Page 7 of 17
OG10.2 | Blood Product Use in Obstetric Haemorrhage — SDL Guide (Part 3)
Applied Practice: Case Scenarios in Obstetric Transfusion
The transition from knowing the principles of transfusion medicine to applying them under pressure in a real clinical encounter requires deliberate, goal-directed practice. The knowledge of when to use cryoprecipitate versus FFP, or how to distinguish TRALI from TACO, is only useful if it can be retrieved and applied in the context of a specific patient with specific vital signs, laboratory results, and a time constraint. The three clinical scenarios below are designed to bridge this gap between declarative knowledge (what the products are) and procedural competence (what to do now, with this patient). Each scenario presents a realistic obstetric haemorrhage situation; your task is to identify the dominant physiological deficit, select the correct component(s), state the dose and threshold, and anticipate what complications to monitor. Work through each scenario before reading the analysis — in a supervised clinical placement, you would be observed managing a similar case under consultant guidance, with the expectation of explaining your reasoning aloud.
Provided image
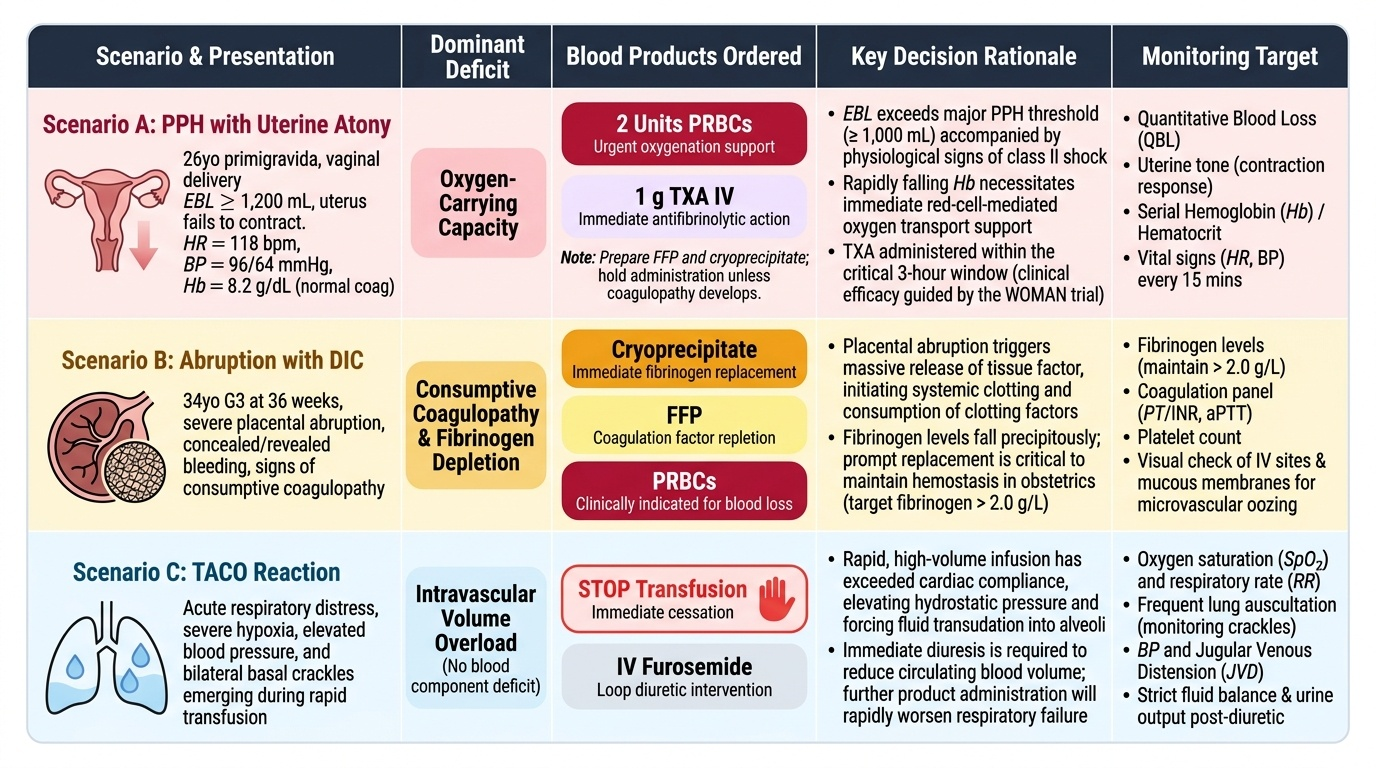
Scenario A — The PPH with Uterine Atony:
A 26-year-old primigravida delivers a 4.2 kg baby vaginally. The placenta is delivered but the uterus fails to contract. Estimated blood loss is 1,200 mL. Oxytocin 20 units in 500 mL saline is running. Pulse 118/min, BP 96/64 mmHg, Hb (sent 30 min ago) 8.2 g/dL, coagulation screen normal, platelet count 145 × 10⁹/L. What do you order?
Analysis: Blood loss exceeds the major PPH threshold (≥1000 mL). Haemoglobin is falling (was 8.2 g/dL 30 min ago — now likely lower). Coagulation is still normal. The deficit is OXYGEN-CARRYING CAPACITY. Order 2 units PRBCs urgently; crossmatch 4 units total. Give tranexamic acid 1 g IV immediately (within the WOMAN trial's 3-hour window). Continue uterotonic escalation (ergometrine if not hypertensive; carboprost if not asthmatic). Prepare FFP and cryoprecipitate in case she develops DIC — but do not give them yet, as coagulation is normal.
Scenario B — The Abruption with DIC:
A 34-year-old gravida 3 at 36 weeks has severe abruption. Fetal heart is absent. BP 80/50 mmHg, Hb 7.1 g/dL, fibrinogen 0.8 g/L (critically low; normal >2 g/L), PT 28 s (normal <14 s), platelets 62 × 10⁹/L, oozing from IV sites.
Analysis: Sher Grade IIIb — fetal death + DIC. The dominant deficits are FIBRINOGEN and ALL CLOTTING FACTORS with borderline platelets. Order: cryoprecipitate 10 units (to raise fibrinogen from 0.8 → aim >2 g/L), FFP 4 units (10–15 mL/kg), 2 units PRBCs (Hb 7.1 with haemodynamic compromise). Platelets are borderline (62 × 10⁹/L) — observe, only transfuse if they fall below 50 in the context of continued bleeding. Target fibrinogen >2 g/L before proceeding to vaginal delivery or any surgical intervention.
Scenario C — Recognising a Transfusion Complication:
A 29-year-old woman is 45 minutes into her second unit of packed red cells post-CS when she becomes dyspnoeic and hypoxic (SpO₂ 88%). BP 148/98 mmHg (elevated), bilateral crackles on auscultation, distended neck veins.
Analysis: The elevated blood pressure and raised JVP distinguish this from TRALI (which causes hypotension) and point to TACO — transfusion-associated circulatory overload. Stop the transfusion. Sit the patient upright. Give furosemide 40 mg IV. Apply high-flow oxygen. Notify the blood bank that the patient has had a reaction. This patient has volume-related pulmonary oedema from the cumulative fluid load of surgery plus 2 units of blood given too rapidly — a slower transfusion rate would have prevented it.
CLINICAL PEARL
Three transfusion principles that are frequently tested and frequently misapplied:
- Cryoprecipitate, not FFP, for fibrinogen replacement in obstetric DIC. FFP contains fibrinogen, but at physiological plasma concentration (~2 g/L) — to raise a patient's fibrinogen from 0.5 g/L to 2 g/L with FFP alone would require an impractical volume (>5 litres). Cryoprecipitate concentrates fibrinogen (~250 mg/unit); 10 units deliver ~2.5 g fibrinogen in approximately 120 mL — efficient and targeted.
- The WOMAN trial window is 3 hours. Tranexamic acid only reduces mortality from obstetric haemorrhage when given within 3 hours of onset. Late administration (>3 hours) shows no benefit. Time matters — this is the single most important actionable evidence-based intervention available at the bedside for PPH.
- Platelets must never be refrigerated. Unlike PRBCs (stored at 4°C) and FFP (−25°C), platelets must be stored at room temperature (20–24°C) with continuous gentle agitation. Refrigeration activates the platelets and renders them non-functional; a 'bag of cold platelets' from the ward fridge will not stop bleeding.
Self-Assessment
You have now covered the complete clinical arc of blood product use in obstetric haemorrhage — from the physiological rationale for each component and the thresholds that trigger their use, through the emergency compatibility protocols and the massive transfusion protocol, to the recognition and management of acute transfusion reactions. This breadth of knowledge is what separates a clinician who can act decisively in a haemorrhage emergency from one who is paralysed by uncertainty about what to order and when. Having worked through the full arc of blood product use in obstetric haemorrhage — from indications and component physiology, through compatibility testing and component selection criteria, to the massive transfusion protocol and transfusion reactions — you should now be able to construct a rational transfusion management plan for any of the scenarios you might encounter in obstetric practice. The questions below focus on the highest-stakes decision points: the threshold values that trigger each component, the critical distinction between TRALI and TACO, the dosing of tranexamic acid, and the implications of ABO incompatibility. Work through each question before reading the explanation.
Key concepts to revisit:
- The composition of cryoprecipitate vs FFP and why cryoprecipitate is preferred for fibrinogen replacement
- The WOMAN trial: population, intervention, outcome, time window
- Emergency O-negative blood: when to use, why Rh matters for women of childbearing age
- Massive transfusion protocol: 1:1:1 ratio, rationale, when to activate
- TRALI vs TACO: mechanism, distinguishing features, management
- Calcium gluconate in massive transfusion: why and how much

Blood Product Pathway in Obstetric Haemorrhage
SELF-CHECK
In a patient with severe obstetric haemorrhage and DIC (fibrinogen 0.7 g/L, PT elevated, platelets 80 × 10⁹/L), which blood product is MOST specifically indicated to correct the fibrinogen deficit?
A. Fresh frozen plasma (FFP) — 4 units
B. Whole blood — 2 units
C. Cryoprecipitate — 10 units
D. Platelet concentrate — 1 pool
Reveal Answer
Answer: C. Cryoprecipitate — 10 units
Cryoprecipitate is the product of choice for fibrinogen replacement. It contains concentrated fibrinogen (~250 mg/unit); 10 units delivers ~2.5 g fibrinogen in a small volume (~120 mL). FFP contains fibrinogen but at physiological plasma concentration (~2 g/L): restoring a critically depleted fibrinogen to therapeutic levels with FFP alone would require impractical volumes (>5 litres). Platelets correct thrombocytopenia but do not replace fibrinogen. Whole blood is not routinely available as a component.