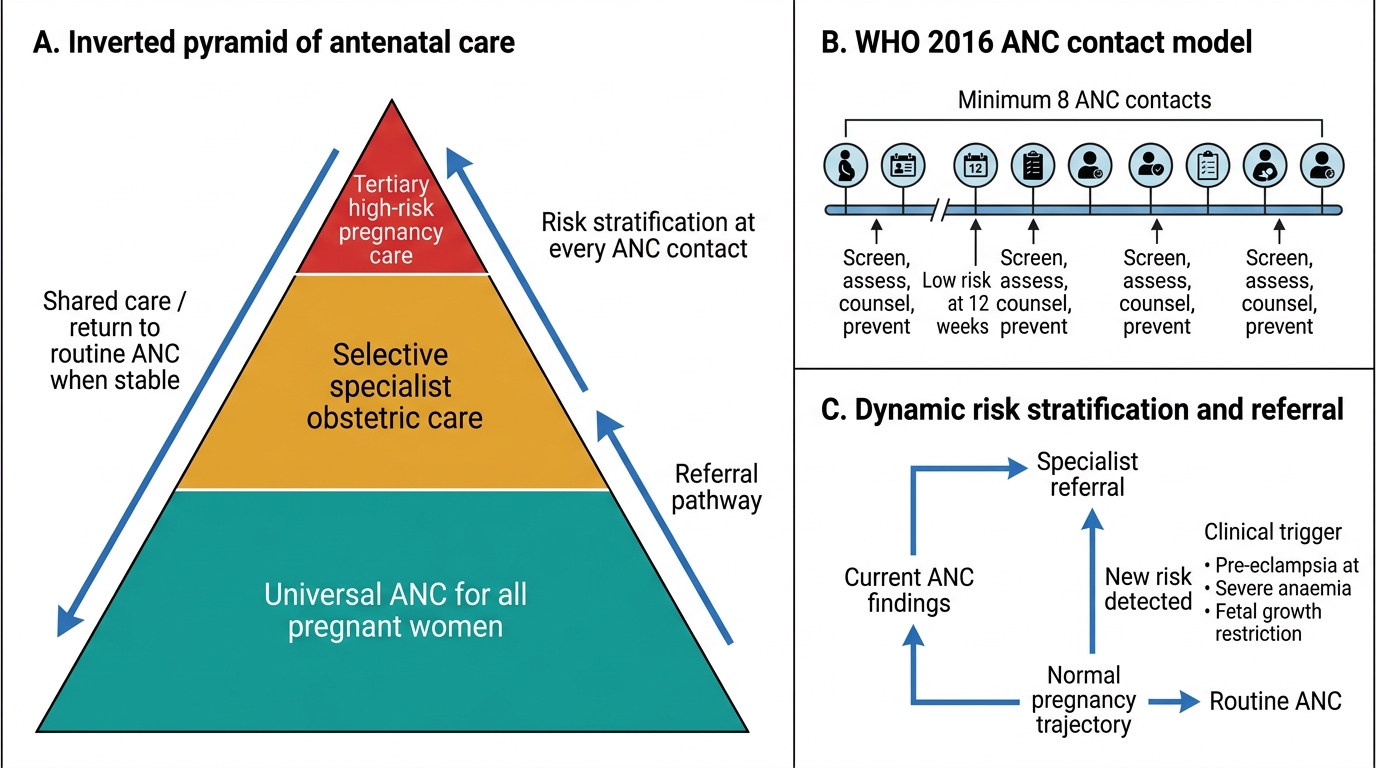
Inverted Pyramid of Antenatal Care
The practical implication is that a risk-stratification screen at every ANC visit determines whether the current visit's findings are consistent with normal pregnancy or indicate a trajectory that requires a higher level of care. This is not a one-time classification at booking; it is a dynamic process, because a woman who is low-risk at 12 weeks may develop pre-eclampsia at 32 weeks.
The ANC Visit Protocol: Schedule, Content and Screening Interventions
The WHO 2016 model of antenatal care recommends a minimum of 8 contacts between a pregnant woman and the health system, replacing the older 4-visit focused ANC model. The shift from 4 to 8 was driven by a systematic review demonstrating that perinatal mortality is significantly reduced with more frequent contacts (RR 0.90, 95% CI 0.83–0.96 from the WHO ANC trial network); the term 'contact' was chosen deliberately over 'visit' to emphasise that meaningful clinical interaction — not mere attendance — is the goal. Each contact must include a minimum set of clinical assessments, preventive interventions, and counselling elements that are standardised by evidence-based guidelines, yet adapted to the gestational age and the findings of the individual woman. This standardisation is what converts a series of individual visits into a coherent surveillance programme capable of detecting and responding to the most common complications of pregnancy at the optimal gestational window for intervention.
Under the India MOHFW framework, the minimum recommended schedule aligns with ANC1–ANC4 at the following gestational ages, with each visit having specific objectives:
| Contact | Gestational Age | Key Assessments | Key Interventions |
|---|---|---|---|
| ANC1 (Booking) | As early as possible (ideally <12 weeks) | Confirm pregnancy, dating USG, BP, weight, Hb, blood group, Rh, VDRL, HIV, urine routine | Register, start IFA (60 mg iron + 500 µg folic acid daily), calcium 500 mg BD, Td1 |
| ANC2 | 14–26 weeks | BP, weight, urine protein, fundal height, fetal heart | Anomaly USG (18–20 weeks), DIPSI/GDM screen (24–28 weeks), second IFA packet |
| ANC3 | 28–34 weeks | BP, oedema, fundal height, abdominal girth, fetal lie/presentation, NST if indicated | Td2 (≥4 weeks after Td1), iron supplementation review, birth preparedness counselling |
| ANC4 | 36 weeks onward | Leopold's manoeuvres, engagement of presenting part, pelvic adequacy, fetal wellbeing | Confirm delivery plan, referral if high-risk, postpartum counselling |
Critical supplementation and immunisation details that are examination essentials:
- IFA: 60 mg elemental iron + 500 µg folic acid per tablet, one tablet daily throughout pregnancy and for 100 days postpartum; administered under the national IFA supplementation programme.
- Calcium: 1.5–2 g elemental calcium per day (typically 500 mg three times daily) from 20 weeks onward for women with low dietary calcium intake, as per WHO 2016 recommendation for pre-eclampsia prevention.
- Td schedule: Td1 at first ANC contact; Td2 at least 4 weeks later (ideally by 36 weeks); in previously immunised women (last Td within 3 years), a single booster is adequate. Neonatal tetanus prophylaxis is the primary goal.
The visit schedule is not merely a checklist — each item has an evidence base and a gestational rationale. The timing of the anomaly ultrasound (18–20 weeks) is chosen because organ structures are sufficiently developed for detailed assessment while the pregnancy is at a stage where management decisions remain clinically feasible.
SELF-CHECK
According to the WHO 2016 ANC model, what is the minimum recommended number of antenatal contacts?
A. 4 contacts
B. 6 contacts
C. 8 contacts
D. 10 contacts
Reveal Answer
Answer: C. 8 contacts
The WHO 2016 model recommends a minimum of 8 contacts, replacing the older 4-visit focused ANC model. The change was driven by evidence that perinatal mortality is significantly reduced with more frequent, meaningful contacts. India's MOHFW minimum is 4 visits (ANC1–ANC4) as a practical floor, but the aspirational target aligns with the 8-contact WHO recommendation.