Page 11 of 38
OG12.4 | Heart Disease in Pregnancy — SDL Guide (Part 2)
Adverse Effects on Mother and Foetus
The adverse outcomes of cardiac disease in pregnancy depend critically on the NYHA functional class, the specific valvular or myocardial lesion, the presence or absence of pulmonary hypertension, and the quality of the multidisciplinary management received. A woman with NYHA Class I mitral regurgitation managed in a tertiary centre has an excellent prognosis approaching that of a normal pregnancy; a woman with NYHA Class IV mitral stenosis and pulmonary oedema presenting in labour at a district hospital without cardiac backup has a mortality risk of 15% or higher. This enormous range in outcome emphasises that risk stratification — assigning each woman to her appropriate level of care early in pregnancy — is the single most important clinical intervention. The adverse effects detailed below are therefore not inevitable consequences of cardiac disease in pregnancy, but rather the consequences of undertreated or unrecognised disease, or of disease severe enough that even optimal management cannot prevent morbidity., the specific lesion, the presence of pulmonary hypertension, and the quality of multidisciplinary management. Stratifying these risks — rather than treating all cardiac disease in pregnancy identically — is the clinical skill this section develops.
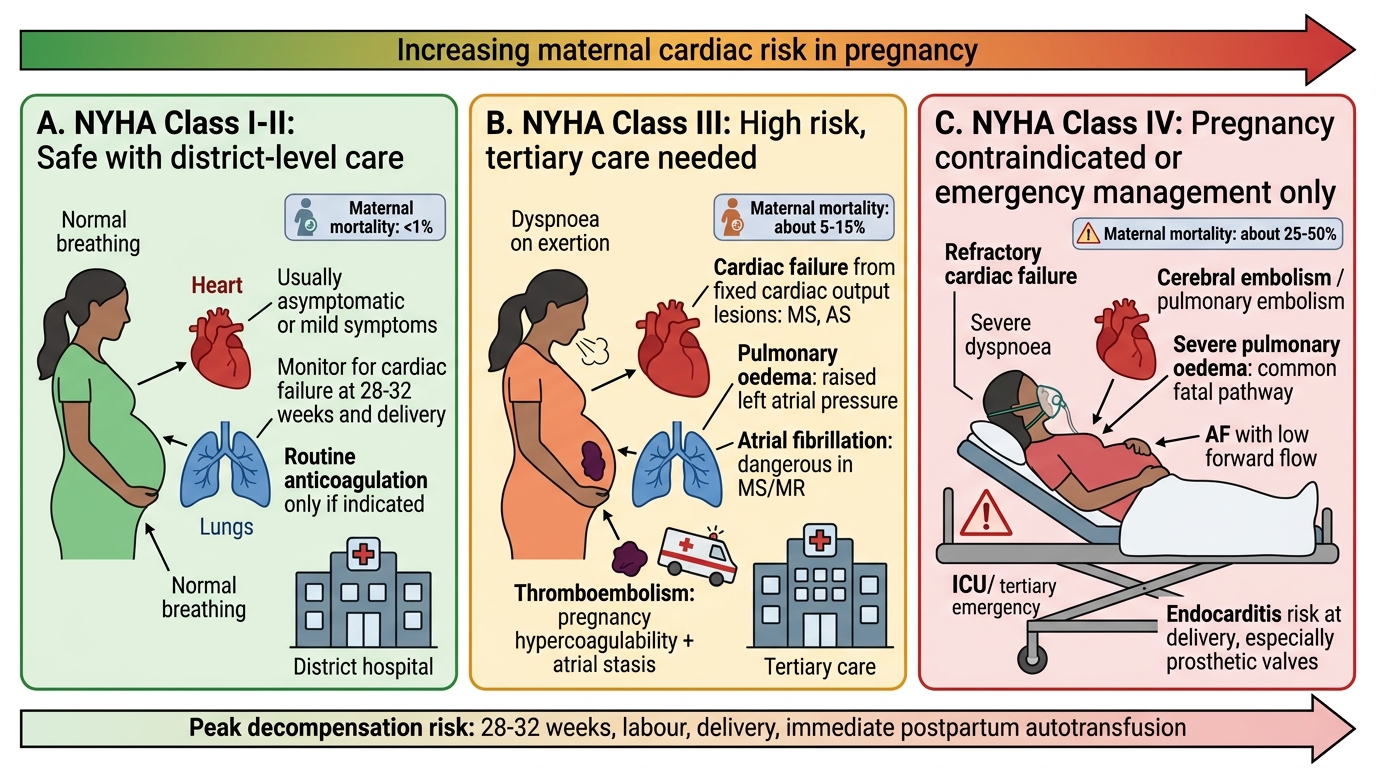
NYHA Functional Class and Maternal Risk in Pregnancy
Maternal adverse effects:
| Complication | Mechanism and lesions at risk |
|---|---|
| Cardiac failure | Fixed cardiac output (MS, AS) cannot accommodate pregnancy demands; decompensation at 28–32 weeks (peak CO) and at delivery (autotransfusion effect) |
| Pulmonary oedema | Elevated left atrial pressure (MS, severe MR, PPCM); most common cause of maternal cardiac death in India |
| Atrial fibrillation | Left atrial dilatation in MS/MR; highly dangerous in MS (reduces forward flow) |
| Thromboembolic events | Hypercoagulable state of pregnancy + atrial stasis (AF, dilated chambers); left atrial thrombus, cerebral embolism, pulmonary embolism |
| Endocarditis | Bacteraemia risk at delivery; rheumatic and congenital lesions at risk; fatal if prosthetic valve involved |
| Maternal mortality | NYHA I/II: <1%; NYHA III: 5–15%; NYHA IV: up to 25%; Eisenmenger: 30–50%; unrecognised/unmanaged lesions carry highest risk |
| Worsening of underlying disease | Pregnancy may accelerate progressive valve disease; PPCM may not fully recover between pregnancies |
| Caesarean section complications | High risk of haemorrhage, PE, cardiac decompensation under general anaesthesia; elective caesarean chosen selectively |
Foetal and neonatal adverse effects:
| Complication | Mechanism | Notes |
|---|---|---|
| IUGR | Reduced uteroplacental blood flow (low cardiac output, medications such as beta-blockers) | Risk proportional to severity of maternal disease |
| Preterm birth | Iatrogenic (early delivery for maternal cardiac deterioration) or spontaneous | |
| LBW / Small for gestational age | IUGR + preterm combined | |
| Foetal cardiac anomaly | Offspring of CHD mothers: 3–5% risk of congenital heart disease (vs 1% background); HOCM is autosomal dominant | Anomaly scan + foetal echocardiography recommended |
| Neonatal bradycardia | Maternal beta-blocker therapy crosses placenta | Neonatal team must be prepared |
| Perinatal mortality | Highest in NYHA III/IV and cyanotic heart disease (foetal hypoxia) |
The CARPREG score (Canadian Cardiovascular Obstetric Network) is a validated tool to predict adverse cardiac events in pregnancy. Predictors include: prior cardiac event (heart failure, TIA, arrhythmia); NYHA class >II; left heart obstruction (MVA <2 cm²); reduced ejection fraction (<40%). Higher CARPREG scores predict higher rates of maternal cardiac events, guiding intensity of monitoring and care.
SELF-CHECK
A 26-year-old woman with mitral stenosis (mitral valve area 1.3 cm², NYHA Class II) is 20 weeks pregnant. Which of the following is an absolute contraindication to continuing this pregnancy?
A. Mitral stenosis with MVA 1.3 cm²
B. Eisenmenger syndrome with right-to-left shunting
C. NYHA Class II with mild exertional breathlessness
D. Rheumatic aortic regurgitation
Reveal Answer
Answer: B. Eisenmenger syndrome with right-to-left shunting
Eisenmenger syndrome — pulmonary hypertension with reversed (right-to-left) shunting — carries a maternal mortality of 30–50% in pregnancy and is classified as mWHO IV (absolute contraindication to pregnancy). The haemodynamic changes of pregnancy (fall in SVR) increase right-to-left shunting and worsen hypoxaemia, while the increased cardiac output cannot be accommodated through the high-resistance pulmonary circulation. MS with MVA 1.3 cm² is moderate stenosis but may be managed in pregnancy; Eisenmenger cannot.
Management During Pregnancy and Labour
The management of heart disease in pregnancy requires a structured multidisciplinary approach that is calibrated to the specific lesion, its severity, and the gestational stage. The core principle is anticipation — the obstetrician and cardiologist must identify the highest-risk moments in the pregnancy (the 28–32 week peak cardiac output, the intrapartum autotransfusion surge, and the 24–48 hour postpartum fluid mobilisation) and have protocols in place before each of these windows arrives. Management is not reactive; it is a structured plan co-authored by the obstetric and cardiac teams at booking or preconception, updated at each antenatal visit, and executed by a coordinated team at delivery. The sequence of management below covers the preconception, antenatal, intrapartum, and postpartum phases, with specific attention to pharmacological choices that are critical in cardiac disease — particularly the drugs that are contraindicated and the physiological reasons why. that begins — ideally — before conception and continues through to the postpartum period. The core team includes the obstetrician, cardiologist (or cardiothoracic surgeon for structural lesions), anaesthetist, and neonatologist; in complex cases, input from haematology (anticoagulation), cardiac surgery (for closed or open mitral valvotomy), and intensive care medicine is required. Every management decision is governed by the principle of balancing maternal cardiac stability with foetal wellbeing.
A. Preconception Counselling
All women with known cardiac disease should receive preconception counselling that covers:
- Risk of maternal mortality and morbidity specific to their lesion and NYHA class
- Expected deterioration in functional class during pregnancy
- Foetal risk (CHD in offspring, IUGR, preterm birth)
- For women with mWHO IV lesions (Eisenmenger syndrome, severely impaired EF, NYHA IV, Marfan syndrome with aortic root >4.5 cm): advise against pregnancy; if pregnant, counsel on termination option
- Anticoagulation management plan (especially for prosthetic heart valves)
- Optimise cardiac function before conception (NYHA class improvement, valvotomy if appropriate)
B. Antenatal Management
- Increased antenatal visit frequency: every 2 weeks in NYHA I–II; weekly or more frequent in NYHA III–IV
- Multidisciplinary team (MDT) approach: joint obstetric-cardiology clinic if available
- Activity restriction: bed rest for NYHA III; hospital admission for NYHA IV or deterioration
- Medications:
- Diuretics: frusemide for pulmonary oedema — safe in pregnancy but monitor for electrolyte disturbance
- Beta-blockers (metoprolol, atenolol): rate control in AF and MS; reduce fetal HR — monitor neonatal bradycardia
- Digoxin: ventricular rate control in AF; safe in pregnancy
- Anticoagulation in AF / prosthetic valves: warfarin is teratogenic in the first trimester; heparin (LMWH or UFH) used in the first trimester and from 36 weeks; warfarin used in second trimester if valvular risk is very high (mechanical prosthetic valve); discuss risks fully with the patient
- ACE inhibitors and ARBs: CONTRAINDICATED in pregnancy (foetal renal dysplasia, oligohydramnios)
- Rheumatic fever prophylaxis: benzathine penicillin 1.2 MU IM every 3–4 weeks throughout pregnancy (prevents new streptococcal episodes worsening RHD)
- Percutaneous mitral valvotomy (balloon mitral valvuloplasty): can be performed in the second trimester for severe MS (MVA <1.5 cm²) refractory to medical management; performed under fluoroscopy (minimum radiation exposure, lead shielding)

Intrapartum Management of Heart Disease in Pregnancy
C. Timing and Mode of Delivery
- NYHA I–II (stable): allow labour to reach term (38–40 weeks); vaginal delivery preferred
- NYHA III–IV or deteriorating: planned delivery at 36–38 weeks at a tertiary centre with cardiac surgical backup
- Mode of delivery: vaginal delivery is haemodynamically preferable to caesarean section in most cardiac disease because it avoids the haemodynamic instability of general anaesthesia and the blood loss and fluid shifts of major surgery; caesarean reserved for obstetric indications or selected high-risk cardiac conditions (severe aortic stenosis, Marfan with aortic dissection risk, PPCM with severely impaired EF)
- Assisted second stage: instrumental delivery (forceps or vacuum) to shorten and reduce the Valsalva effort of the second stage, which increases intrathoracic pressure and impairs venous return
D. Intrapartum Management
- Cardiac monitoring throughout labour: SpO₂, continuous ECG, blood pressure
- Position: left lateral to avoid aortocaval compression
- Fluid management: strict input/output charting; avoid fluid overload (risk of pulmonary oedema in MS, PPCM)
- Analgesia: epidural preferred for pain relief in most cardiac conditions (reduces sympathetic response, lowers BP — monitor for hypotension in severe AS); opioids used with caution (respiratory depression)
- Antibiotic prophylaxis for subacute bacterial endocarditis (SBE): IV antibiotics (amoxicillin + gentamicin) at delivery for moderate-to-high risk lesions
- Oxytocin (for third-stage or PPH): use cautiously in cardiac disease — rapid IV bolus of oxytocin causes vasodilation and reflex tachycardia, which can precipitate collapse in MS or AS; give as slow IV infusion, NOT bolus
- Ergometrine CONTRAINDICATED in cardiac disease — causes severe hypertension and coronary artery spasm
E. Postpartum Management
- The first 24–48 hours postpartum are highest-risk: fluid mobilisation from the uterus and peripheral tissues increases central venous volume by up to 1 L, risking pulmonary oedema in MS and PPCM
- Continue cardiac monitoring in HDU/ICU for at least 24 hours in NYHA III–IV
- Resume anticoagulation early if indicated (AF, prosthetic valve)
- Counsel on future pregnancy risk (if PPCM: avoid subsequent pregnancy until EF normalises; if RHD: advise valvotomy before next pregnancy if MS is severe)
- Contraception: WHO MEC 3/4 conditions apply — COC and high-dose oestrogen-containing methods contraindicated in most significant cardiac disease (thromboembolism risk); progesterone-only methods, IUCD, or sterilisation are safer options
CLINICAL PEARL
The two most commonly missed management points in heart disease in pregnancy examinations are: (1) Ergometrine is absolutely contraindicated — it causes severe vasoconstriction and hypertension that can precipitate acute pulmonary oedema in a patient with mitral stenosis, and coronary artery spasm in ischaemic disease; the only safe oxytocic for the third stage is a slow infusion of oxytocin. (2) The postpartum period is as dangerous as labour — the fluid mobilised from the contracting uterus and oedematous tissues floods the central circulation within 24–48 hours of delivery, creating a new peak of cardiac stress that has claimed lives in women who survived labour safely with MS or PPCM. HDU-level monitoring for at least 24–48 hours postpartum is mandatory in NYHA III–IV.
SELF-CHECK
In a woman with severe mitral stenosis who delivers vaginally, which uterotonic agent is used for active management of the third stage?
A. Ergometrine 0.5 mg IV bolus
B. Carboprost 250 mcg IM
C. Oxytocin 10 IU as a slow IV infusion
D. Misoprostol 400 mcg oral
Reveal Answer
Answer: C. Oxytocin 10 IU as a slow IV infusion
Ergometrine is absolutely contraindicated in significant cardiac disease — it causes vasoconstriction and hypertension that can precipitate acute pulmonary oedema in mitral stenosis. Oxytocin is the uterotonic of choice but must be administered as a SLOW IV infusion (NOT as a rapid IV bolus), as a rapid bolus causes vasodilation and reflex tachycardia that can also be hazardous in MS. Carboprost (PGF2α) is used for PPH but can cause bronchospasm and should be used cautiously; it is not first-line for AMTSL in cardiac disease.
Self-Assessment
Having completed this module, you should be able to navigate the full clinical spectrum of heart disease in pregnancy — from recognising the warning signs that distinguish pathological cardiac symptoms from normal physiological adaptation, through classifying the specific lesion and applying NYHA grading, to selecting the appropriate management pathway and anticipating the critical intrapartum and postpartum hazards. The examination questions on this topic consistently test the same clinical decision points: the identification of dangerous lesions, the NYHA threshold at which pregnancy is inadvisable, the contraindicated medications, and the intrapartum and postpartum management of cardiac emergencies. These are not arbitrary facts but direct clinical consequences of the haemodynamic principles explored throughout this module, and your ability to reason through them using physiological principles — rather than memorisation alone — will serve you far better in both examinations and clinical practice. of heart disease in pregnancy — from recognising the warning signs that distinguish pathological from physiological symptoms, through classifying the lesion and applying NYHA grading, to selecting the appropriate management pathway and anticipating the critical intrapartum and postpartum hazards. The knowledge tested in examinations and in clinical practice focuses particularly on the dangerous lesions (mitral stenosis with AF, Eisenmenger syndrome), the contraindicated drugs (ergometrine, ACE inhibitors), and the NYHA classification applied to pregnancy management decisions. These are not arbitrary facts but the direct clinical consequences of the haemodynamic principles explored in this module.
Key facts to have immediately accessible:
• Most common cause of heart disease in pregnancy in India: rheumatic mitral stenosis
• Most dangerous valvular lesion: mitral stenosis (fixed obstruction, cannot accommodate increased CO demands)
• Absolute contraindication to pregnancy: Eisenmenger syndrome (maternal mortality 30–50%)
• NYHA III/IV: maternal mortality 5–15%; hospital care at tertiary centre mandatory
• Contraindicated uterotonics: ergometrine (hypertension/vasospasm) — use slow oxytocin infusion instead
• Contraindicated antihypertensives: ACE inhibitors and ARBs in pregnancy (foetal renal toxicity)
• Anticoagulation strategy: LMWH in first trimester and after 36 weeks; warfarin acceptable second trimester for high-risk mechanical valves
• Postpartum risk window: first 24–48 hours (fluid mobilisation) — do NOT discharge early