Page 12 of 30
OG8.5 | Pelvic Assessment and CPD Evaluation — SDL Guide
Learning Objectives
- State the clinical indications for pelvic assessment in antenatal care and in labour (OG8.5)
- Describe the four Caldwell-Moloy pelvic types and identify their characteristic features and obstetric implications
- Enumerate the key obstetric diameters of the pelvic inlet, cavity, and outlet with their normal thresholds
- Demonstrate the technique of clinical pelvimetry on a model — including measurement of the diagonal conjugate, bi-ischial diameter, and sub-pubic angle assessment
- Derive the obstetric conjugate from the diagonal conjugate and interpret measurements to assess pelvic adequacy
- Describe the management of suspected or confirmed cephalopelvic disproportion (CPD), including criteria for trial of labour versus elective caesarean section
INSTRUCTIONS
Cephalopelvic disproportion (CPD) — the mismatch between the size of the fetal presenting part and the dimensions of the maternal pelvis — is a direct cause of obstructed labour, one of the five major contributors to maternal mortality globally. Recognising a contracted pelvis or suspected CPD before or early in labour, and making the correct management decision, prevents maternal and fetal morbidity. Competency OG8.5 (SH level) requires you to demonstrate pelvimetry on a model — a skill that combines anatomical knowledge, procedural competence, and clinical interpretation. This module prepares you for DOAP assessments and for the reality of obstetric emergencies in district hospitals.
References
- DC Dutta's Textbook of Obstetrics, 9th ed., Ch. 5 — The Female Pelvis; Ch. 34 — Obstructed Labour (textbook)
- Williams Obstetrics, 26th ed., Ch. 2 — Maternal Anatomy; Ch. 23 — Abnormal Labour (textbook)
- Jeffcoate's Principles of Gynaecology, 8th ed. — Chapter on Pelvic Anatomy (textbook)
- FOGSI Good Clinical Practice — Obstructed Labour Management, 2021 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 19-year-old primigravida, Sumathi, is admitted at full term in active labour. Her height is 142 cm. Her antenatal card shows no record of pelvic assessment at her last ANC visit. After 18 hours of active labour, she has reached full dilatation but the fetal head has not descended despite strong uterine contractions. The fetal head is 4/5 palpable abdominally; vaginal examination shows the head is deeply moulded and there is no further descent despite maternal expulsive effort. The obstetrician diagnoses obstructed labour secondary to cephalopelvic disproportion. An emergency caesarean section is performed; both mother and baby survive, but Sumathi has developed a vesicovaginal fistula that will require complex repair. This outcome was not inevitable. A pelvic assessment at 36 weeks — recording Sumathi's height, estimating the pelvic dimensions, and noting that her diagonal conjugate was 9.5 cm — would have identified her as high-risk for CPD and planned an elective caesarean section before obstructed labour developed.
WHY THIS MATTERS
Pelvic assessment and CPD evaluation (OG8.5, SH level) is a skills competency assessed in DOAP stations and bedside examinations using an obstetric pelvic model. But its clinical importance extends far beyond examination performance: obstructed labour from unrecognised CPD is a leading cause of maternal mortality in low-income settings and a major cause of obstetric fistula — a condition that can permanently alter a woman's quality of life. India's incidence of obstructed labour correlates directly with the proportion of deliveries occurring without skilled birth attendance and without antenatal pelvic assessment. As a future clinician practicing in a wide range of settings, your ability to perform and interpret clinical pelvimetry is a skill that directly prevents harm — not a theoretical exercise.
RECALL
From anatomy: the bony pelvis consists of two innominate bones (ilium, ischium, pubis fused at the triradiate cartilage), the sacrum, and the coccyx. The pelvic inlet (brim) is bounded by the sacral promontory posteriorly, the iliopectineal lines laterally, and the upper border of the pubic symphysis anteriorly. The pelvic outlet is bounded by the lower border of the pubic symphysis anteriorly, the ischial tuberosities laterally, and the tip of the sacrum/coccyx posteriorly. The pelvic cavity is the space between the inlet and the outlet. From obstetric physiology: the presenting part of the fetus must traverse the inlet, navigate the cavity, and pass through the outlet — and at each level, specific diameters are the limiting dimensions. The three P's of labour — passenger (fetus), passage (pelvis), and powers (uterine contractions) — must all be adequate; CPD represents failure of the first two P's to be compatible.
When and Why Pelvic Assessment Matters in Obstetric Care
Cephalopelvic disproportion (CPD) is the condition in which the presenting fetal part (usually the cephalic vertex) is too large, or oriented in an unfavourable attitude, to pass through the bony pelvis without causing obstruction. CPD may be absolute (the head physically cannot pass through even with optimal uterine contractions) or relative (with very strong contractions and favourable fetal head moulding, passage is possible but at the cost of significant risk to mother and fetus). Distinguishing absolute from relative CPD, and predicting which women will have it before labour becomes obstructed, is the clinical problem that pelvic assessment attempts to solve.
The clinical indications for pelvic assessment arise at two time points:
Antenatal pelvic assessment (≥36 weeks): All women, particularly those at increased risk of CPD, should have their pelvic dimensions assessed at the final ANC visit or at 36–38 weeks. High-risk indicators that mandate especially careful pelvic assessment:
- Height <150 cm (short stature is a surrogate for small pelvic dimensions; the cut-off is <145 cm in some guidelines, and <150 cm in others — both warrant assessment)
- Previous obstructed labour or caesarean section for CPD/failure to progress
- Primigravida with non-engagement of the fetal head at term
- Suspected macrosomia (EFW >4 kg)
- Rickets, osteomalacia, pelvic fractures, or spinal deformity in the history
- Fetal macrosomia in a diabetic pregnancy
Intrapartum assessment: Pelvimetry (or re-assessment of pelvic dimensions) is indicated when labour is not progressing at the expected rate despite adequate uterine contractions — poor progress in the active phase of labour (cervical dilatation <1 cm/hour after 4 cm in active labour) may reflect CPD, malposition, or insufficient uterine activity, and pelvic assessment contributes to distinguishing these causes.
The historical importance of pelvic assessment lies in its role as the primary preventive tool against obstructed labour, which — before the era of safe caesarean section — was the leading cause of maternal death and the primary cause of obstetric vesicovaginal and rectovaginal fistulae.
Pelvic Anatomy and Governing Principles of Pelvic Adequacy
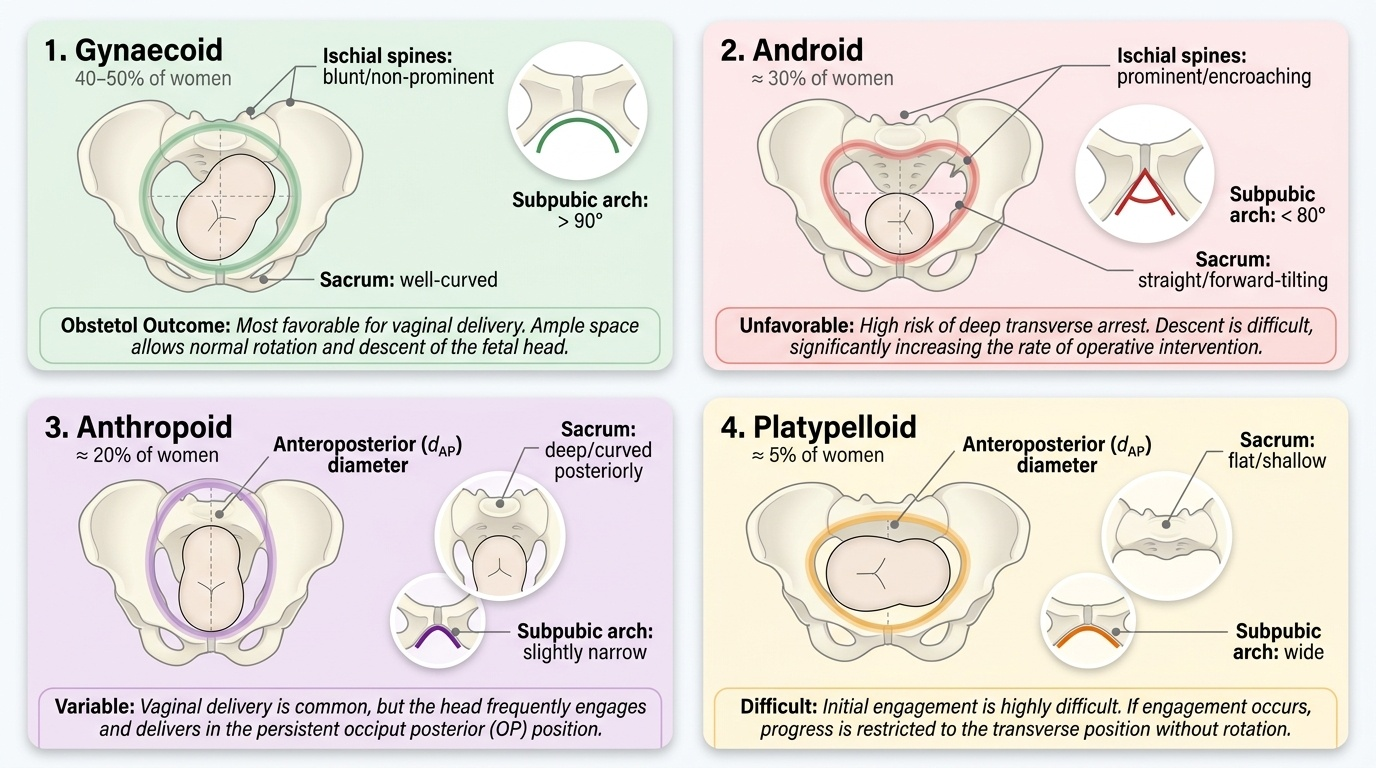
The Caldwell-Moloy classification (1933) describes four fundamental pelvic types based on the shape of the pelvic inlet, with implications for the expected mechanism of labour and the probability of vaginal delivery:
1. Gynaecoid pelvis (40–50% of women): Rounded or slightly oval inlet; well-curved sacrum; wide subpubic arch (>90°); ischial spines not prominent. This is the most favourable pelvic type for vaginal delivery — the round inlet accommodates the fetal head well in the transverse diameter, and the wide outlet facilitates delivery. The standard 'normal female pelvis.'
2. Android pelvis (~30% of women): Heart-shaped or wedge-shaped inlet (narrowest posteriorly); straight sacrum; narrow subpubic arch (<80°); prominent ischial spines narrowing the midplane. This is the least favourable for vaginal delivery — the narrow posterior segment forces the fetal head into the anterior segment; the narrow midplane and outlet make descent difficult. Associated with deep transverse arrest in labour.
3. Anthropoid pelvis (~20% of women): Long oval inlet with anteroposterior diameter greater than the transverse; deep sacrum; narrow subpubic arch. Vaginal delivery is possible but the head tends to engage and deliver in the occiput posterior (OP) or occiput anterior (OA) position — a 'persistent OP' or OP delivery may result.
4. Platypelloid pelvis (<5% of women): Flat, kidney-shaped inlet with wide transverse diameter and short anteroposterior diameter; shallow sacrum; wide subpubic arch. Engagement is difficult because the inlet AP diameter is too small; when engagement occurs the head must enter in the transverse diameter and cannot rotate easily.
Provided image
The key obstetric diameters at each level of the pelvis determine which pelvic type will or will not accommodate a term fetal head (average BPD 9.5 cm, SOF diameter 9.5 cm):
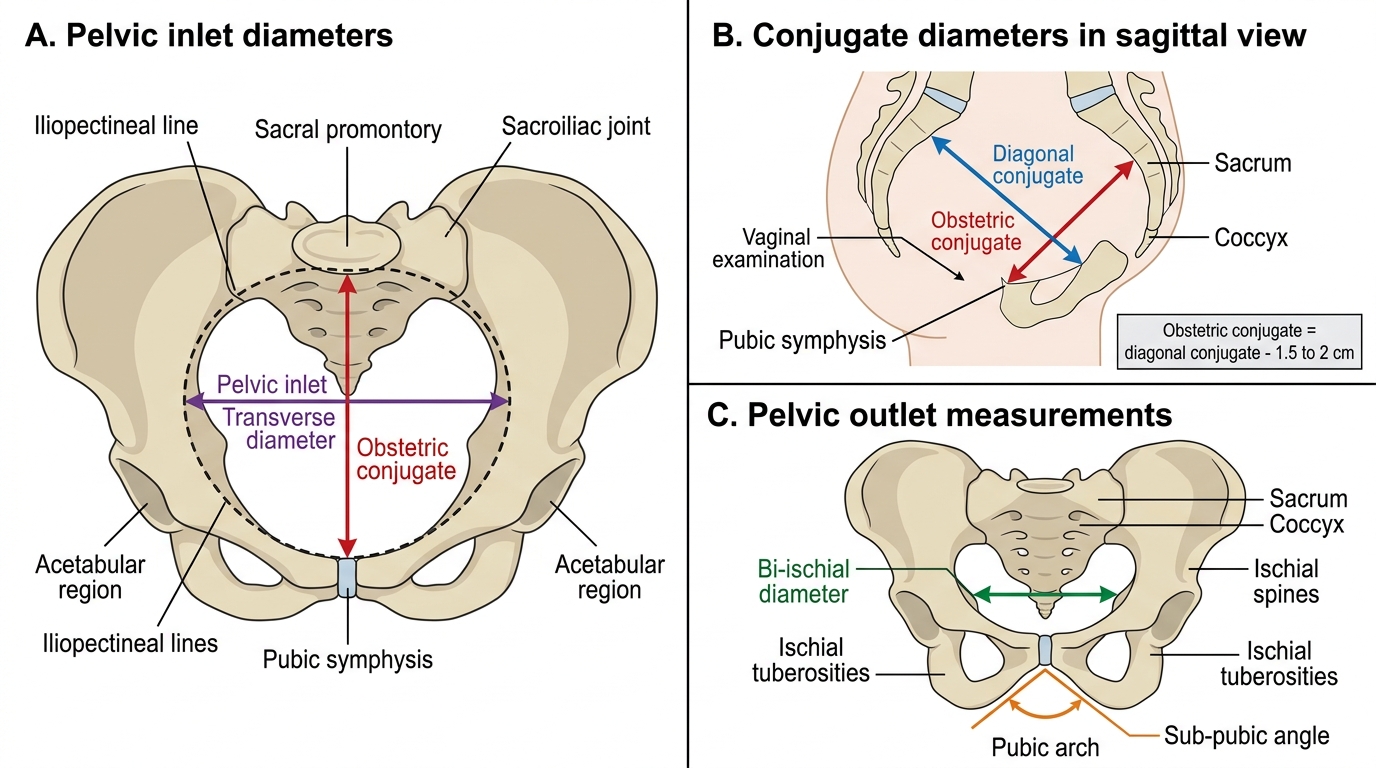
Pelvic inlet diameters:
- Obstetric conjugate (true conjugate): from sacral promontory to the inner surface of the pubic symphysis — the shortest AP diameter the fetal head must pass; normal ≥10 cm; cannot be measured directly (sacral promontory unreachable by finger in a normal pelvis). Derived from diagonal conjugate by subtracting 1.5–2 cm.
- Diagonal conjugate: from sacral promontory to the lower border (inferior margin) of the pubic symphysis; the only clinically measurable AP inlet diameter; normal ≥12.5 cm. Measured by vaginal examination.
- Transverse diameter of inlet: widest transverse dimension of the inlet; normal ≥13 cm; estimated clinically or measured radiologically.
Pelvic cavity diameters (midplane):
- Bispinous diameter (interspinous diameter): distance between the ischial spines; normal ≥10 cm; the most important midplane diameter; narrowed in android pelvis; assessed clinically by palpating ischial spines.
Pelvic outlet diameters:
- Bi-ischial diameter (bi-tuberous / intertuberous): distance between the ischial tuberosities; normal ≥8 cm; measured with a closed fist or Thoms pelvimeter placed between the tuberosities.
- Subpubic angle: normally >90° (two fingers width below the symphysis); narrow subpubic angle (<85°) forces the fetal head away from the pubic arch, reducing the effective outlet.
Key Obstetric Diameters of the Female Bony Pelvis
SELF-CHECK
A clinician measures a diagonal conjugate of 11 cm during pelvic assessment. What is the estimated obstetric conjugate, and what is the clinical significance?
A. Obstetric conjugate ≈ 12.5–13 cm; this is normal
B. Obstetric conjugate ≈ 9–9.5 cm; this is below the 10 cm threshold for a contracted pelvis
C. Obstetric conjugate = 11 cm; this equals the diagonal conjugate
D. Obstetric conjugate ≈ 11 cm; this is normal as the threshold is 10 cm
Reveal Answer
Answer: B. Obstetric conjugate ≈ 9–9.5 cm; this is below the 10 cm threshold for a contracted pelvis
The obstetric conjugate is derived from the diagonal conjugate by subtracting 1.5–2 cm. Diagonal conjugate 11 cm minus 1.5–2 cm = obstetric conjugate 9–9.5 cm. The threshold for a contracted pelvis (inlet) is obstetric conjugate <10 cm. Therefore, an obstetric conjugate of 9–9.5 cm indicates a contracted inlet, and this woman is at risk for CPD with a term-sized fetus. Management options include trial of labour with close monitoring or elective caesarean section depending on other factors (estimated fetal weight, pelvic type, previous obstetric history).
Technique of Clinical Pelvimetry on a Model
Clinical pelvimetry is performed on an obstetric pelvic model as the primary teaching tool, as well as on patients in the late third trimester (≥36 weeks) as part of the clinical assessment. The technique requires a systematic approach to assess each level of the pelvis in turn: inlet, midplane, and outlet. Before beginning, ensure the patient (or model) is positioned in the dorsal lithotomy position (Sims' position for supine pelvimetry), bladder empty, and that the examiner explains each step clearly. In clinical practice, pelvimetry is performed as part of a vaginal examination and requires valid consent.
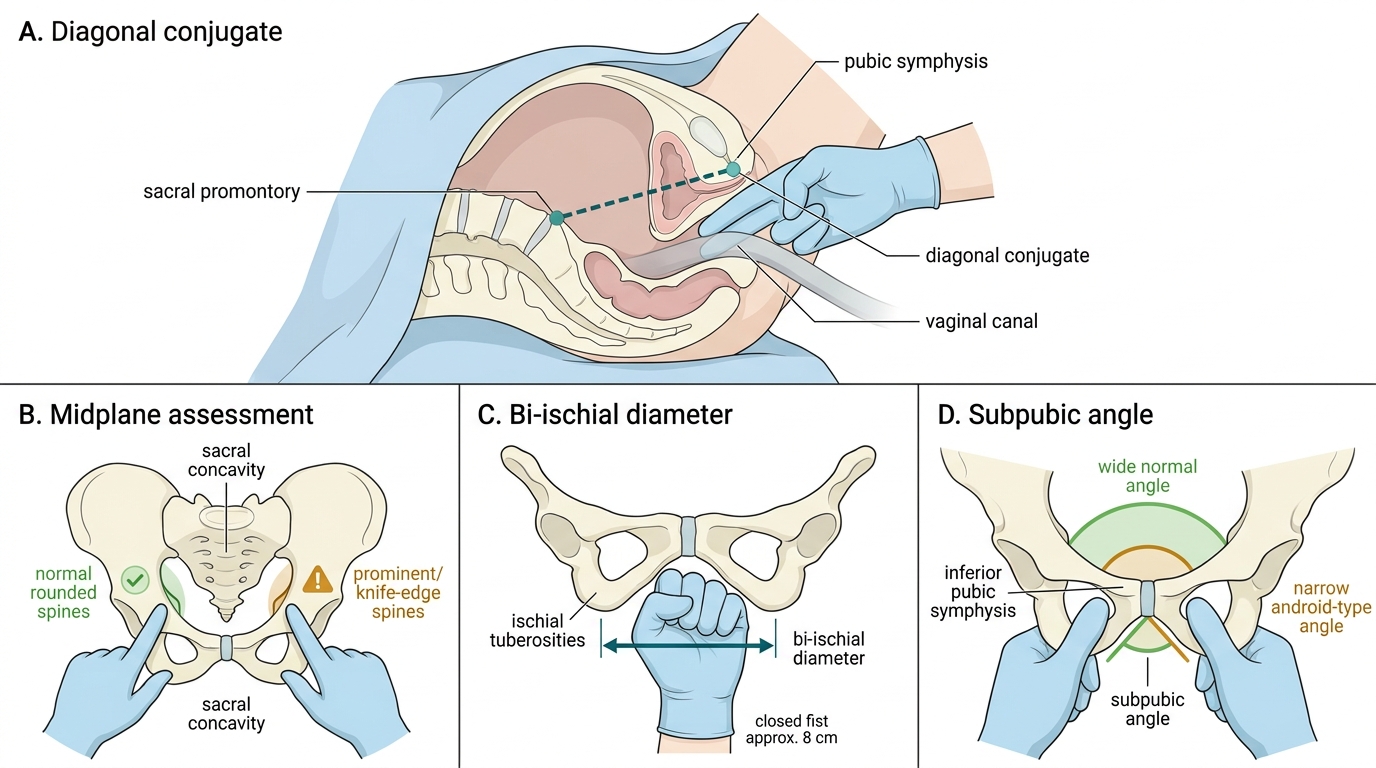
Step 1 — Measurement of the diagonal conjugate:
Insert the right index and middle fingers into the vagina, keeping the wrist below the level of the perineum. Advance the fingers along the posterior vaginal wall until the middle finger touches the sacral promontory. Bring the index finger of the left hand to mark the point where the examining right hand contacts the inferior border of the pubic symphysis. Withdraw the fingers and measure the distance from the tip of the right middle finger to the marked point on the right hand using a ruler. This measured distance is the diagonal conjugate (DC). Normal DC ≥12.5 cm. If the sacral promontory cannot be reached with the examining finger, the DC is estimated as >12.5 cm (suggesting an adequate inlet).
Clinical Pelvimetry Technique
Step 2 — Assessment of the midplane:
With the fingers still in the vaginal canal (or re-inserted), sweep the fingers laterally to palpate the ischial spines. Note whether they are:
- Not prominent (normal): do not project significantly into the cavity — bispinous diameter estimated ≥10 cm
- Slightly prominent: suggestive of android or anthropoid pelvis; borderline
- Markedly prominent / knife-edge: encroaching significantly on the midplane — bispinous diameter likely <10 cm; high risk of deep transverse arrest in labour
Also assess the sacral concavity: a deeply curved (concave) sacrum provides more posterior space; a straight or forward-projecting sacrum reduces the available outlet space.
Step 3 — Measurement of the bi-ischial (intertuberous) diameter:
With the woman in lithotomy position, place a closed fist (knuckles against the perineum) between the two ischial tuberosities. A standard closed fist measures approximately 8 cm (the normal minimum). If the fist fits comfortably, the bi-ischial diameter is ≥8 cm (adequate outlet). A more precise measurement uses a Thoms pelvimeter.
Step 4 — Assessment of the subpubic angle:
Place both thumbs at the inferior border of the pubic symphysis and estimate the angle subtended by the pubic rami. Normal: the two thumbs can be placed side by side comfortably (approximately 90° = two finger widths). A narrow subpubic angle (<85°) forces the fetal head toward the sacrum and reduces the functional transverse diameter of the outlet.
Step 5 — Overall clinical impression:
Summarise findings: DC and estimated obstetric conjugate; ischial spine prominence; sacral curve; subpubic angle; bi-ischial diameter. Classify as: adequate pelvis (all measurements within normal), borderline pelvis (one or more borderline measurements), or contracted pelvis (one or more measurements below threshold — particularly obstetric conjugate <10 cm).