Page 32 of 38
OG12.11,OG16.4 | Intrauterine Growth Retardation — SDL Guide (Part 2)
Management Principles and Timing of Delivery
The management of IUGR requires individualised decision-making that balances two competing risks: the risk of ongoing intrauterine hypoxia and potential fetal death if the pregnancy continues, against the risk of iatrogenic prematurity if delivery is timed too early. No single intervention can treat the underlying placental pathology; the mainstay of management is meticulous fetal surveillance to identify the optimal window for delivery before irreversible fetal compromise.
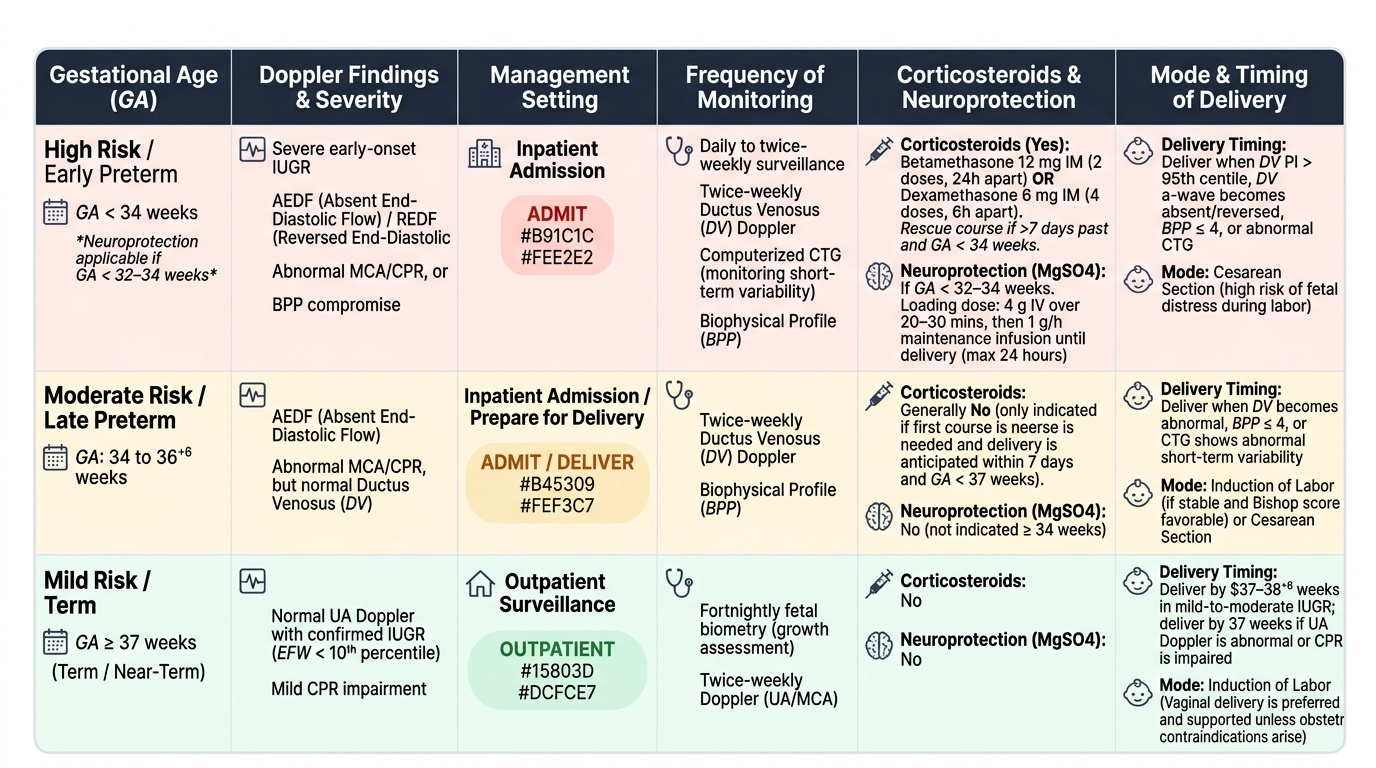
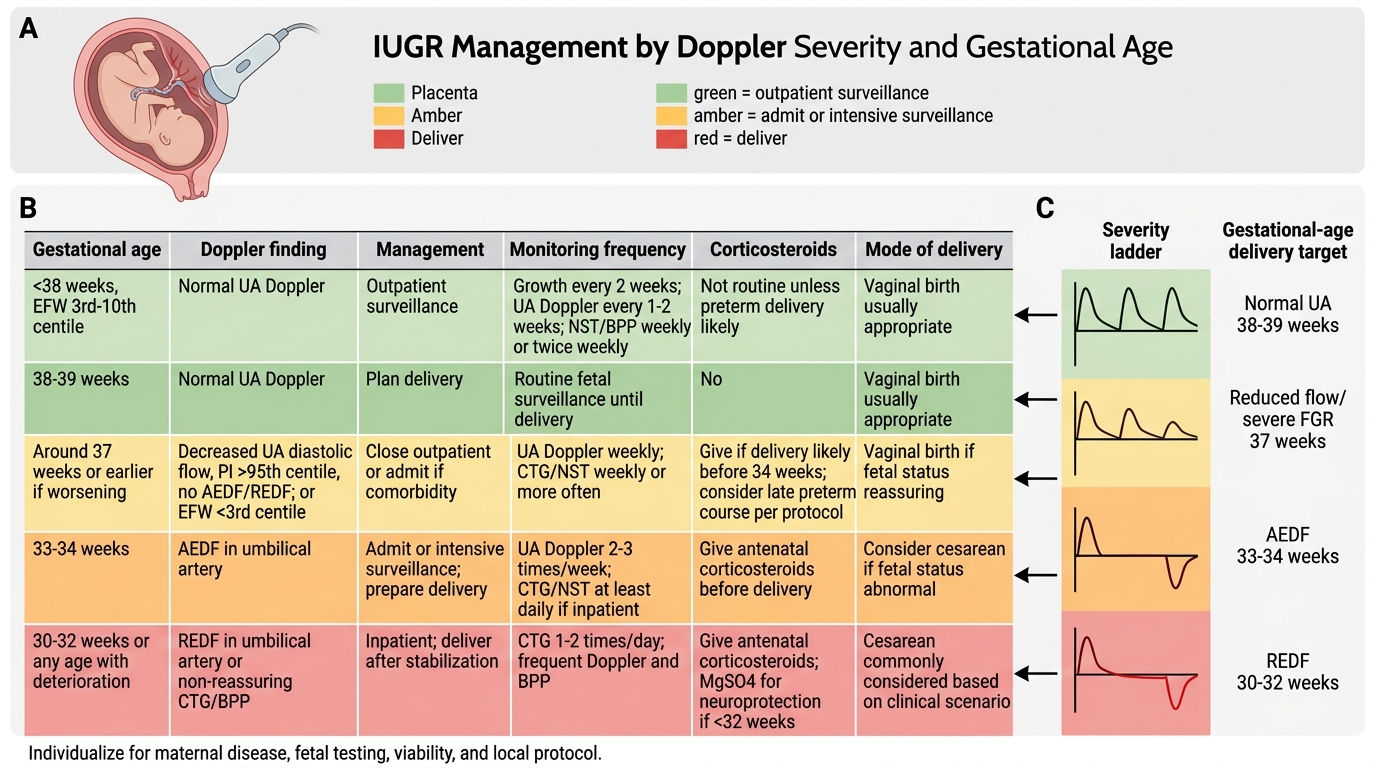
Outpatient versus inpatient management depends on the severity of the Doppler findings. A fetus with normal UA Doppler but confirmed IUGR (EFW <10th centile) may be monitored with fortnightly biometry and twice-weekly Doppler in an outpatient setting. AEDF, abnormal MCA/CPR, or BPP compromise warrants admission for closer and more frequent monitoring.
Corticosteroids (betamethasone 12 mg IM 24 hours apart × 2 doses, or dexamethasone 6 mg IM 6-hourly × 4 doses) are administered when delivery is anticipated before 34 weeks, ideally at least 24 hours before delivery, to accelerate fetal lung maturation and reduce the risk of respiratory distress syndrome, intraventricular haemorrhage, and necrotising enterocolitis. A rescue (repeat) course may be given if the first course was given before 34 weeks and delivery has not occurred within 7 days.
Magnesium sulphate (MgSO4) for neuroprotection: when preterm delivery is anticipated before 32 weeks (some guidelines extend to <34 weeks), MgSO4 is administered to reduce the risk of cerebral palsy. The RCOG regimen is a loading dose of 4 g IV over 20–30 minutes followed by 1 g/h maintenance infusion until delivery (or for a maximum of 24 hours). This is distinct from the eclampsia regimen (Pritchard or Zuspan) — the neuroprotection indication uses the same drug but at lower maintenance doses and for a different purpose.
Delivery timing is guided by gestational age, Doppler findings, and the TRUFFLE trial evidence:
• Term or near-term IUGR (≥37 weeks): deliver by 37–38+6 weeks in mild-to-moderate IUGR; by 37 weeks if UA Doppler is abnormal or CPR is impaired.
• Severe early-onset IUGR (<34 weeks) with AEDF: admit; twice-weekly ductus venosus Doppler + BPP; deliver when DV becomes abnormal (PI >95th centile), DV a-wave becomes absent or reversed, BPP falls to ≤4, or there is CTG evidence of short-term variability loss.
• REDF in the umbilical artery: deliver by 34 weeks; earlier if DV or BPP becomes abnormal. Below 28 weeks, REDF represents an extremely difficult decision — parental counselling about prognosis is mandatory.
• Ductus venosus absent/reversed a-wave: deliver regardless of gestational age if the fetus is viable, after administration of corticosteroids if time allows.
The TRUFFLE trial enrolled 503 early-onset preterm IUGR fetuses (26–32 weeks) and randomised delivery timing to three triggers: CTG short-term variability, DV PI >95th centile, or DV a-wave absent/reversed. The primary outcome was survival without neurodevelopmental impairment at 2 years. The DV a-wave trigger arm achieved the best balance of outcome, forming the basis of current evidence-based practice.
Mode of delivery: there is no absolute rule. Vaginal delivery with continuous electronic fetal monitoring is appropriate in the majority of IUGR fetuses without other obstetric indications for caesarean. However, a fetus with severe IUGR and REDF or DV abnormality has limited physiological reserve and may not tolerate the stress of labour — a decision for caesarean section should be made with the obstetric team and documented. Intrapartum CTG must be interpreted with heightened vigilance; a non-reassuring CTG in a growth-restricted fetus requires expedited delivery.
Neonatal preparation: a neonatologist must be present at delivery; the neonatal team should be briefed pre-delivery. Expected neonatal complications include hypothermia, hypoglycaemia, polycythaemia, respiratory distress syndrome (if preterm), necrotising enterocolitis, and neurodevelopmental delay.
Provided image
IUGR Management by Doppler Severity and Gestational Age
Prevention, Counselling, and Long-Term Implications
While the underlying placental pathology in most cases of IUGR cannot be reversed once established, several preventive and modifiable strategies can reduce recurrence risk and attenuate severity.
Low-dose aspirin (75–150 mg at night) is the most evidence-based pharmacological intervention for prevention of placenta-mediated IUGR. Aspirin inhibits thromboxane synthesis preferentially, reducing platelet-mediated vasoconstriction and placental microthrombus formation. It should be commenced before 16 weeks of gestation (ideally by 12 weeks) in women with high-risk factors: previous pre-eclampsia or IUGR, chronic hypertension, diabetes with vasculopathy, antiphospholipid syndrome, or ≥3 moderate-risk factors (BMI >35, age >40, nulliparity, multiple pregnancy, family history of pre-eclampsia). The ASPRE trial demonstrated that aspirin from 11–14 weeks in women identified as high-risk by first-trimester combined screening reduced preterm pre-eclampsia and IUGR by approximately 62%.
Other preventive measures include optimisation of maternal nutrition (adequate protein and micronutrients — iron, folate, calcium supplementation per national guidelines), smoking cessation (smoking is an independent, strong, dose-dependent cause of IUGR — women who quit before 15 weeks have outcomes approaching non-smokers), treatment of underlying hypertension and thrombophilias, and haematological management of severe anaemia before conception.
Counselling should address: (a) the prognosis for the current pregnancy, including the surveillance plan and what findings would trigger hospitalisation or delivery; (b) the recurrence risk — approximately 20–25% in the next pregnancy, higher if caused by thrombophilia or APS; (c) the plan for pre-conceptional optimisation in future pregnancies (aspirin, specialist review); and (d) the long-term implications for the child. Neonates who were growth-restricted are at elevated risk for learning difficulties, attention deficit disorders, and impaired neurodevelopment, particularly if born preterm.
Barker hypothesis (developmental origins of health and disease): one of the most important long-term implications of IUGR is the programming effect on fetal metabolism. Barker and colleagues demonstrated that undernutrition during critical windows of fetal development permanently alters gene expression and metabolic set-points (epigenetic programming), predisposing the individual to coronary artery disease, hypertension, type 2 diabetes, and metabolic syndrome in adult life — even when nutrition becomes adequate after birth. This relationship was first observed in populations exposed to famine during the Dutch Hunger Winter (1944–45). Counselling should note that although the child's long-term risk is elevated, a healthy postnatal environment — adequate nutrition without excess, physical activity, and no smoking — can substantially attenuate this programmed risk.
CLINICAL PEARL
Three points that distinguish the prepared final-year student in IUGR viva:
- SGA ≠ IUGR: A constitutionally small but well baby (SGA) does not require the same Doppler surveillance protocol as a truly growth-restricted fetus. The distinction is made by the growth velocity and customised chart — a baby that has always plotted at the 8th centile but is growing along that centile is not IUGR; a baby that has dropped from the 40th to the 8th centile over 8 weeks is.
- The Doppler sequence is a progression, not a jump: Doppler deterioration follows a predictable order — UA S/D ratio rises → AEDF → REDF → MCA becomes abnormal (CPR <1) → ductus venosus a-wave disappears/reverses → biophysical profile falls → CTG deteriorates. Knowing this hierarchy allows you to state not just 'what is abnormal' but 'where in the deterioration sequence is this fetus' — the key question in viva.
- MgSO4 for neuroprotection vs eclampsia — same drug, different purpose, different regimen details: the neuroprotection regimen (4 g loading, 1 g/h maintenance, before <32 weeks preterm delivery) is NOT the Pritchard or Zuspan eclampsia regimen — do not confuse them or invent intermediate doses. The antidote is the same (calcium gluconate 1 g IV), but the indication and monitoring context differ.
SELF-CHECK
You counsel a 27-year-old woman at booking who had IUGR at 32 weeks in her last pregnancy (no identified cause). Her BMI is 28 and she is a non-smoker. Which intervention has the strongest evidence for reducing IUGR recurrence if started before 16 weeks?
A. Low-molecular-weight heparin (LMWH) starting at 10 weeks
B. Low-dose aspirin 75–150 mg at night starting by 16 weeks
C. High-dose folic acid supplementation throughout pregnancy
D. Calcium supplementation from 20 weeks
Reveal Answer
Answer: B. Low-dose aspirin 75–150 mg at night starting by 16 weeks
Low-dose aspirin started before 16 weeks (ideally by 12 weeks) has the strongest evidence for prevention of placenta-mediated IUGR in high-risk women. The ASPRE trial showed a 62% reduction in preterm pre-eclampsia and IUGR with early aspirin in first-trimester-screened high-risk women. LMWH has evidence only in confirmed thrombophilia or APS. High-dose folate reduces neural tube defects. Calcium reduces pre-eclampsia in calcium-deficient populations but is not the primary IUGR-prevention strategy.
SELF-CHECK
Which of the following Doppler findings indicates the most severe stage of fetal compromise in IUGR and warrants delivery regardless of gestational age (if viable)?
A. Umbilical artery S/D ratio above the 95th centile for gestational age
B. MCA pulsatility index below the 5th centile
C. Cerebroplacental ratio less than 1.0
D. Ductus venosus absent or reversed a-wave
Reveal Answer
Answer: D. Ductus venosus absent or reversed a-wave
Ductus venosus absent or reversed a-wave is the most ominous finding, reflecting imminent cardiac decompensation and central venous pressure elevation. It is a pre-terminal marker and forms the TRUFFLE trial's most aggressive delivery trigger. UA S/D ratio elevation is an early finding; MCA abnormality and reduced CPR indicate brain-sparing but not immediately pre-terminal status. DV a-wave reversal precedes BPP and CTG deterioration and mandates delivery in a viable fetus.