Page 16 of 23
OG9.6 | Hyperemesis Gravidarum — SDL Guide
Learning Objectives
- Define hyperemesis gravidarum and distinguish it from physiological nausea and vomiting of pregnancy using the established diagnostic criteria
- Explain the aetiopathogenesis of hyperemesis gravidarum, including the roles of β-hCG, oestrogen, H. pylori, and the mechanism of gestational transient thyrotoxicosis
- Apply the PUQE score to quantify severity and outline the essential investigations required to confirm the diagnosis and exclude secondary causes
- Identify the complications of hyperemesis gravidarum, particularly Wernicke's encephalopathy, and explain why thiamine must precede dextrose infusion
- Describe the stepwise inpatient management including IV rehydration, the antiemetic ladder, electrolyte correction, thromboprophylaxis, and nutritional support
INSTRUCTIONS
Hyperemesis gravidarum is a potentially life-threatening complication of early pregnancy that demands prompt recognition and systematic management. While many pregnant women experience some nausea and vomiting in the first trimester, the small subset who develop true hyperemesis face serious maternal risks — most critically Wernicke's encephalopathy — if management is delayed or if the sequence of fluid administration is wrong. This SDL teaches you to distinguish hyperemesis from normal pregnancy sickness, work through a targeted investigation protocol, and apply evidence-based treatment. The single most important clinical pearl — give thiamine before dextrose — will be woven through every section of this module.
References
- DC Dutta's Textbook of Obstetrics, 10th edition, Ch 11 (Hyperemesis Gravidarum) (textbook)
- Williams Obstetrics, 26th edition, Ch 54 (Nausea and Vomiting) (textbook)
- RCOG Green-top Guideline 69 — The Management of Nausea and Vomiting of Pregnancy and Hyperemesis Gravidarum (2024) (guideline)
- Shaw's Textbook of Gynaecology, 16th edition (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 26-year-old primigravida at 9 weeks gestation is brought to the emergency department by her husband after three days of unable to keep anything down — not even water. She has lost 4 kg since her booking visit four weeks ago, her lips are cracked, she feels too weak to stand, and she is visibly distressed. Her urine dipstick shows 3+ ketones. As you arrange IV access, the nurse asks: "Should we start dextrose saline or Ringer's lactate?" You hesitate — then you remember something critical. Before any drip goes in, this patient needs one drug first. What is it, and why does the sequence matter so much?
WHY THIS MATTERS
Nausea and vomiting in early pregnancy is one of the commonest conditions you will encounter in obstetric practice, affecting up to 80% of pregnant women. Most resolve spontaneously. But hyperemesis gravidarum (HG) — the severe, pathological end of this spectrum — complicates 0.3–3% of pregnancies and remains a significant cause of hospital admission in the first trimester. If unrecognised or mismanaged, it carries genuine life-threatening consequences: Wernicke's encephalopathy, which can leave permanent neurological damage or cause death, is the most serious. For the MBBS student entering clinical rotations, knowing where the spectrum crosses from normal to pathological, and knowing the right sequence of interventions, can prevent an iatrogenic disaster.
RECALL
Before proceeding, retrieve some foundational knowledge. Recall that β-hCG (beta human chorionic gonadotrophin) is produced by trophoblastic tissue from implantation and peaks between 8–10 weeks of gestation — this is exactly the window when HG is worst. Recall that thiamine (vitamin B1) is a water-soluble vitamin essential for glucose metabolism in the brain; its stores are depleted within two to three weeks of poor oral intake. Recall from physiology that the thyroid-stimulating hormone (TSH) receptor has structural homology with the hCG receptor, which is why very high hCG levels can produce biochemical thyroid changes. Finally, recall that pregnancy itself is a hypercoagulable state — a fact that becomes clinically relevant when a woman is also dehydrated and immobile.
Clinical Presentation and Diagnosis of Hyperemesis Gravidarum
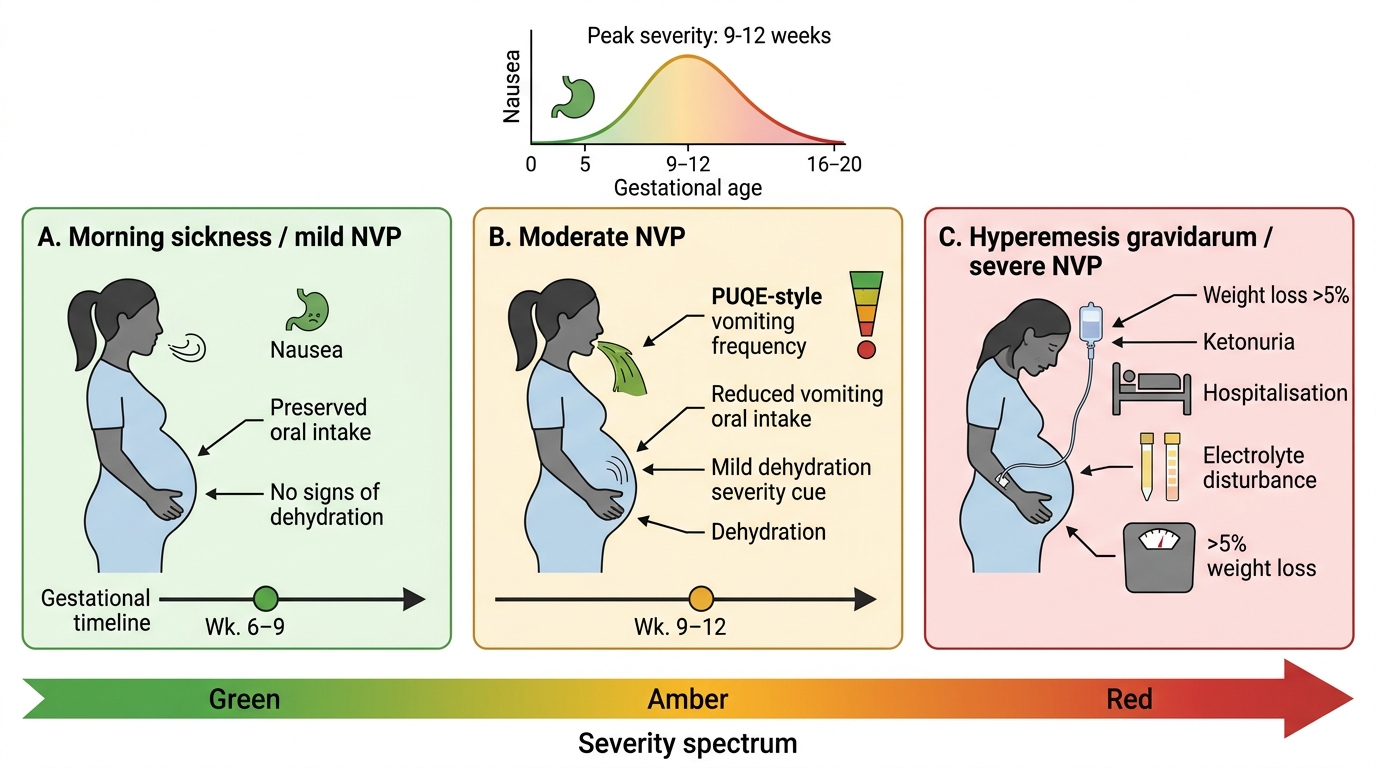
The nausea and vomiting of early pregnancy exists along a severity spectrum, and understanding where normal ends and pathological begins is the foundation of clinical management. In the majority of pregnancies, nausea and vomiting of pregnancy (NVP) begins around 4–6 weeks, peaks between 8–12 weeks, and resolves for most women by 16 weeks. It does not usually cause significant weight loss, dehydration, or electrolyte disturbance, and it can be managed at home with dietary modification and, when needed, outpatient antiemetics.
Hyperemesis gravidarum is the severe end of this spectrum. It is a clinical diagnosis characterised by three defining features: (1) intractable vomiting that is not relieved by standard anti-emetic measures; (2) weight loss exceeding 5% of pre-pregnancy body weight; and (3) evidence of dehydration and starvation, most usefully demonstrated by ketonuria ≥2+ on urine dipstick. Electrolyte disturbances — particularly hypokalaemia and hyponatraemia — and occasionally transaminase elevation complete the biochemical picture of a woman in a catabolic, nutritionally depleted state.
The onset of HG mirrors the hCG curve: symptoms are most severe between 8–10 weeks and in most cases begin to improve by 16–20 weeks, though a minority of women suffer throughout pregnancy. Clinically, the woman with HG is unable to retain oral fluids, may have ptyalism (excessive salivation which she cannot swallow), and shows signs of dehydration: sunken eyes, dry mouth, poor skin turgor, and reduced urine output. The presence of Mallory-Weiss tears — longitudinal mucosal lacerations at the gastro-oesophageal junction from repeated retching — should be considered when there is haematemesis.
To quantify severity, the PUQE (Pregnancy-Unique Quantification of Emesis) score is a validated three-item instrument asking: how many hours per day do you feel nauseated (1–5 points), how many times per day do you vomit (1–5 points), and how many retching episodes per day (1–5 points). The total score classifies severity: mild ≤6, moderate 7–12, severe ≥13. Although originally developed for NVP, PUQE guides clinical decision-making in HG and is increasingly required in structured assessments.
Spectrum of Nausea and Vomiting in Early Pregnancy
SELF-CHECK
A 28-year-old woman at 10 weeks gestation presents with vomiting 8 times a day for 2 weeks. She has lost 3.2 kg from her pre-pregnancy weight of 55 kg (5.8% loss). Urine dipstick shows 3+ ketones. Serum potassium is 2.9 mEq/L. Which single criterion BEST establishes this as hyperemesis gravidarum rather than moderate NVP?
A. Gestational age of 10 weeks
B. Vomiting frequency of 8 times per day
C. Weight loss of 5.8% of pre-pregnancy body weight with ketonuria
D. Serum potassium of 2.9 mEq/L
Reveal Answer
Answer: C. Weight loss of 5.8% of pre-pregnancy body weight with ketonuria
The defining diagnostic threshold for hyperemesis gravidarum is weight loss >5% of pre-pregnancy body weight combined with ketonuria, reflecting dehydration and starvation. The 5.8% loss plus 3+ ketones here is the defining criterion. Vomiting frequency and hypokalaemia are consequences, not the primary diagnostic threshold. Gestational age simply contextualises the timing.
Aetiology and Pathophysiology
The pathophysiology of hyperemesis gravidarum is multifactorial, and no single cause has been identified. However, several interacting biological, infectious, and psychosocial factors contribute to a coherent mechanistic picture that explains both the timing and the severity.
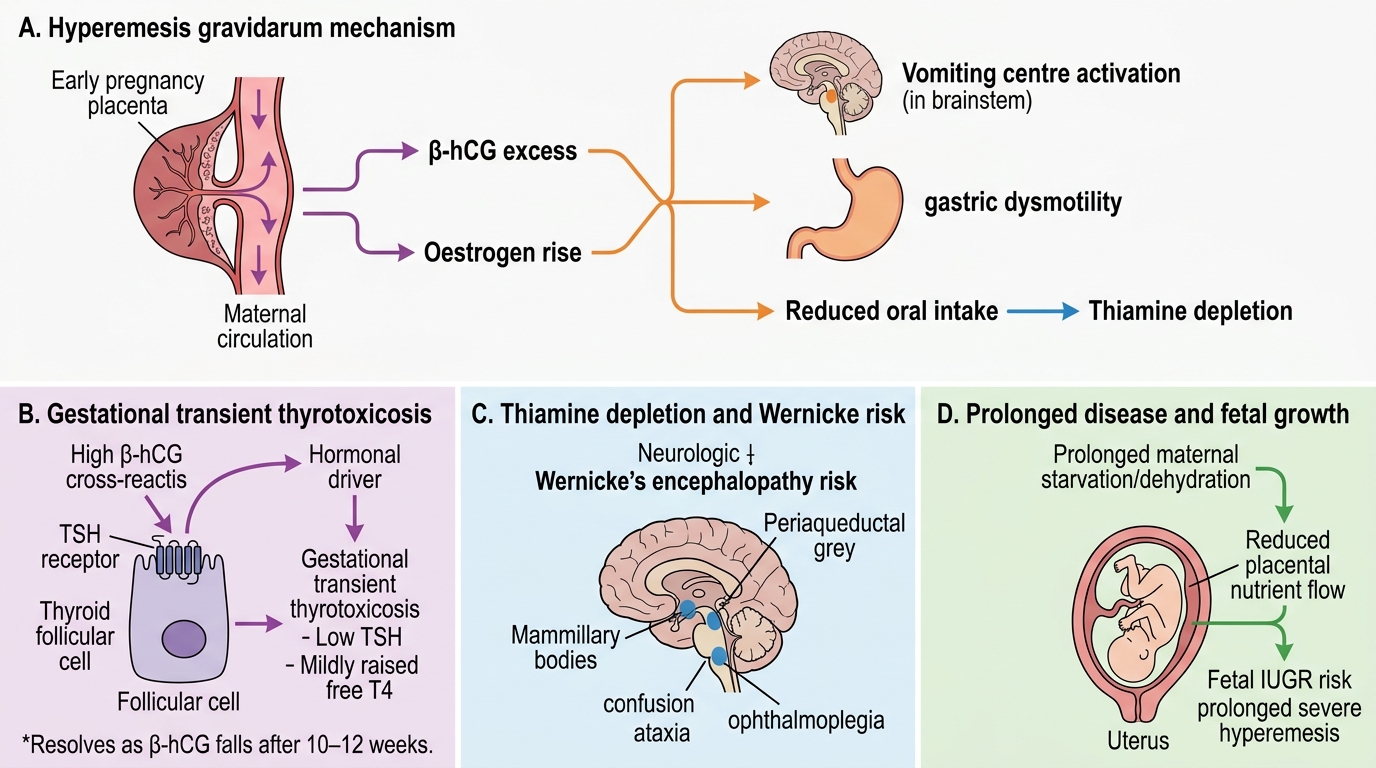
The central driver: β-hCG excess. The most consistently implicated factor is a direct relationship between circulating β-hCG and emetic severity. β-hCG stimulates the chemoreceptor trigger zone and acts on gastric parietal cells to increase acid production and slow gastric emptying. This explains why HG peaks at 8–10 weeks — the moment of maximum hCG — and why conditions that produce supraphysiological hCG, such as molar pregnancy and multiple gestation, are associated with unusually severe vomiting. Oestrogen, which also peaks in early pregnancy, sensitises the emetic centre and the vestibular apparatus, compounding the nausea.
Gestational transient thyrotoxicosis. Because β-hCG shares structural homology with TSH, high circulating hCG levels cross-react with the TSH receptor on thyroid follicular cells, stimulating thyroid hormone synthesis. This produces gestational transient thyrotoxicosis (GTT), seen biochemically in up to 60% of women with HG: a suppressed TSH with mildly elevated free T4. Critically, GTT does not require antithyroid treatment — it resolves as hCG falls and does not represent autoimmune Graves' disease. However, it must be distinguished from true hyperthyroidism (look for anti-thyroid antibodies, goitre, or eye signs).
Helicobacter pylori. An association between H. pylori infection and HG has been documented in multiple studies. The proposed mechanism involves gastric mucosal irritation and altered gastric emptying. Eradication of H. pylori in women with confirmed infection and refractory HG has been shown in some studies to reduce symptom severity.
Psychosocial and genetic factors. Psychological factors including anxiety, ambivalence about pregnancy, and prior adverse experiences may amplify emesis, though they do not cause HG de novo. A family history of HG, a personal history of HG in a prior pregnancy (recurrence risk approximately 15–20%), motion sickness, and a history of migraine are all established risk factors, pointing to a genetic predisposition in some women.
Downstream metabolic consequences. Prolonged vomiting and inability to eat depletes glycogen stores, forcing the body into starvation ketosis (ketones in urine) and protein catabolism. Most critically, thiamine (vitamin B1) — a water-soluble vitamin with very limited body stores — becomes depleted within 2–3 weeks of poor oral intake. Since thiamine is essential for the pyruvate dehydrogenase complex and the pentose phosphate pathway, its deficiency selectively damages the metabolically most active brain regions, particularly the mamillary bodies and periventricular grey matter, producing the biochemical substrate for Wernicke's encephalopathy. This complication is entirely preventable — but only if thiamine is administered before glucose (dextrose) is given, because glucose infusion in a thiamine-depleted state rapidly consumes the remaining thiamine reserves, precipitating acute neurological crisis.
Mechanism and Complications of Hyperemesis Gravidarum
SELF-CHECK
A woman with hyperemesis gravidarum at 9 weeks has a TSH of 0.03 mIU/L (low) and free T4 of 22 pmol/L (mildly elevated). She has no goitre, no eye signs, and no thyroid antibodies. What is the most appropriate next step regarding her thyroid status?
A. Start carbimazole immediately to prevent thyroid storm
B. Arrange urgent endocrinology referral for radioiodine therapy
C. Observe and repeat TFTs at 20 weeks — this is gestational transient thyrotoxicosis
D. Start propranolol to control the tachycardia from thyrotoxicosis
Reveal Answer
Answer: C. Observe and repeat TFTs at 20 weeks — this is gestational transient thyrotoxicosis
The biochemical picture — suppressed TSH with mildly elevated fT4, NO antibodies, NO goitre, NO eye signs — is classic gestational transient thyrotoxicosis (GTT) caused by β-hCG cross-reacting with the TSH receptor. GTT resolves spontaneously as β-hCG falls after 10–12 weeks and does NOT require antithyroid treatment. Carbimazole would be inappropriate and potentially teratogenic. Repeat TFTs at 20 weeks after resolution is appropriate.
Investigations and Differential Diagnosis
When a pregnant woman presents with severe vomiting in the first trimester, the clinical task is two-fold: quantify the severity and biochemical impact of the vomiting, and exclude secondary causes that may mimic or complicate HG. Hyperemesis gravidarum is a diagnosis of exclusion — secondary causes must be ruled out before ascribing the vomiting to HG.
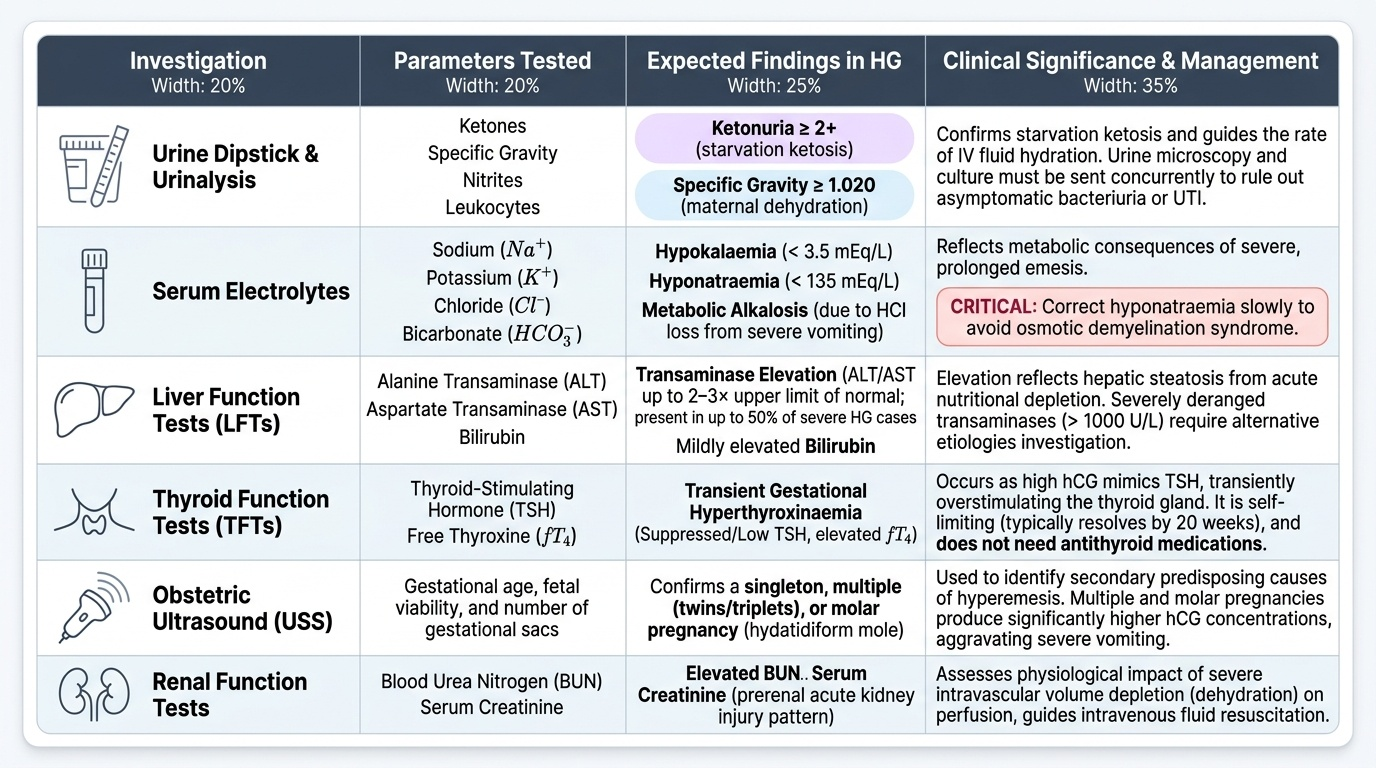
Urinalysis is the first and most accessible test. Urine dipstick demonstrating ketonuria ≥2+ confirms starvation ketosis and supports the diagnosis of HG. Specific gravity >1.020 reflects dehydration. Importantly, urine should also be sent for microscopy and culture, as urinary tract infections (UTI) can precipitate or worsen vomiting in pregnancy and must not be missed.
Serum electrolytes typically reveal the metabolic consequences of prolonged vomiting and poor intake: hypokalaemia (serum potassium <3.5 mEq/L) due to vomiting-driven losses and secondary hyperaldosteronism; hyponatraemia (serum sodium <135 mEq/L) in severe cases; and metabolic alkalosis from loss of hydrochloric acid in vomitus. These electrolyte abnormalities must be corrected, and the correction must be gradual — overly rapid correction of hyponatraemia risks osmotic demyelination syndrome.
Liver function tests (LFTs) show transaminase elevation (ALT/AST) in up to 50% of women with severe HG, likely reflecting hepatic steatosis from nutritional depletion. Bilirubin may be mildly elevated. However, markedly deranged LFTs should prompt consideration of other diagnoses (acute fatty liver of pregnancy, hepatitis A/E, cholestasis).
Thyroid function tests (TFTs) are essential because, as described in the pathophysiology section, up to 60% of women with HG have a suppressed TSH and elevated fT4 (gestational transient thyrotoxicosis). TFTs contextualise the biochemistry and allow exclusion of autoimmune hyperthyroidism (positive anti-TPO or anti-TSH receptor antibodies with clinical features of Graves' disease).
Pelvic ultrasound is mandatory in every woman with HG to exclude two high-hCG states: molar pregnancy (gestational trophoblastic disease, GTD) and multiple pregnancy. A hydatidiform mole produces extremely high β-hCG, causing the most severe end of the HG spectrum, and carries its own oncological management pathway. Multiple pregnancy is an established predisposing factor. Ultrasound establishes viability, gestational age, number of fetuses, and uterine and adnexal anatomy.
The differential diagnosis of vomiting in early pregnancy is broad: appendicitis (right iliac fossa tenderness, fever, raised WCC), acute pancreatitis (elevated lipase, upper abdominal pain), peptic ulcer disease (epigastric pain, H. pylori), hepatitis A/E (jaundice, liver tenderness, hepatitis serology), diabetic ketoacidosis (elevated glucose, acidosis), and in the later first trimester, urinary tract obstruction. A thorough history and examination, supplemented by targeted investigations, distinguishes these from HG.
Provided image