Page 22 of 38
OG12.8 | Iso-Immunization in Pregnancy — SDL Guide
Learning Objectives
- Explain the mechanism of Rh iso-immunization and why IgG — but not IgM — causes haemolytic disease of the newborn
- Describe the clinical and laboratory investigations used to detect and monitor Rh iso-immunization, including ICT titre, Kleihauer-Betke test, and MCA-PSV Doppler
- State the correct dose, timing, and indications for anti-D immunoglobulin prophylaxis
- Outline the management of established Rh iso-immunization including intrauterine transfusion (IUT) and timing of delivery
- Describe the principles of neonatal management of haemolytic disease of the newborn (HDNB)
INSTRUCTIONS
Rh haemolytic disease of the newborn was once a major cause of perinatal mortality — jaundiced, hydropic babies dying within hours of birth. The discovery of anti-D immunoglobulin prophylaxis and the development of intrauterine transfusion transformed this disease from a common tragedy to a largely preventable condition. Yet iso-immunization still occurs in India due to gaps in prophylaxis coverage, particularly after miscarriage and sensitising events at peripheral facilities. This module equips you with the mechanistic understanding, diagnostic toolkit, and management protocol to both prevent and manage this entirely preventable condition.
References
- DC Dutta's Textbook of Obstetrics, 9th ed., Ch 17 — Isoimmunization in Pregnancy (textbook)
- Williams Obstetrics, 26th ed., Ch 15 — Fetal Haemolytic Disease (textbook)
- RCOG Green-top Guideline No. 65 — The Management of Women with Red Cell Antibodies during Pregnancy (2014) (guideline)
- Oepkes D et al. Doppler ultrasonography versus amniocentesis to predict fetal anemia. NEJM 2006;355:156-164 (journal)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Anita is a 28-year-old gravida 2 para 1 at 26 weeks gestation. Her first pregnancy three years ago ended in a miscarriage at 10 weeks, managed conservatively at a primary health centre. No anti-D was given. Blood typing now shows she is O Rh-negative. Her husband is B Rh-positive. Her indirect Coombs test (ICT) returns positive at a titre of 1:32. The fetal anatomy scan shows the baby is Rh-positive. She is referred to your tertiary centre. Her previous baby (a boy, Rh-positive) was born healthy. What has happened immunologically between her miscarriage and this pregnancy? What surveillance does she need now, and under what circumstances would you consider intrauterine blood transfusion? The answer to these questions will determine whether this baby survives.
WHY THIS MATTERS
Iso-immunization (red cell alloimmunization) remains a clinically relevant condition in India for two reasons: first, anti-D prophylaxis coverage is incomplete — many first-trimester events at peripheral facilities do not trigger anti-D administration, leaving a proportion of Rh-negative women unprotected after their first sensitising event. Second, when iso-immunization is established, fetal surveillance with MCA-PSV Doppler and timely intrauterine transfusion can genuinely save a baby that would otherwise die from hydrops fetalis. Understanding the mechanism, the monitoring protocol, and the prophylaxis rules transforms a potentially tragic situation into a manageable one. As a future clinician, you will order blood grouping on every antenatal woman and make decisions about anti-D administration after every sensitising event — these are not academic exercises.
RECALL
Recall from Immunology that immunoglobulin classes differ in their ability to cross the placenta. IgG (all subclasses) is actively transported across the placenta by the neonatal Fc receptor (FcRn) on trophoblasts from approximately 16 weeks, providing passive immunity to the fetus. IgM is a pentameric molecule too large for this transplacental transport — it remains in the maternal circulation. This difference is the immunological basis of haemolytic disease of the newborn: the IgG secondary immune response produces anti-D that crosses the placenta; the primary IgM response from the first exposure does not. Recall also from Biochemistry that haem released from lysed red cells is processed to bilirubin, which is conjugated in the liver — neonatal unconjugated hyperbilirubinaemia from massive red cell destruction is the mechanism of kernicterus.
Rh-Negative Mother, Rh-Positive Baby — A Clinical Encounter
In clinical practice, iso-immunization is almost always detected asymptomatically — either at booking blood group and antibody screen, or on routine ICT performed in an already-identified Rh-negative woman. The affected baby does not declare itself with dramatic symptoms until the condition is advanced; the mother is typically entirely asymptomatic. This silent presentation makes systematic screening the only reliable way to identify at-risk pregnancies before fetal compromise occurs.
Who is at risk? Approximately 15–17% of Caucasian women are Rh-D negative; the frequency is lower in South Asian and East Asian populations (approximately 5–8% in India). An Rh-negative woman is at risk only if the fetus inherits the paternal D antigen (i.e., the father is D-positive, either homozygous DD or heterozygous Dd). If the father is DD, all offspring are D-positive; if Dd, 50% are positive. Paternal Rh genotyping can determine the probability that the fetus is affected. Fetal Rh genotyping from cell-free fetal DNA in maternal plasma is available in some centres and provides a definitive answer without invasive testing.
The clinical presentation of established iso-immunization varies by severity:
- Unaffected or mildly affected fetus: ICT positive with a low titre (≤1:8); fetus may be Rh-negative (if the father is heterozygous and the fetus inherited the d allele) or mildly affected with subclinical haemolysis; the baby is born with mild anaemia and jaundice — responsive to phototherapy
- Moderately affected fetus: MCA-PSV Doppler >1.5 MoM indicating significant fetal anaemia; fetal hydrops has not yet developed; baby may require exchange transfusion after birth or IUT before 34 weeks
- Hydrops fetalis: the most severe manifestation — generalised fetal oedema (skin oedema, ascites, pleural effusions, pericardial effusion) resulting from severe anaemia causing high-output cardiac failure and hypoalbuminaemia; visualised on ultrasound; carries high perinatal mortality without IUT. Polyhydramnios and fetal cardiomegaly may be present
In the neonate (haemolytic disease of the newborn, HDNB): jaundice appears within 24 hours of birth (distinguishing it from physiological jaundice, which appears after 24 h); pallor, hepatosplenomegaly (from extramedullary haematopoiesis), and in severe cases hydrops. Serum bilirubin rises rapidly and, if untreated, bilirubin deposition in the basal ganglia causes kernicterus (bilirubin encephalopathy) — a preventable cause of cerebral palsy and deafness.
SELF-CHECK
A woman with blood group O Rh-negative delivers an O Rh-positive baby. The cord blood Direct Coombs Test (DCT) is POSITIVE. What does this mean?
A. The mother has anti-D antibodies circulating in her serum
B. Anti-D IgG from the mother has coated the fetal red cells
C. The fetus has produced its own anti-D in response to maternal D antigen
D. The fetal red cells lack D antigen, causing haemolysis
Reveal Answer
Answer: B. Anti-D IgG from the mother has coated the fetal red cells
The Direct Coombs Test (DCT) is performed on the cord/neonatal blood; a positive result means that antibodies (maternal anti-D IgG) are ALREADY BOUND to the fetal red blood cells. This confirms active maternal sensitization has affected the neonate. The Indirect Coombs Test (ICT) is performed on MATERNAL serum to detect circulating (free, unbound) anti-D antibodies — the two tests detect the same immune process at different levels: ICT = antibodies in maternal serum; DCT = antibodies bound to fetal cells.
How Rh Iso-Immunization Develops — Pathophysiology
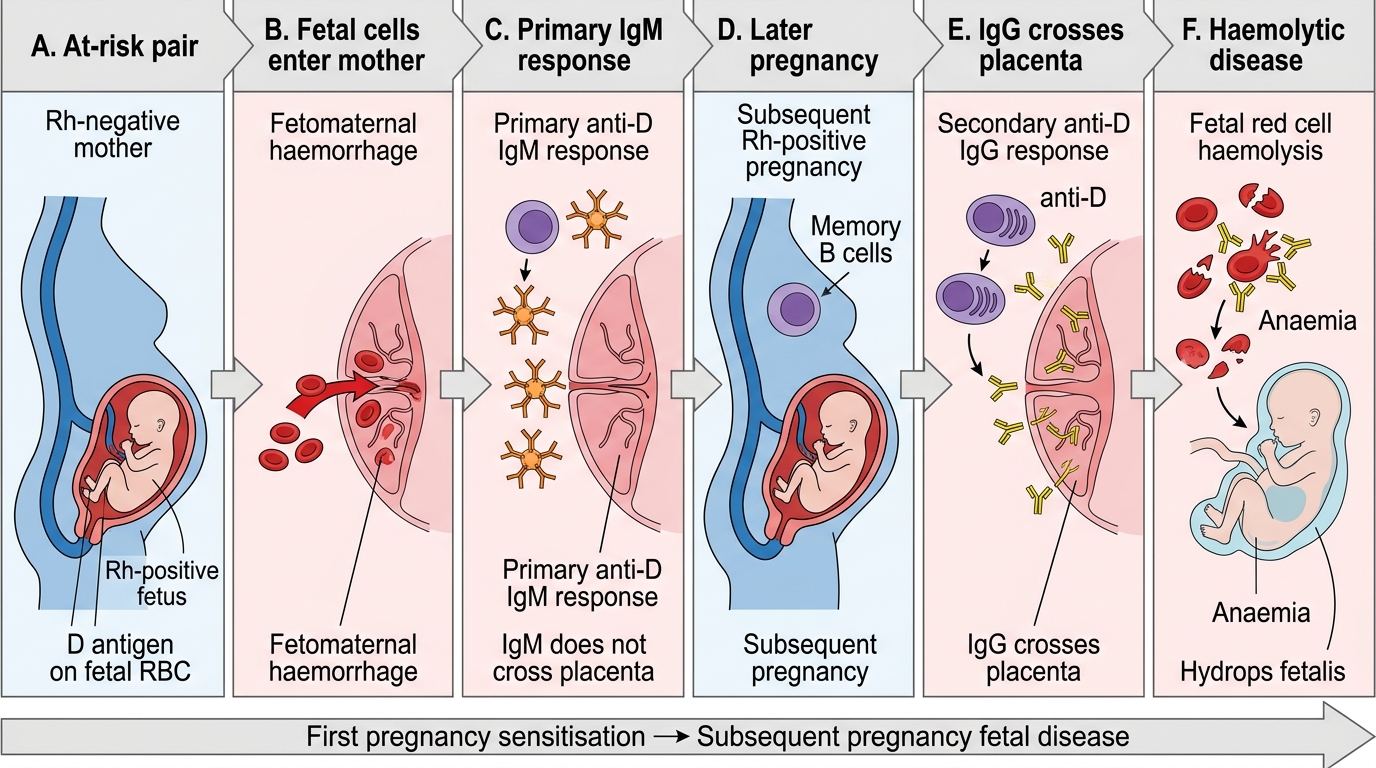
The pathophysiology of Rh iso-immunization unfolds across two pregnancies and involves a classic primary-then-secondary immune response directed against a single red cell surface antigen — the Rh D antigen — on fetal erythrocytes that have leaked into the maternal circulation.
Step 1 — Sensitisation (first sensitising event):
The Rh D antigen is expressed only on red blood cells (not platelets, lymphocytes, or nucleated precursors). During pregnancy, small quantities of fetal red cells normally enter the maternal circulation through microscopic breaks in the chorionic villi — a process called fetomaternal haemorrhage (FMH). In most pregnancies, the volume of FMH is tiny (<0.1 mL) and does not trigger sensitisation. However, larger FMH events — at delivery (20–30% of all deliveries have FMH >0.1 mL), after miscarriage, ectopic pregnancy, antepartum haemorrhage, amniocentesis, external cephalic version, or abdominal trauma — deliver enough D-positive red cells to trigger a primary immune response in the Rh-negative mother. The primary response takes 6–12 weeks to develop and is predominantly IgM (too large to cross the placenta) — so the first pregnancy is almost always unaffected.
Step 2 — Secondary immune response (subsequent D-positive pregnancy):
When D-positive fetal red cells re-enter the sensitised mother's circulation in a subsequent pregnancy, a brisk anamnestic (memory) secondary immune response rapidly produces large quantities of IgG anti-D antibodies. These IgG antibodies are small enough to be actively transported across the placenta by neonatal Fc receptors (FcRn) on trophoblasts from 16 weeks gestation onward. The transferred anti-D binds to the D antigen on fetal erythrocytes, coating them with antibody (opsonisation).
Step 3 — Fetal red cell destruction:
Antibody-coated fetal red cells are recognised and destroyed by fetal splenic macrophages (extravascular haemolysis). The rate of haemolysis depends on the quantity and avidity of the transferred anti-D antibodies. As fetal haemolysis accelerates:
- Compensatory extramedullary erythropoiesis develops in the fetal liver and spleen — causing hepatosplenomegaly
- Fetal anaemia (haemoglobin <10 g/dL in the fetus) triggers a hyperdynamic circulation and decreased erythrocyte production relative to demand
- Portal hypertension from hepatic involvement reduces albumin synthesis → hypoalbuminaemia → oncotic pressure falls → generalised fetal oedema and fluid accumulation in serous cavities (hydrops fetalis)
- In the neonate, the icteric neonatal liver cannot conjugate the massive bilirubin load from haemolysis → unconjugated hyperbilirubinaemia → kernicterus risk
Sensitising events that trigger anti-D prophylaxis (any event causing FMH):
- Miscarriage (spontaneous or induced), especially ≥12 weeks
- Ectopic pregnancy
- Antepartum haemorrhage (including threatened miscarriage with significant bleeding)
- Amniocentesis, chorionic villus sampling, cordocentesis
- External cephalic version
- Abdominal trauma during pregnancy
- Delivery (normal or caesarean)
Mechanism of Rh Iso-Immunization
Diagnosis and Investigation of Rh Iso-Immunization
The diagnostic pathway for Rh iso-immunization begins at the first antenatal visit and continues with serial monitoring throughout the pregnancy. The key investigations serve three distinct purposes: identifying the at-risk woman, detecting early sensitisation, and quantifying the degree of fetal compromise.
At Booking (First Antenatal Visit):
Every pregnant woman must have ABO blood group and Rh D typing performed. All Rh-D negative women are identified, and an Indirect Coombs Test (ICT) — also called the indirect antiglobulin test (IAT) — is performed to detect whether the woman is already sensitised from a previous event. The ICT mixes the woman's serum with standardised D-positive red cells in the presence of anti-human globulin; agglutination indicates that anti-D IgG antibodies are present in her serum and have bound to the test cells.
ICT is Positive — Managing the Sensitised Woman:
If ICT is positive, the antibody must be identified (anti-D vs other Rh antibodies vs non-Rh antibodies such as anti-Kell) and its titre (dilution end-point) established. In non-sensitised Rh-negative women, ICT will be negative throughout — they receive prophylaxis. For the sensitised woman:
- ICT titre <1:8: fetal hydrops is very unlikely; monitor with repeat titres every 4 weeks; fetal surveillance with MCA Doppler from 24 weeks
- ICT titre 1:8–1:16: borderline; begin MCA-PSV Doppler monitoring
- ICT titre ≥1:16 (critical titre): significant risk of fetal haemolytic disease; begin regular MCA-PSV Doppler monitoring every 1–2 weeks; titre alone is no longer reliable at this level because it does not correlate linearly with fetal anaemia severity
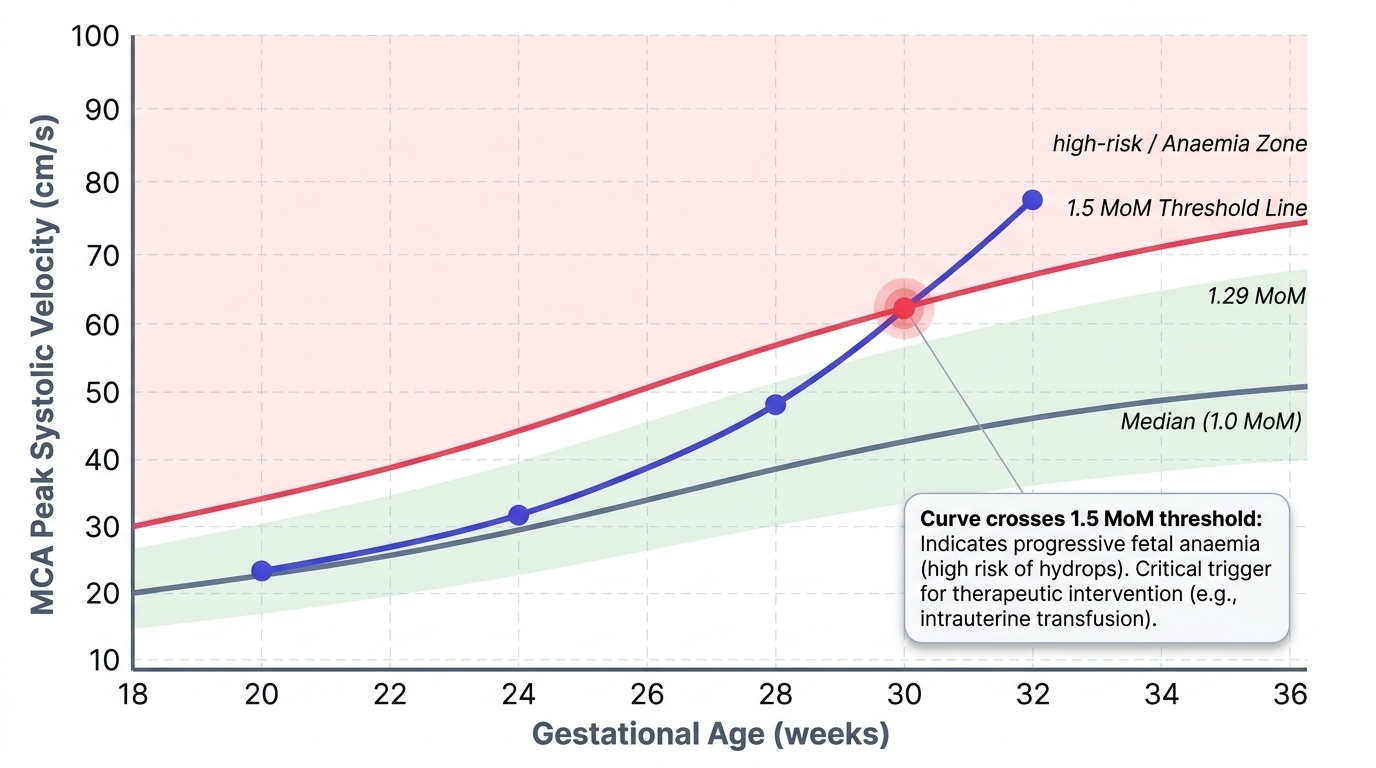
MCA-PSV Doppler — the key non-invasive fetal surveillance tool:
The middle cerebral artery peak systolic velocity (MCA-PSV) exploits the physiology of fetal anaemia: when the fetus is anaemic, cardiac output increases and blood viscosity falls → blood flows faster through the cerebral vasculature → MCA-PSV rises. MCA-PSV is measured by Doppler ultrasound at the origin of the MCA from the circle of Willis. Values are expressed as multiples of the median (MoM) for gestational age. A value >1.5 MoM for gestational age indicates moderate-to-severe fetal anaemia with a sensitivity approaching 90% for fetal haemoglobin ≤8 g/dL (the threshold for IUT). This measurement has replaced invasive amniocentesis (measurement of amniotic fluid bilirubin optical density — the Liley curve) as the primary fetal surveillance tool in sensitised pregnancies.
Kleihauer-Betke (KB) Test — quantifying fetomaternal haemorrhage:
Performed on maternal blood after a sensitising event or delivery. The KB test uses the principle of acid elution: fetal haemoglobin (HbF) resists acid (remaining red in colour); adult haemoglobin (HbA) elutes out (leaving ghost cells). The percentage of fetal cells in the maternal smear is counted under microscopy and used to calculate the total volume of fetomaternal haemorrhage:
FMH volume (mL) = (% fetal cells / 100) × maternal blood volume (5,000 mL)
A standard 300 µg dose of anti-D covers up to 30 mL of fetal blood (or 15 mL fetal red cells). If KBT reveals FMH >30 mL, additional anti-D at 10 µg per 1 mL of fetal red cells is required.
Cordocentesis (percutaneous umbilical blood sampling, PUBS):
When MCA-PSV >1.5 MoM, fetal blood is sampled directly from the umbilical vein under ultrasound guidance. This provides fetal haemoglobin, haematocrit, blood group, and reticulocyte count — and the equipment for intrauterine transfusion is on standby during the same procedure. Cordocentesis is invasive (0.5–1% procedure-related loss rate) and is reserved for cases where the MCA-PSV threshold has been crossed.
Provided image
SELF-CHECK
A Rh-negative woman at 30 weeks has ICT titre 1:32 and MCA-PSV Doppler measured at 1.7 MoM for gestational age. What is the next step in management?
A. Repeat MCA-PSV in 4 weeks to confirm the finding
B. Administer anti-D immunoglobulin 300 µg — this will reduce the antibody titre
C. Proceed to cordocentesis ± intrauterine transfusion
D. Deliver immediately by caesarean section
Reveal Answer
Answer: C. Proceed to cordocentesis ± intrauterine transfusion
MCA-PSV >1.5 MoM is the threshold for fetal anaemia requiring invasive intervention. The next step is cordocentesis (percutaneous umbilical blood sampling) to confirm fetal haemoglobin and haematocrit, with intrauterine transfusion (IUT) performed in the same sitting if fetal Hb <10 g/dL (or haematocrit <30%). Anti-D prophylaxis is ineffective once sensitisation has occurred — it only prevents sensitisation in non-immunised women. Delivery at 30 weeks without fetal lung maturity is not appropriate when IUT is available. Waiting 4 weeks with MCA-PSV 1.7 MoM risks progressive anaemia and hydrops.