Page 20 of 30
OG8.9 | Stillbirth Evaluation — SDL Guide (Part 2)
Management — Delivery and Aftercare
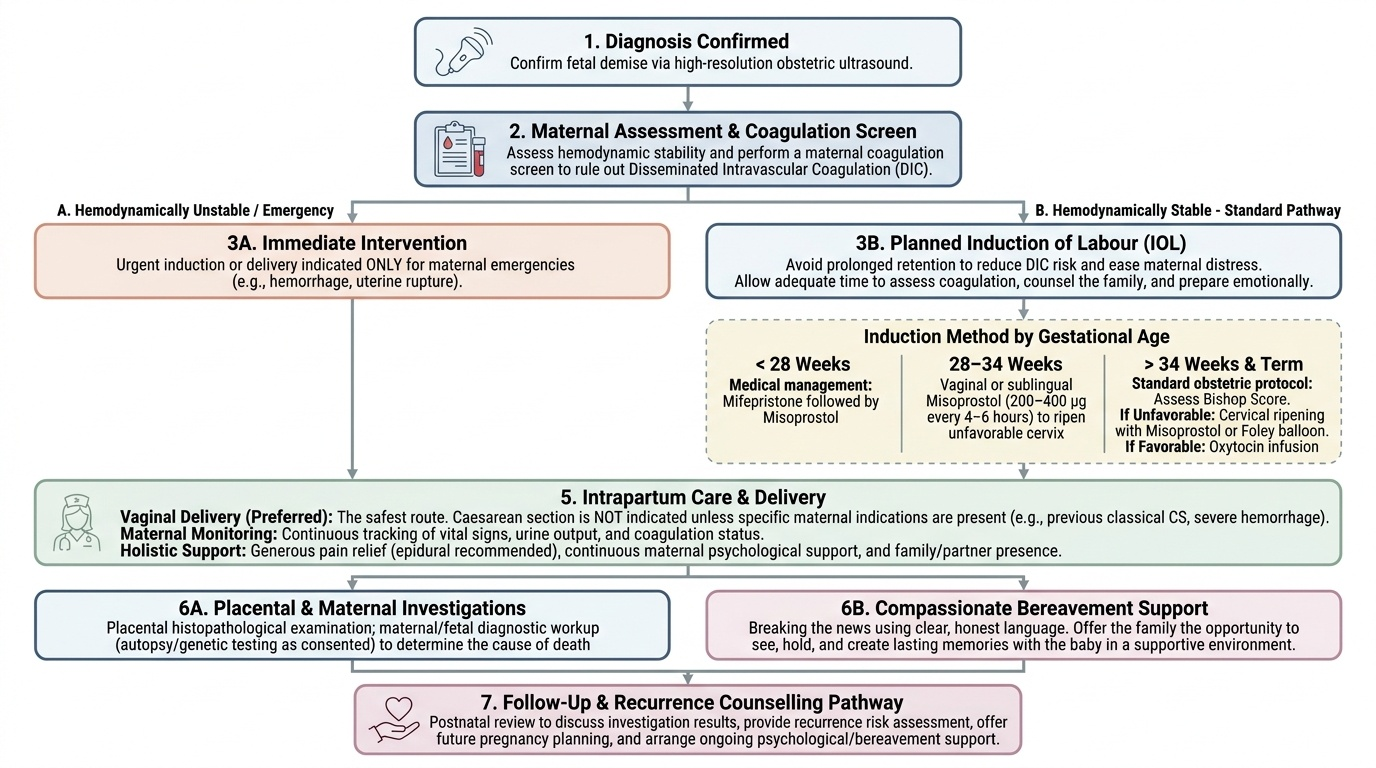
The management of stillbirth encompasses three domains: decision-making about delivery, obstetric and medical care during delivery, and postnatal care including bereavement support, investigation review, and recurrence counselling. All three are equally important and must be handled with clinical precision and human sensitivity.
Decision about timing of delivery:
The majority of antepartum stillbirths are managed by induction of labour (IOL) rather than waiting for spontaneous labour. The reasons are: (a) risk of DIC increases with prolonged retention of dead fetus; (b) prolonged waiting causes significant psychological harm to the mother; (c) most women strongly prefer to know and deliver rather than to wait. However, there is no emergency requiring immediate IOL in a haemodynamically stable woman — adequate time to assess coagulation and inform the family is appropriate.
Method of induction:
- Before 28 weeks: Mifepristone + misoprostol (medical management) is preferred.
- 28–34 weeks: Misoprostol (200–400 µg per vagina or sublingual, at 4–6 hourly intervals) is the most commonly used regimen. The cervix is often unfavourable — misoprostol is effective at ripening in this range.
- After 34 weeks (and at term): Induction as per standard protocol — assess Bishop score; misoprostol or Foley balloon for cervical ripening if unfavourable; oxytocin infusion once cervix is favourable. Vaginal delivery is the preferred route in the vast majority of cases — caesarean section is NOT indicated for a stillbirth unless there is a specific maternal indication (uterine rupture, previous classical CS, haemorrhage).
Intrapartum care:
- Monitor maternal vital signs, urine output, and coagulation status throughout labour.
- Pain relief should be offered generously — epidural analgesia is appropriate.
- Continuous maternal psychological support (a nurse or midwife with the mother throughout labour).
- Allow the father or a support person to be present if the family wishes.
Bereavement care — non-negotiable component of management:
- Breaking the news: Use clear, compassionate language. Do not use euphemisms ('we lost the baby'). Explain clearly: 'Your baby's heart has stopped beating. I am very sorry. Your baby has died.'
- Viewing and holding the baby: Families should always be offered the opportunity to see and hold the stillborn. Research consistently shows this helps the grieving process. Never assume they do not want to. Respect the decision if they decline.
- Memory-making: Offer a photograph, hand/footprint. These become important mementos for grieving families.
- Information giving: Explain the investigation plan clearly. Avoid speculation about causes at this stage — investigations take time, and premature attribution may be wrong.
- Referral to bereavement counselling: Formal psychological support should be offered; pastoral care (chaplaincy/religious support per the family's faith) should be facilitated.
- Registration: In India, stillbirths (≥28 weeks) must be registered under the Registration of Births and Deaths Act 1969. The hospital issues a certificate; the family registers with the local municipality.
DIC management (if coagulopathy develops):
- Fresh frozen plasma (FFP) to replace clotting factors.
- Cryoprecipitate for fibrinogen replacement.
- Platelet concentrate if platelets <50,000.
- Treat underlying cause (prompt delivery is the primary treatment).
Recurrence counselling:
- Review investigation results at the 6-week postnatal visit.
- Explain the identified cause and its recurrence risk (varies from <1% for isolated cord accident to >20% for antiphospholipid syndrome or poorly controlled diabetes).
- Plan for the next pregnancy: enhanced surveillance schedule, low-dose aspirin for antiphospholipid syndrome, folic acid supplementation, optimal management of underlying maternal disease.
Provided image
Self-Assessment
Having worked through the presentation, classification, causes, investigation, and management of stillbirth, use the following questions to consolidate your knowledge at the level required by OG8.9 (KH — Knowledge and How). The examination commonly tests definition thresholds, ability to classify by maceration state, knowledge of the ReCoDe system, and the investigation and management protocol. The viva or practical assessment may present a clinical scenario involving a dead fetus at term and ask you to outline an integrated management plan covering diagnosis, maternal investigations, route of delivery, and bereavement care. University written examinations frequently ask short-answer or essay questions on enumeration of causes and investigation protocol. OSCE or practical assessments may probe your attitude and communication skill around breaking bad news — a component that is examined but often under-prepared. Approach each consolidation question below systematically, formulating your answer before checking against the module content.
Key consolidation questions:
- Define stillbirth using the India/NMC definition. How does it differ from abortion and neonatal death?
- Distinguish fresh from macerated stillbirth — what does each imply about timing?
- Name the eight ReCoDe categories and give one example condition for each.
- Which three investigations must be done BEFORE induction of labour for a stillbirth, and why?
- A woman with a 36-week stillbirth has a coagulation screen showing elevated D-dimer and low fibrinogen. What is the diagnosis, and how do you manage it?
- Describe three key elements of bereavement care that are non-negotiable.
- What legal requirement applies to a stillbirth at 32 weeks in India?
CLINICAL PEARL
Never diagnose stillbirth on auscultation alone — always confirm by real-time ultrasound before informing the family. Auscultation can miss a slow fetal heart or be misled by maternal heart sounds, and a wrong diagnosis of stillbirth is a devastating error. On the other hand, once confirmed, do not delay informing the family or performing coagulation screening — every hour of retained dead fetus increases the risk of DIC. The most preventable stillbirths in India are intrapartum fresh stillbirths — these should be zero in a facility with skilled birth attendance and cardiotocography. Every intrapartum death should trigger a critical incident review. Finally, for examinations: the ReCoDe system is the current preferred classification; 'unexplained' is a legitimate category only after full investigation.
SELF-CHECK
Under the Registration of Births and Deaths Act 1969 (India), which of the following events requires formal registration as a 'stillbirth'?
A. Delivery of a dead fetus at 20 weeks weighing 450 g
B. Delivery of a dead fetus at 30 weeks weighing 1200 g
C. Neonatal death within 24 hours of a live birth at 32 weeks
D. Death of a twin at 26 weeks in utero
Reveal Answer
Answer: B. Delivery of a dead fetus at 30 weeks weighing 1200 g
India's legal definition of stillbirth for registration purposes requires ≥28 weeks gestational age OR ≥1000 g birth weight with no signs of life. Option B (30 weeks, 1200 g) meets both criteria and must be registered as a stillbirth. Option A (20 weeks, 450 g) falls below both thresholds and is classified as abortion. Option C describes a neonatal death (live birth followed by death) — a different registration category. Option D (26 weeks in utero) meets neither threshold for Indian stillbirth registration.