Page 3 of 17
OG10.1 | Antepartum Haemorrhage — SDL Guide (Part 3)
Management of Placenta Praevia
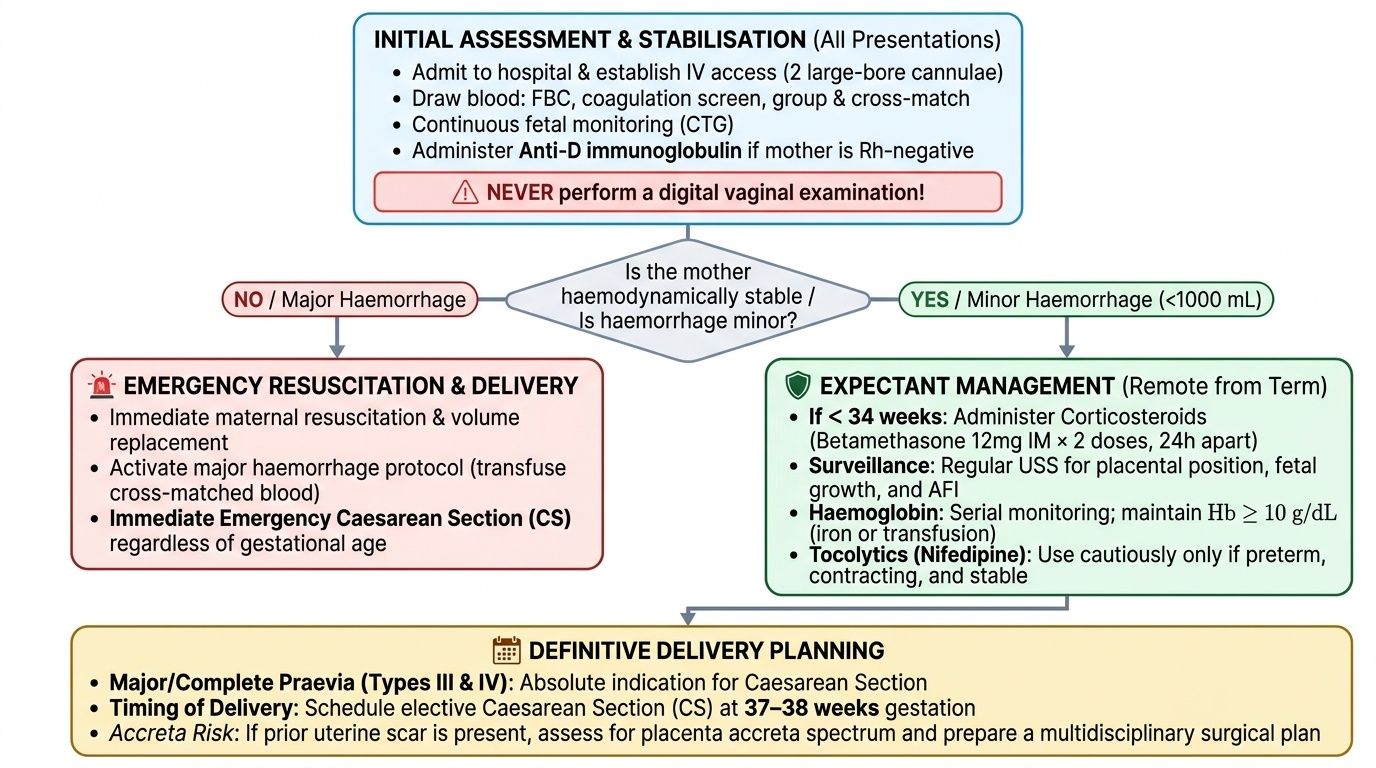
Management of placenta praevia depends on four intersecting variables: the type of praevia (I–IV), the current gestational age, the haemodynamic status of the mother, and whether active labour is present. The overarching principles that govern every decision are: first, preserve maternal life regardless of gestational age; second, give the fetus every achievable opportunity for further maturation before delivery; and third, plan both the timing and route of delivery to minimise haemorrhagic risk. In practice this means that minor praevia in a stable preterm patient is managed expectantly with close surveillance, while major praevia in an unstable patient mandates immediate resuscitation and emergency caesarean section regardless of gestation. The type of praevia is decisive for delivery route — Types III and IV (major or complete praevia) are absolute indications for caesarean section because the placenta physically obstructs the birth canal and any attempt at vaginal delivery would shear the placenta and cause uncontrollable haemorrhage. The evolving risk of placenta accreta spectrum in patients with a prior uterine scar must also be considered in every case of praevia, and a multidisciplinary plan should be activated when accreta is suspected.
Initial stabilisation — all presentations:
- Admit to hospital with IV access (two large-bore cannulae), blood taken for FBC, coagulation screen, group and cross-match.
- Continuous fetal monitoring with CTG.
- Corticosteroids (betamethasone 12 mg IM × 2 doses, 24 hours apart) if gestation <34 weeks and delivery is likely — to accelerate fetal lung maturity.
- Anti-D immunoglobulin for all Rh-negative mothers.
- NEVER perform a digital vaginal examination.
Management of minor APH (haemodynamically stable, <1000 mL blood loss):
- Expectant management if remote from term (under 36–37 weeks), bleeding has stopped, fetal condition is reassuring, and praevia is Type I or II.
- Hospitalise until at least 34–36 weeks.
- Regular USS surveillance for placental position, fetal growth, and AFI.
- Serial haemoglobin monitoring; maintain Hb >10 g/dL with iron supplementation or transfusion.
- Tocolytics (nifedipine) may be used cautiously to stop contractions if preterm and cervix is unfavourable — but only in haemodynamically stable patients.
- Deliver at 36–37 weeks for Types II–IV (even if not bleeding), because the risk of unpredictable major haemorrhage rises sharply at term.
Management of major APH (haemodynamically unstable, ≥1000 mL, or fetal compromise):
- Emergency resuscitation: IV fluid resuscitation, blood transfusion, oxygen, call for senior obstetric and anaesthetic help.
- Emergency CS regardless of gestational age — fetal age is secondary to maternal and fetal survival.
- Prepare for potential hysterectomy if PAS is suspected or uterine bleeding is uncontrollable.
Route of delivery:
- Types I and II posterior praevia: Vaginal delivery may be attempted if the fetal head is engaged and pressing against the placenta (acting as a 'tamponade'), bleeding is minor, and theatre is immediately available.
- Types III and IV (major praevia) / all central praevia: Caesarean section is mandatory. Schedule elective CS at 37–38 weeks for Types III–IV.
- PAS suspected: Multidisciplinary team — senior obstetrician, urology, vascular surgery, interventional radiology, blood bank, NICU. Planned CS-hysterectomy may be needed.
Provided image
Management of Placental Abruption
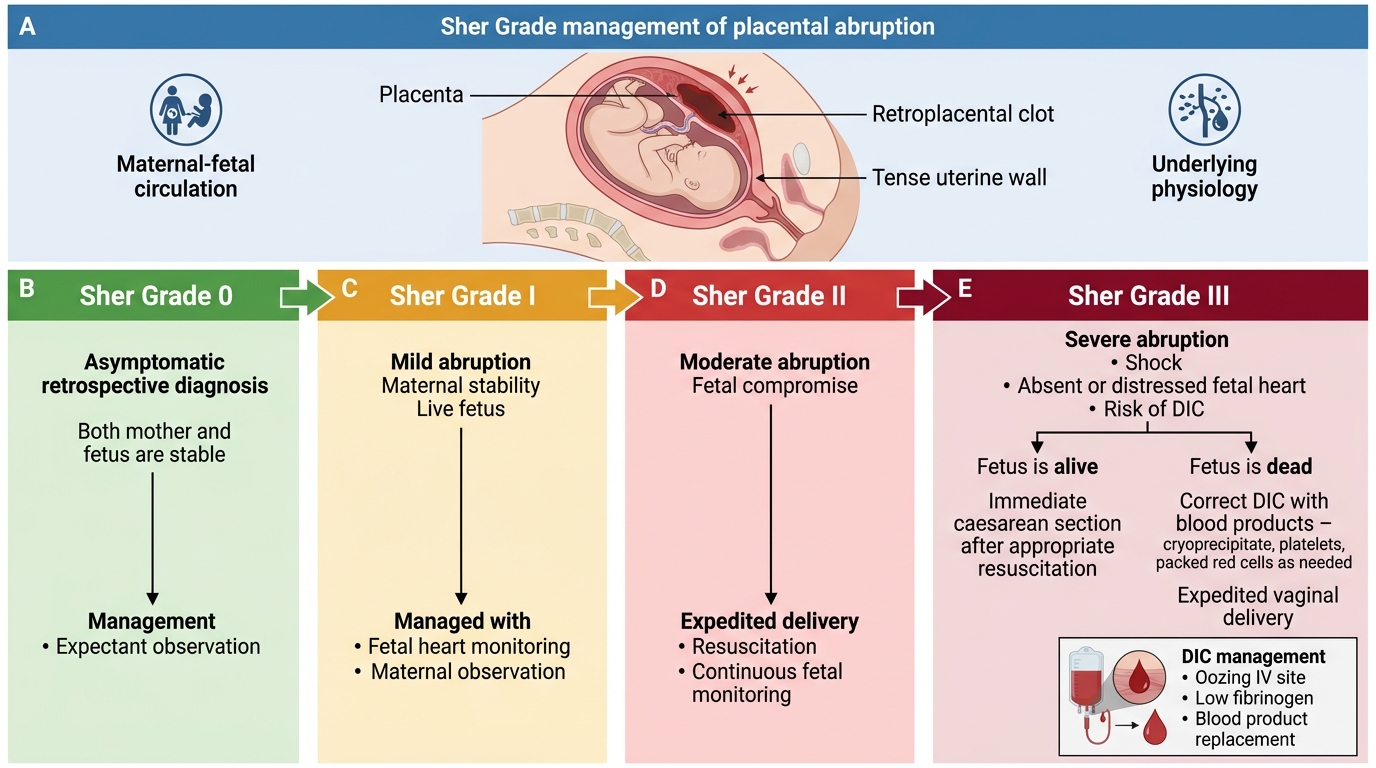
Placental abruption is an unpredictable, potentially catastrophic obstetric emergency whose severity can escalate within minutes. Because the retroplacental haematoma expands silently and the degree of external bleeding consistently underestimates the true volume of haemorrhage — especially in concealed abruption — clinicians must act on haemodynamic status and fetal well-being, not on the quantity of visible blood. Every management decision is fundamentally guided by two parameters: the haemodynamic status of the mother and the condition of the fetus, as assessed by continuous cardiotocography. The Sher grading system (Grades 0–III) provides a practical, clinically validated framework for calibrating management intensity to the severity of separation. Grade 0 and I cases can be managed expectantly if the fetus is viable and preterm; Grade II requires urgent delivery to rescue the compromised fetus; Grade III, where fetal death has occurred, shifts the management goal entirely to maternal survival, with the additional complexity of disseminated intravascular coagulation in Grade IIIb. In all grades, simultaneous resuscitation and investigation must proceed in parallel from the moment of presentation.
Initial resuscitation and monitoring (all grades):
- Two large-bore IV cannulae; aggressive fluid resuscitation with crystalloid and colloid while awaiting blood.
- Blood for FBC, coagulation screen (PT, aPTT, fibrinogen, D-dimers), group and cross-match, urea and electrolytes.
- Urinary catheter for continuous urine output monitoring (target ≥30 mL/h).
- Continuous CTG monitoring.
- Anti-D for Rh-negative mothers (Kleihauer-Betke to guide anti-D dose).
Grade-based management:
Grade 0 and I (minor, no maternal/fetal compromise):
- Haemodynamically stable; no fetal distress.
- If preterm (<37 weeks): expectant management under close observation; corticosteroids if <34 weeks.
- If at term: may proceed to delivery (augment labour or CS if other indications).
- Regular fetal surveillance — biophysical profile, growth scans.
Grade II (moderate, fetal distress present, no fetal death):
- Urgent delivery is indicated to prevent progression to fetal death.
- Rapid amniotomy (AROM) may reduce intrauterine pressure and decrease further placental separation; also accelerates labour.
- If vaginal delivery is imminent (≥8 cm dilated) and fetal condition permits: expedite vaginal delivery.
- If delivery is not imminent or CTG is severely abnormal: emergency CS is indicated.
- Prepare blood products — at minimum 2–4 units packed red cells.
Grade III (severe, fetal death — IIIa without DIC, IIIb with DIC):
- Fetal death has occurred. The primary goal shifts entirely to maternal survival.
- IIIa (no coagulopathy): Induce and expedite vaginal delivery in most cases (lower maternal morbidity than CS when fetus is dead). AROM + Syntocinon infusion. The uterine tetany usually resolves with delivery, and the uterus typically contracts well.
- IIIb (with DIC): Simultaneously manage haemorrhage AND coagulopathy.
- Fibrinogen replacement: 4–6 g cryoprecipitate (each unit ≈ 250 mg fibrinogen); target fibrinogen >2 g/L.
- Fresh Frozen Plasma (FFP): 10–15 mL/kg to replace consumed clotting factors; target PT/aPTT <1.5× normal.
- Platelets: Transfuse if count <50×10⁹/L with active bleeding, or <20×10⁹/L prophylactically.
- Packed Red Cells: Maintain Hb ≥8 g/dL in the actively bleeding patient.
- Vaginal delivery preferred; CS carries enormous risk of uncontrollable haemorrhage in a coagulopathic patient.
Couvelaire uterus (uteroplacental apoplexy):
If at CS the uterus is found to be suffused with blood (blue-black discolouration), this is Couvelaire uterus — extensive myometrial infiltration of blood impairing contractility. Management: uterotonic agents, B-Lynch suture, internal iliac artery ligation, or hysterectomy if PPH is uncontrollable.
Sher Grade Management of Placental Abruption
SELF-CHECK
A patient at 36 weeks develops sudden severe abdominal pain, a rock-hard uterus, and absent fetal heart sounds. Her blood pressure is 80/50 mmHg and blood is oozing from the IV site. Coagulation screen shows fibrinogen 0.6 g/L. Which statement best describes the next management step?
A. Immediate caesarean section to save the fetus
B. Transfuse 4–6 units of packed red cells and proceed to CS under general anaesthesia
C. Resuscitate, replace fibrinogen with cryoprecipitate, and expedite vaginal delivery
D. Administer IV oxytocin and wait for spontaneous delivery
Reveal Answer
Answer: C. Resuscitate, replace fibrinogen with cryoprecipitate, and expedite vaginal delivery
This is Sher Grade IIIb abruption — fetal death plus DIC (fibrinogen 0.6 g/L is critically low, normal >2 g/L). The fetus is dead so CS is not indicated for fetal reasons. The priority is maternal: correct DIC with cryoprecipitate (fibrinogen), FFP, and platelets, then expedite vaginal delivery — CS in an actively coagulopathic patient carries unacceptable risk of uncontrollable haemorrhage.
CLINICAL PEARL
Three APH traps every final-year student must remember:
- Never perform a digital vaginal examination in APH until the placenta has been localised by USS. This is absolute — it can convert a stable minor haemorrhage into a life-threatening catastrophe if the placenta is praevia.
- Concealed abruption kills by stealth. A patient with a tense, tender, woody uterus and minimal visible bleeding but profound shock has likely lost 1–2 litres into the retroplacental space. Do not be falsely reassured by the 'small' amount of external blood.
- In Grade IIIb abruption (DIC), treat the coagulopathy BEFORE attempting CS. Operating on a patient with fibrinogen <1 g/L without first replacing clotting factors creates a surgical wound that cannot clot — hysterectomy will still not control the haemorrhage. Stabilise coagulation first (cryoprecipitate, FFP), then deliver vaginally wherever possible.
Self-Assessment
By this point in the module you have covered the full clinical span of antepartum haemorrhage — from the precise definition and gestational threshold, through the contrasting pathophysiology of placenta praevia and placental abruption, to the investigation hierarchy anchored by ultrasonography, and the grade- and type-matched management algorithms that determine whether a patient proceeds to expectant care, urgent delivery, or immediate resuscitation and caesarean section. The self-assessment questions below are drawn from the most clinically consequential decision points in the module. Approach each question as you would a viva or OSCE station: formulate your answer first, then read the explanation to confirm or correct your reasoning. Pay particular attention to the Sher grading questions (the most-tested classification in obstetric finals) and the contraindications to vaginal examination and to caesarean section in a coagulopathic patient.
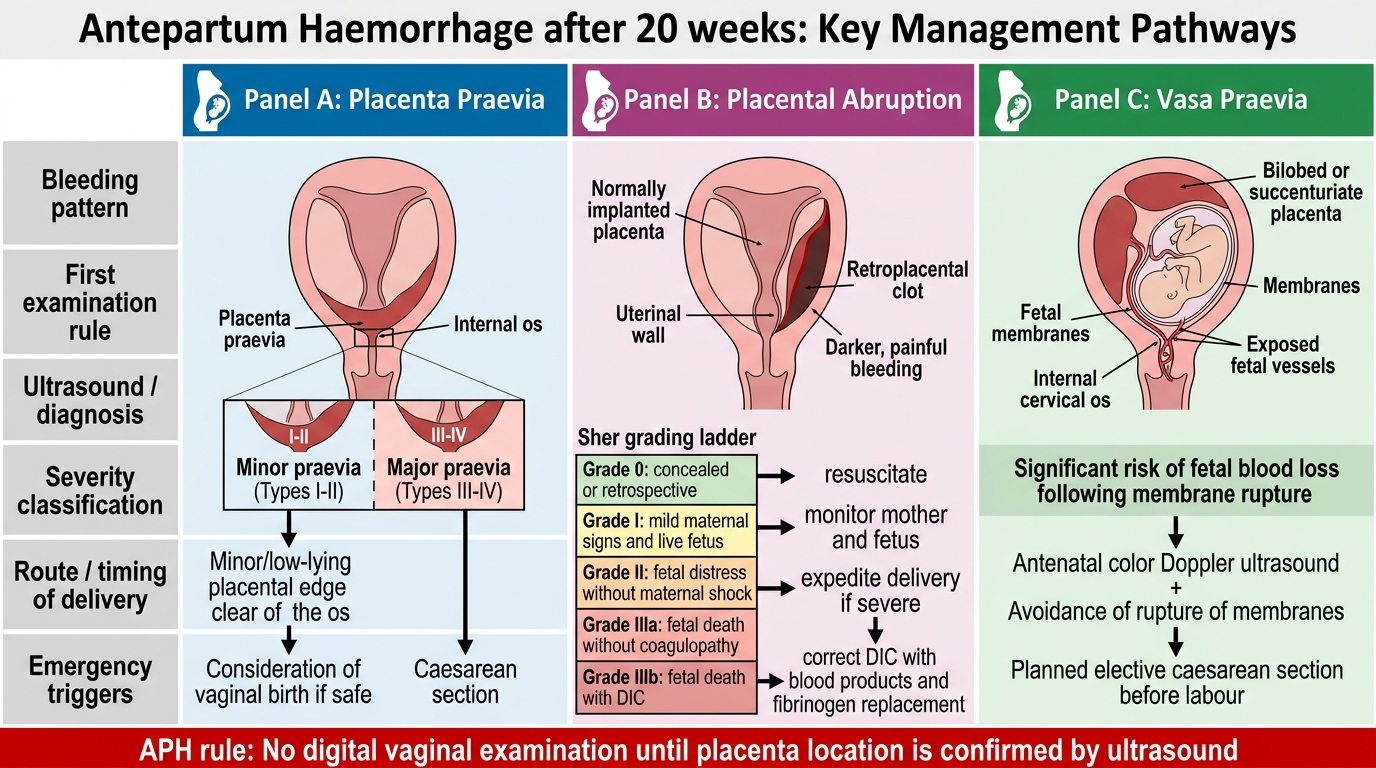
APH Management Pathways: Praevia, Abruption, and Vasa Praevia
Key concepts to revisit:
- The 20-week definition of APH and its distinction from early-pregnancy bleeding
- The four types of placenta praevia and the mandatory management threshold for Types III–IV
- The Sher grading of abruption and grade-specific management
- The rule prohibiting vaginal digital examination before USS
- Couvelaire uterus and its management
- Vasa praevia and why it is uniquely dangerous (fetal blood loss)
- DIC management in abruption: fibrinogen replacement thresholds and product choice
SELF-CHECK
A 26-year-old primigravida at 38 weeks presents with painless fresh bleeding. USS confirms Type IV (complete) placenta praevia. Bleeding has now stopped; she is haemodynamically stable. What is the most appropriate next management?
A. Allow vaginal delivery since she is primigravida
B. Discharge home with outpatient USS follow-up at 40 weeks
C. Admit and plan elective caesarean section at 37–38 weeks (she is now at 38 weeks — proceed to CS)
D. Perform a careful digital cervical assessment to check dilatation
Reveal Answer
Answer: C. Admit and plan elective caesarean section at 37–38 weeks (she is now at 38 weeks — proceed to CS)
Type IV (complete) praevia is an absolute indication for caesarean section. She is at 38 weeks — within the recommended elective CS window of 37–38 weeks for major praevia. Even though bleeding has stopped, expectant management beyond 37–38 weeks for Type IV praevia is inappropriate because of the risk of sudden major haemorrhage. Vaginal examination is absolutely contraindicated.