Page 2 of 38
OG12.1 | Hypertensive Disorders of Pregnancy — SDL Guide (Part 2)
Management: Antihypertensives, MgSO4, and Definitive Delivery
The management of hypertensive disorders of pregnancy rests on four interlocking pillars: (1) lowering blood pressure to prevent maternal end-organ damage; (2) preventing and treating convulsions with magnesium sulphate; (3) supporting fetal wellbeing through surveillance and timed delivery; and (4) preventing recurrence in future pregnancies through antenatal risk stratification and prophylaxis. It is essential to internalise that delivery of the placenta is the only definitive treatment for pre-eclampsia — all other interventions are temporising measures to stabilise the mother and optimise the fetus before delivery.
1. Antihypertensive therapy
Antihypertensive treatment is indicated urgently (within 30–60 minutes) when BP reaches the severe-feature threshold of ≥160/110 mmHg, to reduce the risk of maternal stroke, hypertensive encephalopathy, and placental abruption. For sustained BP between 140–159/90–109 mmHg (without severe features), the evidence for acute treatment is less definitive, but most guidelines recommend treatment to reduce the risk of progression.
For acute severe hypertension (BP ≥160/110), the antihypertensives of choice are:
- Labetalol (combined α- and β-blocker): 20 mg IV bolus; may repeat with 40 mg, then 80 mg at 10-minute intervals up to a maximum of 300 mg cumulative dose; or 200 mg orally if IV access is unavailable. Once controlled, transition to oral labetalol. Contraindicated in asthma and heart failure.
- Hydralazine: 5 mg IV bolus, repeat 5 mg at 20-minute intervals; maximum 20 mg per episode. Acts by direct arteriolar vasodilation. Associated with reflex tachycardia and maternal hypotension — use with caution and hydrate the patient before administration.
- Oral nifedipine (short-acting calcium channel blocker): 10–20 mg orally; repeat after 30 minutes if required; maximum 30 mg in the first hour. Highly effective and widely available in Indian settings. Do NOT use sublingual nifedipine (risk of precipitous hypotension and fetal distress). There is a theoretical concern about interaction with MgSO4 (both cause vasodilation and neuromuscular blockade) but clinical experience suggests combined use is acceptable with close monitoring.
For maintenance oral antihypertensive therapy, options include labetalol 100–400 mg 8-hourly, methyldopa 250–500 mg 6–8-hourly (safe in pregnancy, first-line in some Indian guidelines), and nifedipine slow-release 10–20 mg 12-hourly. ACE inhibitors and ARBs are contraindicated in pregnancy due to fetotoxicity (oligohydramnios, renal agenesis, skull ossification defects). Beta-blockers should be used cautiously due to potential fetal growth restriction with prolonged use, but labetalol at standard doses is considered safe.
2. Magnesium sulphate (MgSO4): seizure prophylaxis and treatment
Magnesium sulphate is the drug of choice for both the prevention of eclampsia in women with severe pre-eclampsia and for the treatment of eclamptic convulsions. Its superiority over diazepam and phenytoin in eclampsia management is established by the landmark MAGPIE trial (Magnesium sulphate for Prevention of Eclampsia), which demonstrated a 58% reduction in eclampsia risk. The mechanism of action is multifactorial: MgSO4 acts as a cerebral vasodilator (reversing vasospasm), a NMDA-receptor antagonist (anticonvulsant effect), and a membrane stabiliser, but does NOT act through an antihypertensive mechanism.
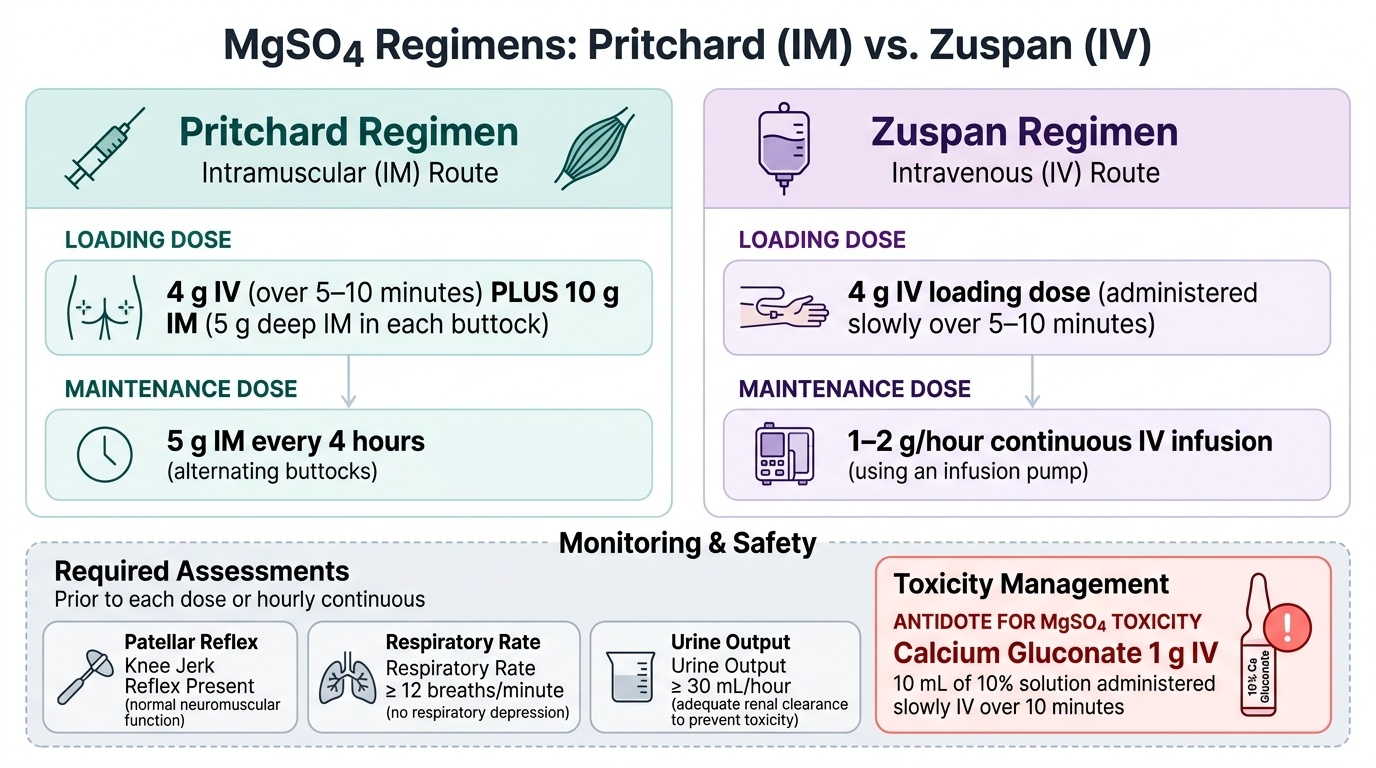
Two regimens are used in clinical practice:
Pritchard regimen (intramuscular / IM — the standard regimen in India per FOGSI/ICMR/NHM guidelines):
- Loading dose: 4 g of MgSO4 (20% solution, 20 mL) administered slowly IV over 5–15 minutes, PLUS 10 g IM (5 g deep IM into each buttock, using 50% MgSO4 solution — 10 mL each side) simultaneously.
- Maintenance dose: 5 g of MgSO4 (50% solution, 10 mL) deep IM into alternate buttocks every 4 hours, continuing for 24 hours after delivery or 24 hours after the last convulsion (whichever is later).
- Addition of 1 mL of 2% lignocaine to the IM injection sites reduces injection pain.
Zuspan regimen (intravenous / IV — used in well-equipped settings with IV infusion facilities):
- Loading dose: 4 g of MgSO4 (20% solution, 20 mL) IV infusion over 15–20 minutes.
- Maintenance dose: 1 g/hour by continuous IV infusion (prepared as 5 g in 500 mL normal saline or 5% dextrose — i.e., 10 mg/mL — run at 100 mL/hour), continuing for 24 hours after delivery or 24 hours after the last convulsion.
Monitoring for MgSO4 toxicity — MANDATORY before each maintenance dose (Pritchard) or hourly (Zuspan):
| Parameter | Required for safe continuation |
|---|---|
| Patellar (knee) jerk reflex | MUST be present (absent = early sign of toxicity; holds at 7–10 mEq/L) |
| Respiratory rate | ≥12 breaths/minute (respiratory arrest occurs at >12 mEq/L) |
| Urine output | ≥30 mL/hour (Mg excreted renally; oliguria → accumulation → toxicity) |
Withhold maintenance MgSO4 if ANY of these criteria are not met. Serum magnesium level (therapeutic: 4–7 mEq/L; toxic signs: >7–8 mEq/L; respiratory arrest: >12 mEq/L) confirms the clinical assessment when available.
Antidote for MgSO4 toxicity: Calcium gluconate 1 g IV (10 mL of a 10% solution) administered slowly over 10 minutes. Keep it at the bedside of every patient on MgSO4. It acts by competitive antagonism of magnesium at calcium-dependent neuromuscular junctions.
Provided image
3. Eclampsia management
Eclampsia is a medical and obstetric emergency. The immediate priorities follow the sequence: protect the airway, prevent injury, terminate the convulsion, prevent recurrence, lower blood pressure, and plan delivery.
- Position: Lateral decubitus (left or right) to prevent aspiration and relieve aortocaval compression. Padded side-rails if available.
- Airway: Insert an airway/oral sponge; suction secretions. High-flow O2 via face mask.
- Convulsion control: MgSO4 loading dose as above (Pritchard or Zuspan). If convulsion persists after the full loading dose, an additional 2 g MgSO4 IV bolus may be given once. Diazepam 10 mg IV is a second-line option if MgSO4 is unavailable.
- Blood pressure: If BP ≥160/110, commence acute antihypertensive (labetalol, hydralazine, or oral nifedipine) as described above.
- Fetal monitoring: After stabilisation of the mother, fetal heart rate monitoring and assessment for signs of abruption.
- Delivery: Proceed to delivery once the mother is stabilised, regardless of gestational age. Vaginal delivery is preferred if feasible; caesarean section is reserved for obstetric indications or failure to progress. Corticosteroids (betamethasone 12 mg IM × 2 doses, 24 hours apart) should be administered before delivery at <34 weeks for fetal lung maturity — but should not delay delivery in an unstable mother.
Complications of eclampsia and severe pre-eclampsia (clinically significant and exam-relevant):
- Placental abruption — complicates 1–4% of pre-eclampsia cases; look for sudden onset abdominal pain, uterine hypertonus, fetal bradycardia.
- Disseminated intravascular coagulation (DIC) — especially in abruption, HELLP, or fetal demise; monitor coagulation indices.
- Cerebral haemorrhage — the most common cause of death in eclampsia; consequence of uncontrolled hypertension.
- Acute renal failure — from profound vasospasm ± DIC; monitor urine output and creatinine.
- Pulmonary oedema — fluid overload compounded by capillary leak; restrict IV fluids.
- HELLP syndrome — may require platelet transfusion (<20 × 10⁹/L or <50 × 10⁹/L pre-caesarean); dexamethasone has been used to accelerate platelet recovery but evidence is not definitive.
- Retinal detachment — rare; associated with severe hypertension.
IMPORTANT: Ergometrine/methylergometrine is contraindicated in hypertensive disorders of pregnancy for oxytocic purposes because it causes severe vasospasm and can precipitate a hypertensive crisis and stroke. For active management of the third stage in a pre-eclamptic patient, use oxytocin 10 IU IM instead.
4. Prevention
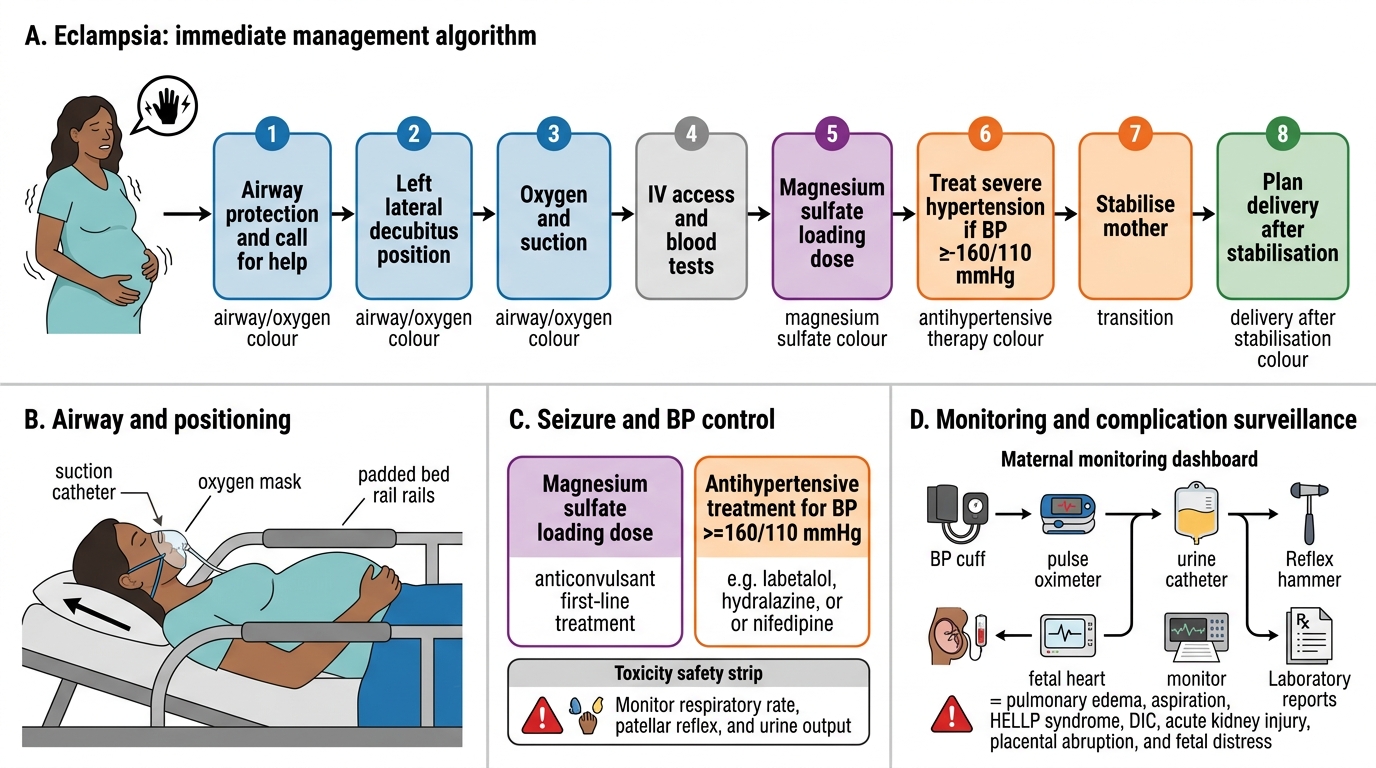
Eclampsia Management Algorithm
- Low-dose aspirin (75–150 mg/day): Recommended in women with ≥1 high-risk factor (previous pre-eclampsia, chronic hypertension, diabetes, renal disease, autoimmune disease, multiple pregnancy) or ≥2 moderate-risk factors. Should be started before 16 weeks of gestation (ideally before 12 weeks) and continued until 36–37 weeks. The ASPRE trial demonstrated a 62% reduction in pre-term pre-eclampsia in screen-positive women treated with 150 mg aspirin from 11–14 weeks.
- Calcium supplementation (1.5–2 g/day elemental calcium): Recommended by WHO and Indian FOGSI/ICMR guidelines in populations with low dietary calcium intake (which includes most of the Indian subcontinent). Calcium lowers blood pressure by reducing smooth muscle contractility and may have a role in trophoblast invasion. Meta-analyses show approximately 50% reduction in the risk of pre-eclampsia with calcium supplementation.
- Other measures: Weight optimisation before pregnancy; management of pre-existing conditions (HTN, diabetes, renal disease, thrombophilia); close antenatal surveillance in high-risk women (BP monitoring, proteinuria testing, serial fetal growth scans).
SELF-CHECK
A patient with eclampsia is started on the Pritchard regimen of magnesium sulphate. After 3 hours, the nursing staff reports that the patellar reflex is absent and the respiratory rate is 10/min. What is the immediate management?
A. Withhold the next maintenance dose only and observe for 30 minutes
B. Administer calcium gluconate 1 g IV (10 mL of 10% solution) immediately and withhold MgSO4
C. Give an additional 2 g MgSO4 IV to achieve therapeutic levels
D. Switch from Pritchard IM to Zuspan IV regimen
Reveal Answer
Answer: B. Administer calcium gluconate 1 g IV (10 mL of 10% solution) immediately and withhold MgSO4
Absent patellar (knee) reflex and respiratory rate below 12/min are signs of MgSO4 toxicity. The monitoring protocol requires ALL THREE parameters (knee jerk present, RR ≥12/min, urine output ≥30 mL/h) to be met before continuing maintenance MgSO4. Absent knee jerk indicates rising serum magnesium levels (typically ≥7 mEq/L); respiratory rate of 10/min is below the safe threshold of 12/min, indicating impending respiratory depression. The immediate action is to WITHHOLD MgSO4 and administer the antidote: CALCIUM GLUCONATE 1 g IV (10 mL of 10% solution), given slowly over 10 minutes. The calcium gluconate should already be at the bedside. Simply withholding the next dose is insufficient when active toxicity signs are present — reversal is required.
Self-Assessment Summary
This module has covered the complete arc of hypertensive disorders of pregnancy from classification and clinical presentation through pathophysiology to diagnosis, investigation, and management. The arc you have traversed reflects the real-world clinical encounter with HDP: a woman presents (arc step 1 — clinical presentation), you understand why her disease behaves as it does (arc step 2 — pathophysiology and the sFlt-1/PlGF axis), you apply the correct thresholds and order the right tests (arc step 3 — diagnosis and investigation), and then you intervene safely with antihypertensives, MgSO4, and planned delivery (arc step 4 — management). The knowledge tested in MBBS examinations, entrance assessments, and ultimately in clinical practice all maps to this arc. The key management facts — the exact MgSO4 doses, the monitoring triad, the antidote, and the contraindicated drugs — must be retrieved automatically and correctly under pressure. Before attempting the final quiz, review the following key self-test points to consolidate your understanding:
Classification:
- The 20-week gestational boundary separates pre-eclampsia and gestational hypertension (post-20 weeks) from chronic hypertension (present before 20 weeks or pre-existing).
- Pre-eclampsia = new-onset BP ≥140/90 mmHg after 20 weeks + proteinuria (≥300 mg/24h or PCR ≥30 mg/mmol or dipstick ≥2+) OR end-organ dysfunction.
- Severe features = BP ≥160/110 mmHg, OR thrombocytopaenia (<100 × 10⁹/L), OR renal insufficiency (creatinine >97 µmol/L), OR impaired LFT (transaminases ×2 normal), OR pulmonary oedema, OR new unresponsive headache/visual disturbance.
- Eclampsia = pre-eclampsia + convulsions. HELLP = haemolysis + elevated liver enzymes + low platelets (<100 × 10⁹/L).
Pathophysiology essentials:
- The primary lesion: defective trophoblast invasion → incomplete spiral-artery remodelling → placental ischaemia.
- The circulating mediator: elevated sFlt-1 neutralises VEGF and PlGF → endothelial dysfunction → vasospasm, proteinuria, thrombocytopaenia, multi-organ damage.
Investigations:
- Mandatory labs: CBC (platelets), LFT (AST/ALT/LDH), RFT (urea/creatinine), uric acid, urine PCR, coagulation screen, blood grouping.
- Fetal surveillance: CTG, obstetric ultrasound (biometry + AFI + placenta), umbilical artery Doppler.
Management: (commit these to memory)
- Acute severe HTN (≥160/110): labetalol IV, hydralazine IV, or oral nifedipine. ACE inhibitors and ARBs are CONTRAINDICATED in pregnancy. Ergometrine/methylergometrine is CONTRAINDICATED in HDP.
- MgSO4 — Pritchard IM regimen: loading 4 g IV + 10 g IM (5 g each buttock); maintenance 5 g IM every 4 h alternate buttocks.
- MgSO4 — Zuspan IV regimen: loading 4 g IV; maintenance 1 g/h infusion.
- MgSO4 monitoring: patellar reflex PRESENT + RR ≥12/min + urine output ≥30 mL/h.
- MgSO4 antidote: calcium gluconate 1 g IV (10 mL of 10% solution).
- Definitive treatment: delivery of the placenta.
- Prevention: low-dose aspirin (75–150 mg/day from <16 weeks) + calcium supplementation (1.5–2 g/day elemental calcium) in high-risk and calcium-deficient populations.
SELF-CHECK
Which statement about low-dose aspirin prophylaxis for pre-eclampsia is CORRECT?
A. It should be started at 28 weeks in all pregnant women regardless of risk
B. It is recommended at 75–150 mg/day started before 16 weeks in women with ≥1 high-risk factor
C. The MAGPIE trial established its efficacy in preventing eclampsia
D. Calcium supplementation is recommended instead of aspirin in Indian guidelines
Reveal Answer
Answer: B. It is recommended at 75–150 mg/day started before 16 weeks in women with ≥1 high-risk factor
Low-dose aspirin (75–150 mg/day) is recommended for pre-eclampsia prevention in women with ≥1 high-risk factor (previous pre-eclampsia, chronic hypertension, diabetes, renal disease, autoimmune disease, multiple pregnancy) or ≥2 moderate-risk factors. The critical timing is initiation BEFORE 16 weeks of gestation (ideally before 12 weeks) — late initiation significantly reduces efficacy. The ASPRE trial (not MAGPIE) established aspirin efficacy; the MAGPIE trial established MgSO4 efficacy in preventing eclampsia. Calcium supplementation (1.5–2 g/day elemental calcium) is also recommended in Indian guidelines for populations with low dietary calcium intake, but it is used IN ADDITION to aspirin in high-risk women, not instead of it. Starting aspirin at 28 weeks is too late to alter the first/second wave of trophoblast invasion.
CLINICAL PEARL
The 'worried obstetrician' rule in HDP: Always beware the eclamptic patient who has 'no warning signs' — up to one-third of eclamptic convulsions occur without preceding severe hypertension or proteinuria, and may even occur postpartum (up to 4–6 weeks after delivery). Any pregnant or recently-delivered woman presenting with a new-onset seizure should be treated as eclampsia until proven otherwise, even if blood pressure was normal at the last check. Similarly, absent or mild proteinuria does not exclude serious pre-eclampsia — HELLP syndrome can present with normal blood pressure in 15–20% of cases. The monitoring mantra — knee jerk, respiratory rate, urine output — must be recited before every MgSO4 maintenance dose. A patient paralysed by unrecognised MgSO4 toxicity because a monitoring check was skipped is a preventable death. Calcium gluconate at the bedside is not optional.