Page 8 of 38
OG12.3 | Diabetes in Pregnancy — SDL Guide (Part 2)
Investigations for Pre-gestational Diabetes Management
Women with pre-gestational diabetes (PGDM) require a more comprehensive investigation protocol than those with GDM, because they have established disease with potential end-organ complications that directly affect pregnancy outcomes. These investigations should ideally be completed during preconception counselling and repeated during pregnancy as clinically indicated.
The cornerstone investigation is HbA1c (glycated haemoglobin), which reflects average plasma glucose over the preceding 2–3 months. In pre-gestational DM, the target HbA1c before conception is below 6.5% (some guidelines aim for below 6.0% if safely achievable without hypoglycaemia). An HbA1c above 10% at conception is associated with a 10-fold increase in major congenital anomalies. During pregnancy, HbA1c targets are typically below 6.5% in the first trimester and below 7.0% in the second and third trimesters, balancing glycaemic control against hypoglycaemia risk. HbA1c is less reliable in the third trimester due to increased red cell turnover.
Self-monitoring of blood glucose (SMBG) is the practical cornerstone of day-to-day management for both GDM and PGDM:
- Fasting target: below 95 mg/dL (5.3 mmol/L)
- 1-hour postprandial target: below 140 mg/dL (7.8 mmol/L)
- 2-hour postprandial target: below 120 mg/dL (6.7 mmol/L)
Organ-specific screening for complications of PGDM:
- Renal function: 24-hour urine protein, serum creatinine, eGFR at booking and each trimester; pre-existing nephropathy worsens pre-eclampsia risk substantially
- Retinal assessment: dilated fundal examination by ophthalmologist at booking and in each trimester; pregnancy can accelerate diabetic retinopathy, and laser treatment may be needed during pregnancy
- Cardiac assessment: ECG, echocardiography if symptomatic or long-standing T1DM; autonomic neuropathy increases risk of postural hypotension and hypoglycaemia unawareness
- Thyroid function: TSH at booking in T1DM (autoimmune association — concurrent Hashimoto's thyroiditis or Graves' disease)
Foetal surveillance:
- First-trimester combined screening (dating scan + nuchal translucency + biochemistry): essential in PGDM to assess aneuploidy risk and for accurate gestational age dating
- Anomaly scan (18–20 weeks): essential in PGDM for detection of cardiac defects and neural tube defects; if cardiac anomaly suspected, foetal echocardiography at 20–24 weeks
- Serial growth scans from 28 weeks (4-weekly): to detect macrosomia and polyhydramnios
- Doppler velocimetry if IUGR suspected (PGDM with nephropathy and vasculopathy can cause IUGR rather than macrosomia)
- Amniotic fluid index (AFI): polyhydramnios (AFI >24 cm or largest pocket >8 cm) is a hallmark of GDM/PGDM, reflecting foetal polyuria in response to foetal hyperglycaemia
Adverse Effects on Mother and Foetus
The adverse effects of diabetes in pregnancy span the entire perinatal period and extend into the long-term health of both mother and child. Understanding these consequences is not merely academic — they provide the clinical rationale for every intervention in this module, from the urgency of early GDM screening to the recommendation for preconception HbA1c optimisation in PGDM. Poorly controlled diabetes creates a cascade of pathological events beginning with maternal hyperglycaemia, progressing to transplacental glucose transfer, driving foetal hyperinsulinaemia, and resulting in the cluster of neonatal complications that obstetricians, paediatricians, and neonatologists must anticipate and manage from the moment of birth. The degree of maternal glycaemic control is the primary determinant of risk, and well-controlled GDM can approach normal-pregnancy perinatal outcomes. Understanding these consequences motivates the clinical urgency of diagnosis and tight glycaemic control, and they form the basis of the NMC examination questions on 'criteria, adverse effects on mother and foetus' (OG12.3).
Diabetes in pregnancy creates a distinct biochemical environment in which maternal hyperglycaemia drives foetal responses — principally foetal hyperinsulinaemia — that account for the majority of the adverse neonatal outcomes. The degree of maternal glycaemic control is the primary determinant of risk; well-controlled GDM approaches normal-pregnancy perinatal outcomes, while uncontrolled PGDM carries perinatal mortality rates several times above baseline.
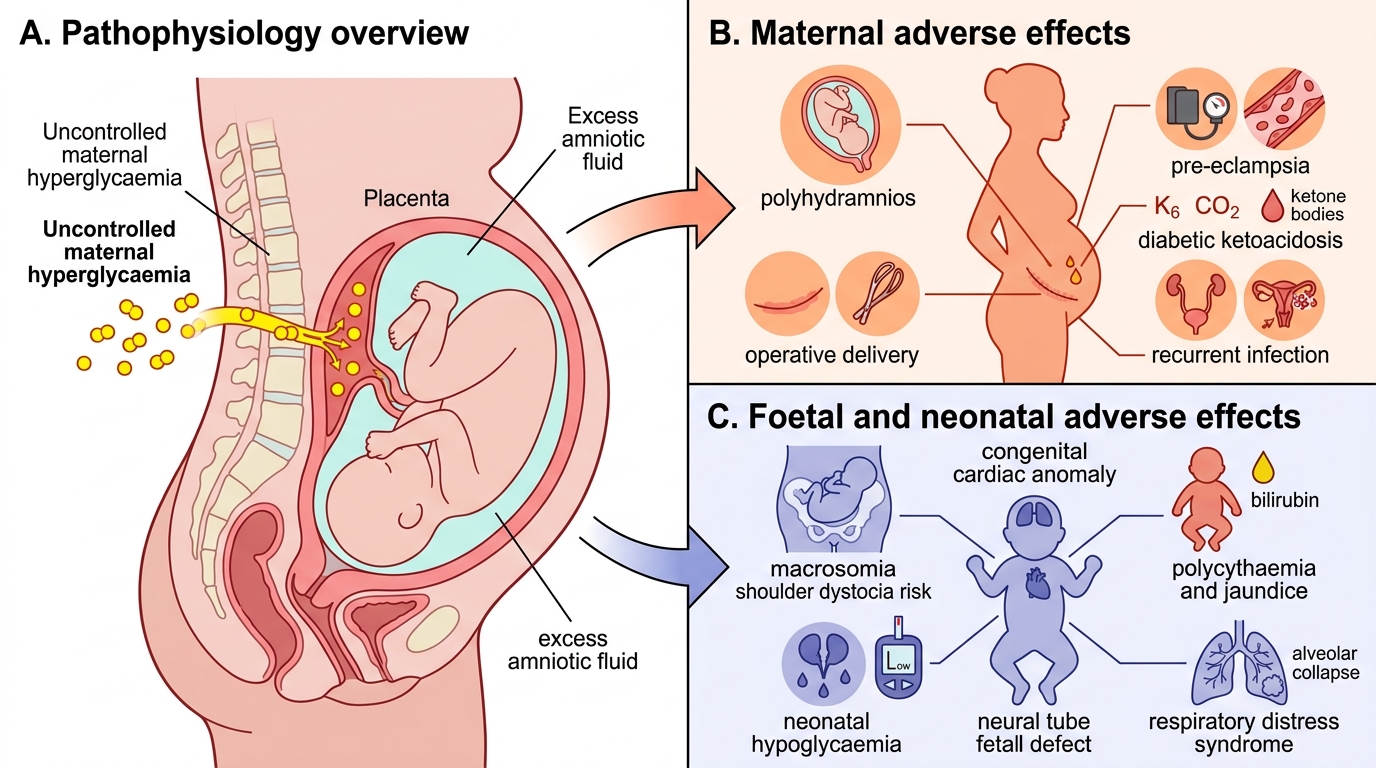
Adverse Effects of Uncontrolled Diabetes in Pregnancy
Maternal adverse effects:
| Complication | Mechanism | Notes |
|---|---|---|
| Polyhydramnios | Foetal polyuria (osmotic diuresis from foetal hyperglycaemia) | AFI >24 cm; risk of cord prolapse, preterm labour |
| Pre-eclampsia | Endothelial dysfunction, insulin resistance | 2–4× risk increase in GDM; higher in PGDM with nephropathy |
| Operative delivery | Macrosomia → CPD, or obstetric indication | Caesarean section rate 2–3× higher in GDM |
| Preterm labour | Polyhydramnios, uterine overdistension | |
| Recurrent infections | Glucosuria, impaired neutrophil function | UTI, vulvovaginal candidiasis, wound infections |
| Diabetic ketoacidosis (DKA) | Occurs at lower glucose thresholds in pregnancy (euglycaemic DKA) | Foetal mortality up to 50% in DKA; requires ICU management |
| Worsening retinopathy | Rapid glucose lowering early in pregnancy; increased retinal blood flow | Regular fundal checks mandatory |
| Future T2DM | Beta-cell exhaustion; ongoing insulin resistance | 50–70% of GDM women develop T2DM within 10 years |
Foetal and neonatal adverse effects:
| Complication | Mechanism | Notes |
|---|---|---|
| Macrosomia | Foetal hyperinsulinaemia (growth factor effect) | BW >4 kg or >90th centile; risk of shoulder dystocia, birth trauma |
| Shoulder dystocia | Excessive foetal trunk and shoulder growth relative to head | Obstetric emergency; risk of brachial plexus injury, Erb's palsy |
| Congenital anomalies | Hyperglycaemia-induced free radicals during organogenesis (wks 3–8) | Mainly PGDM; cardiac (VSD, TGA), neural tube, caudal regression syndrome |
| Neonatal hypoglycaemia | Persistent foetal hyperinsulinaemia at birth without maternal glucose | <2.6 mmol/L; requires early feeding and glucose monitoring |
| Respiratory distress syndrome | Insulin suppresses surfactant synthesis | Even at term; more common before 38 weeks |
| Polycythaemia | Foetal hypoxia stimulates erythropoiesis | Haematocrit >65%; risk of hyperviscosity, neonatal jaundice |
| Neonatal jaundice | Polycythaemia + haemolysis + immature liver conjugation | |
| IUGR | In PGDM with vasculopathy/nephropathy reducing uteroplacental flow | Paradoxical — small for gestational age rather than macrosomic |
| Perinatal mortality | Stillbirth (chronic hypoxia, DKA) and neonatal death | 3–5× baseline in poorly controlled PGDM |
SELF-CHECK
A woman with Type 1 DM has her HbA1c measured at preconception counselling: it is 9.8%. She asks when she can start trying to conceive. The best advice is:
A. She can conceive immediately; HbA1c will improve in pregnancy
B. She should wait until HbA1c is optimised below 6.5% before conception
C. HbA1c above 8% is acceptable in pregnancy; conception may proceed
D. She should switch all insulin to oral metformin before conception
Reveal Answer
Answer: B. She should wait until HbA1c is optimised below 6.5% before conception
The target HbA1c before conception in pre-gestational DM is below 6.5% (ideally below 6.0%). An HbA1c of 9.8% is associated with a greatly increased risk of congenital anomalies — the teratogenic window is weeks 3–8 of embryogenesis, before most women know they are pregnant. She must achieve good glycaemic control before conception. Metformin may be used as adjunct in T2DM preconceptionally, but insulin is not replaced by metformin in T1DM (absolute insulin deficiency).
Management During Pregnancy and Labour
The management of diabetes in pregnancy is a coordinated, multidisciplinary effort spanning the preconception period through to postpartum reclassification. It requires the obstetrician, diabetologist, dietitian, ophthalmologist, neonatologist, and — where available — a diabetes specialist nurse to work as a team, with the pregnant woman as the active participant monitoring her own glucose at home. The overarching goal is restoration of euglycaemia: in GDM, this means preventing foetal hyperinsulinaemia and macrosomia; in PGDM, it means that goal plus protecting the mother from worsening microvascular complications and preventing the congenital anomalies that cluster in the first trimester. The management framework described below moves sequentially through diet, pharmacotherapy, foetal surveillance, intrapartum management, and postpartum follow-up — each step building on the previous. For GDM, the goal is to restore euglycaemia sufficient to eliminate foetal hyperinsulinaemia and prevent macrosomia; for PGDM, the goal is tighter control throughout with careful surveillance for complications. The management framework encompasses dietary modification, pharmacological therapy, foetal monitoring, timing and mode of delivery, intrapartum glucose management, and postpartum care.
A. Dietary Modification (first-line for GDM)
All women with GDM should receive structured medical nutrition therapy (MNT) from a dietitian:
- Caloric distribution: 40–45% carbohydrates (complex, low-glycaemic index), 30–35% fat (predominantly unsaturated), 20–25% protein
- Distribute carbohydrates across 3 meals and 2–3 snacks to blunt postprandial glucose peaks
- Total caloric intake approximately 25–35 kcal/kg of ideal body weight; avoid caloric restriction below 1800 kcal/day in pregnancy
- 2-week dietary trial before pharmacological therapy in women with GDM (unless initial glucose is markedly elevated)
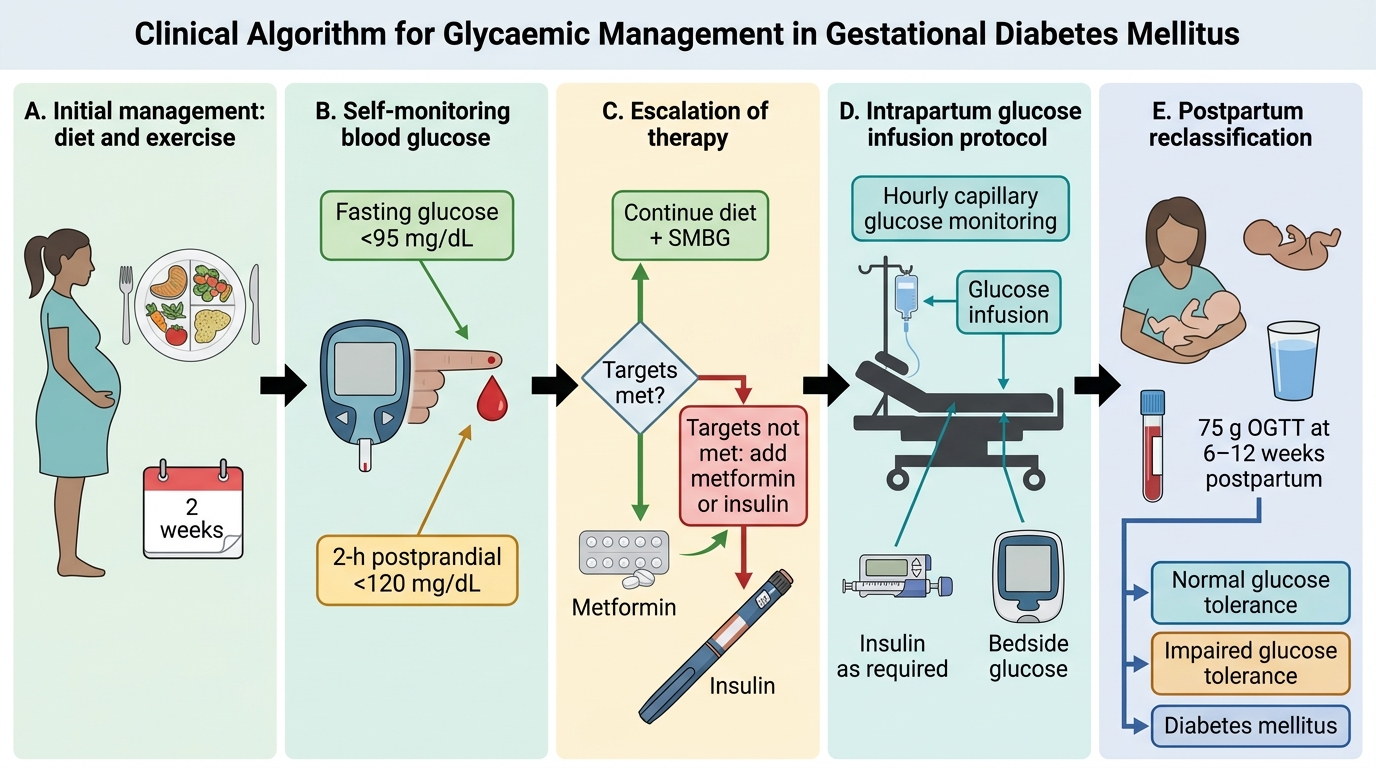
Glycaemic Management Algorithm in Gestational Diabetes
B. Pharmacological Therapy
When dietary modification alone does not achieve SMBG targets (fasting <95 mg/dL, 2-h postprandial <120 mg/dL), pharmacological therapy is introduced:
Metformin:
- First-line oral agent in GDM (used extensively in India under FOGSI guidance)
- Mechanism: reduces hepatic gluconeogenesis, improves peripheral insulin sensitivity
- Crosses the placenta — long-term foetal safety data from MiG trial (Metformin in GDM): no increased short-term neonatal adverse outcomes; some concern about long-term foetal metabolic programming (requires ongoing surveillance)
- Contraindicated in renal impairment (eGFR <30), hepatic failure, DKA, hypoxia
- Up to 50% of women started on metformin for GDM will eventually require supplemental insulin
Insulin:
- Treatment of choice in PGDM; used in GDM when metformin fails or is contraindicated
- Insulin does not cross the placenta and has the longest safety record in pregnancy
- Regimens: multiple daily injections (MDI) — basal-bolus (long-acting analogue such as insulin glargine or detemir + rapid-acting mealtime insulin such as aspart or lispro)
- Glargine safety in pregnancy: FDA category C; widely used in clinical practice with reassuring safety data
- Insulin requirements change throughout pregnancy: relatively stable first trimester, rising substantially from second trimester (peak insulin resistance at 32–36 weeks), then often decreasing after 36–37 weeks
- Hypoglycaemia risk highest in first trimester (when insulin requirements fall and nausea reduces intake)
Oral hypoglycaemics other than metformin are generally avoided in pregnancy (glibenclamide/glyburide — crosses placenta, neonatal hypoglycaemia risk; sulphonylureas generally avoided).
C. Foetal Surveillance (summary of key timing)
- Growth scans at 28, 32, 36 weeks
- Cardiotocography (CTG) from 36 weeks
- Biophysical profile if growth restriction suspected
- Doppler if IUGR or vasculopathy present
D. Timing and Mode of Delivery
- GDM on diet alone: delivery at 40–41 weeks if no other complications; caesarean section only for obstetric indications
- GDM on medication: induction at 38–39 weeks to prevent macrosomia at 40 weeks and avoid risk of stillbirth; caesarean if EFW >4.5 kg on late gestation scan
- PGDM with good control and no complications: 38–39 weeks
- PGDM with complications (vasculopathy, nephropathy): earlier, individualised timing
- Caesarean section is indicated for macrosomic infant (EFW >4.5 kg) to prevent shoulder dystocia
E. Intrapartum Glucose Management
- Target intrapartum glucose: 4–7 mmol/L (72–126 mg/dL) — tight control to prevent neonatal hypoglycaemia
- Women on diet alone (GDM A1): hourly blood glucose monitoring; insulin only if glucose exceeds target
- Women on insulin: Glucose-Insulin-Potassium (GIK) infusion regimen (dextrose 5% + insulin infusion + potassium, titrated to hourly blood glucose targets)
- Insulin requirements fall sharply after delivery of the placenta (removal of the diabetogenic hormones)
- Neonatal team should be present at delivery for monitoring and management of neonatal hypoglycaemia
F. Postpartum Management
- In GDM: stop insulin/metformin immediately after delivery (placenta removed → insulin resistance resolves rapidly)
- Encourage breastfeeding (reduces long-term T2DM risk in both mother and child)
- Postpartum reclassification: 75 g fasting OGTT at 6–12 weeks postpartum in ALL women with GDM:
- Normal: fasting <100 mg/dL AND 2-h <140 mg/dL
- Impaired fasting glucose or impaired glucose tolerance: heightened T2DM risk — lifestyle modification and annual monitoring
- Diabetes: T2DM confirmed; refer to diabetologist
- Long-term: 50–70% of women with GDM develop T2DM within 10 years; counsel on diet, exercise, and annual glucose monitoring
CLINICAL PEARL
The single most commonly tested factual trap in diabetes in pregnancy examinations is the DIPSI vs IADPSG protocol confusion. Remember: DIPSI = non-fasting, single 2-h sample, cut-off ≥140 mg/dL (Indian protocol, FOGSI-endorsed); IADPSG = fasting OGTT, THREE time points (fasting/1-h/2-h), cut-offs 92/180/153 mg/dL (international, WHO-adopted, any ONE positive = GDM). The 2-h IADPSG threshold is 153 mg/dL — higher than DIPSI's 140 — so the same 145 mg/dL value would be POSITIVE under DIPSI but NEGATIVE under IADPSG. Never merge these protocols or apply one protocol's threshold to the other's test conditions.
SELF-CHECK
Which of the following correctly states the IADPSG/WHO-2013 diagnostic criteria for GDM?
A. 75 g non-fasting glucose; 2-hour plasma glucose ≥140 mg/dL
B. 100 g fasting glucose; three thresholds — fasting ≥95, 1-h ≥180, 2-h ≥155 mg/dL (two or more needed)
C. 75 g fasting OGTT; any one of fasting ≥92, 1-h ≥180, 2-h ≥153 mg/dL
D. 75 g fasting OGTT; 2-hour value ≥140 mg/dL only
Reveal Answer
Answer: C. 75 g fasting OGTT; any one of fasting ≥92, 1-h ≥180, 2-h ≥153 mg/dL
The IADPSG/WHO-2013 criteria require a 75 g ORAL glucose load administered in the fasting state, with plasma glucose measured at three time points: fasting (0 min), 1 hour, and 2 hours. GDM is diagnosed if ANY ONE of the following is met: fasting ≥92 mg/dL, 1-h ≥180 mg/dL, or 2-h ≥153 mg/dL. Option A describes DIPSI (non-fasting, 2-h only). Option B describes the older Carpenter-Coustan criteria (100 g, two positives needed). Option D conflates the IADPSG test conditions with a DIPSI-style threshold.
Self-Assessment
This section allows you to consolidate the key clinical knowledge from this module before you encounter diabetes in pregnancy at the bedside or in examinations. The topics covered here — classification of diabetes in pregnancy, the DIPSI and IADPSG protocols with their exact thresholds, the pathophysiology linking maternal hyperglycaemia to foetal outcomes, and the management algorithm from diet through to postpartum reclassification — form a tightly integrated clinical framework. You should be able to apply each component to a novel clinical vignette without confusion between protocols or threshold values. The most reliably tested examination points are the precise DIPSI and IADPSG thresholds, the insulin vs metformin choice in different clinical contexts, the intrapartum glucose target, and the mandatory postpartum reclassification timeline and method. The most common knowledge gaps in this topic — consistently identified in viva voce examinations and clinical skill assessments — are: (1) incorrect or merged DIPSI and IADPSG thresholds; (2) incorrect intrapartum glucose targets; (3) incomplete recall of the foetal consequences of hyperinsulinaemia; and (4) omission of postpartum reclassification. Work through the final micro-quiz question below to check your recall, then review the summary for any gaps.
Key thresholds and protocols to remember:
• DIPSI: 75 g NON-fasting glucose; 2-h ≥140 mg/dL = GDM
• IADPSG/WHO-2013: 75 g FASTING OGTT; fasting ≥92 OR 1-h ≥180 OR 2-h ≥153 mg/dL (any one)
• SMBG targets: fasting <95 mg/dL, 2-h postprandial <120 mg/dL
• Intrapartum target: 4–7 mmol/L (72–126 mg/dL)
• Postpartum: 75 g OGTT at 6–12 weeks to reclassify
• Preconception HbA1c target in PGDM: <6.5%
• Insulin does NOT cross the placenta; metformin DOES