Page 25 of 38
OG12.9 | Thyroid Disorders in Pregnancy — SDL Guide
Learning Objectives
- Explain the physiological changes in thyroid function during pregnancy and the basis of trimester-specific TSH reference ranges
- Distinguish between Graves' disease and gestational transient thyrotoxicosis on clinical and biochemical grounds
- Describe the impact of hypothyroidism and hyperthyroidism on maternal and fetal outcomes
- Outline the management of hypothyroidism in pregnancy including levothyroxine dose adjustment (~30%) and TSH monitoring
- Explain the choice of PTU (first trimester) vs carbimazole/methimazole (second-third trimester) for hyperthyroidism and the neonatal surveillance implications
INSTRUCTIONS
Thyroid disorders are the second most common endocrine complication of pregnancy after gestational diabetes. The thyroid is profoundly affected by pregnancy — increased thyroxine-binding globulin, elevated hCG cross-stimulating TSH receptors, and rising fetal iodine demands all alter the biochemical picture. Failure to use trimester-specific TSH reference ranges leads to both over- and under-diagnosis. Untreated hypothyroidism impairs fetal neurodevelopment; untreated hyperthyroidism risks thyroid storm, preterm birth, and fetal thyrotoxicosis. This module gives you the pathophysiological framework, the diagnostic decision-tree, and the prescribing rules to manage both conditions safely.
References
- DC Dutta's Textbook of Obstetrics, 9th ed., Ch 18 — Medical Disorders in Pregnancy (textbook)
- ATA (American Thyroid Association) — Management of Thyroid Dysfunction during Pregnancy and Postpartum: Guidelines 2017 (guideline)
- Williams Obstetrics, 26th ed., Ch 58 — Thyroid and Other Endocrine Disorders (textbook)
- FOGSI Good Clinical Practice Recommendations — Thyroid Disorders in Pregnancy 2021 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Shalini is a 29-year-old primigravida at 8 weeks gestation, referred to you for 'abnormal thyroid tests'. She complains of extreme fatigue — 'I can barely get out of bed' — and has gained 4 kg in the first trimester. Her TSH is reported as 5.8 mIU/L. Her friend, also 8 weeks pregnant, has just been diagnosed with 'hyperthyroidism' because her TSH is 0.05 mIU/L and she has severe nausea and vomiting. You know from your training that the normal non-pregnant TSH range is 0.4–4.0 mIU/L. But you also know that pregnancy changes the rules. Which woman truly has a thyroid disorder — and for which one might the laboratory result be entirely explained by the normal physiology of early pregnancy? The answer requires you to apply trimester-specific reference ranges and understand exactly why hCG behaves as a weak TSH mimic.
WHY THIS MATTERS
Thyroid disorders complicate approximately 2–3% of pregnancies in India. Hypothyroidism (predominantly subclinical) is the more common condition; if untreated, it is associated with preeclampsia, placental abruption, preterm birth, and — most critically — impaired fetal neurodevelopment (the fetal brain depends entirely on maternal thyroid hormone for the first 12 weeks before the fetal thyroid becomes functional). Hyperthyroidism, if poorly controlled, risks thyroid storm (a medical emergency with up to 25% maternal mortality), preterm birth, intrauterine growth restriction, and — when managed with antithyroid drugs — neonatal thyroid dysfunction from transplacental drug transfer. The choice between PTU and carbimazole is not arbitrary: carbimazole carries a specific teratogenic risk in the first trimester, while PTU carries hepatotoxicity risk if used long-term. Getting the drug choice and the monitoring right requires knowledge of the mechanisms, not just the prescription.
RECALL
Recall from Physiology that the thyroid gland synthesises thyroxine (T4) and triiodothyronine (T3) through a process of iodide trapping, organification (TPO + hydrogen peroxide oxidises iodide → binds to thyroglobulin), and proteolytic release. T4 is the principal secretory product but has lower receptor affinity than T3; peripheral deiodinases convert T4 → T3 in target tissues. The hypothalamic–pituitary–thyroid (HPT) axis: TRH (hypothalamus) → TSH (pituitary) → stimulates T3/T4 production → negative feedback inhibits TRH/TSH. TSH has the highest sensitivity for detecting early thyroid dysfunction. Recall also from Biochemistry that in non-pregnant adults, thyroid hormones circulate mostly protein-bound (99%) — thyroxine-binding globulin (TBG) is the main carrier. Only the free fractions (FT3, FT4) are biologically active — total T3/T4 levels are unreliable in pregnancy because TBG increases.
The Pregnant Woman with Thyroid Symptoms — Recognising the Problem
The clinical diagnosis of thyroid disorders in pregnancy requires extra care because many symptoms of thyroid dysfunction — fatigue, heat intolerance, palpitations, weight changes, mood disturbance — overlap substantially with normal pregnancy symptoms. A systematic clinical approach, anchored by biochemical testing, is essential.
HYPOTHYROIDISM — clinical features:
The symptoms of hypothyroidism in pregnancy mirror those outside pregnancy but are often dismissed as 'normal pregnancy tiredness': profound fatigue and lethargy, cold intolerance, constipation, dry skin, hair thinning, periorbital oedema, and weight gain in excess of expected pregnancy gain. Goitre may be present if the underlying cause is Hashimoto's thyroiditis or iodine deficiency. In severe hypothyroidism, myxoedema (non-pitting oedema, slowed reflexes) may develop. The most feared consequence is subclinical hypothyroidism going undetected — no symptoms at all, but with the fetal brain silently deprived of adequate thyroid hormone at a critical developmental window.
Causes of hypothyroidism in pregnancy:
- Hashimoto's thyroiditis (autoimmune): the most common cause; anti-thyroid peroxidase (anti-TPO) antibodies progressively destroy thyroid tissue; tends to improve in mid-pregnancy (immune tolerance) then relapse postpartum
- Iodine deficiency: globally common; in India, universal iodisation of salt has reduced prevalence but it remains a consideration in areas with inadequate coverage; the fetus is at high risk for endemic cretinism (irreversible intellectual disability, deafness, growth failure)
- Post-treatment: prior thyroidectomy or radioactive iodine (RAI) ablation for hyperthyroidism; these women are always hypothyroid and require higher levothyroxine doses in pregnancy
HYPERTHYROIDISM — clinical features:
Hyperthyroid symptoms during pregnancy include palpitations, tremor, anxiety, heat intolerance, excessive sweating, and weight loss or failure to gain expected pregnancy weight despite good appetite. Tachycardia (resting HR >100), goitre, and eye signs (exophthalmos, lid lag, proptosis) specifically suggest Graves' disease rather than gestational thyrotoxicosis. Graves' disease is the most common cause of hyperthyroidism in pregnancy (~85% of cases) and is caused by TRAb (TSH-receptor-stimulating antibodies).
Gestational Transient Thyrotoxicosis (GTT):
GTT must be distinguished from Graves' because it requires no antithyroid drugs. It occurs in 1–3% of pregnancies, peaks at 10–12 weeks (coinciding with peak hCG), and resolves spontaneously by 18–20 weeks. Clinical clues: no goitre, no eye signs, associated with hyperemesis gravidarum, and the severity parallels hCG levels (higher hCG → more suppressed TSH). TRAb is ABSENT in GTT (present in Graves').
Thyroid storm is a rare but life-threatening complication of uncontrolled hyperthyroidism triggered by delivery, infection, surgery, or stress; it presents with extreme tachycardia, high fever (>38.5°C), agitation, vomiting, diarrhoea, and heart failure — with a maternal mortality of up to 25% without prompt ICU-level management.
SELF-CHECK
A woman at 10 weeks gestation has severe nausea/vomiting, TSH 0.04 mIU/L (T1 reference 0.1–2.5), FT4 mildly elevated, no goitre, no eye signs, TRAb NEGATIVE. What is the most likely diagnosis?
A. Graves' disease requiring urgent antithyroid therapy
B. Gestational transient thyrotoxicosis — manage supportively, no ATD needed
C. Subclinical hypothyroidism — start levothyroxine
D. Normal pregnancy — TSH of 0.04 is within trimester-specific range
Reveal Answer
Answer: B. Gestational transient thyrotoxicosis — manage supportively, no ATD needed
Gestational transient thyrotoxicosis (GTT) is caused by hCG cross-reacting with TSH receptors — it peaks at 10–12 weeks, is associated with hyperemesis, has mildly suppressed TSH and slightly elevated FT4, NO goitre, NO eye signs, and NEGATIVE TRAb (the hallmark that distinguishes it from Graves'). GTT is self-limiting and resolves by 18–20 weeks; antithyroid drugs are NOT indicated. TSH 0.04 is below the T1 reference range (0.1) — this is NOT normal — but the clinical context and negative TRAb confirm GTT rather than Graves'.
Why Pregnancy Changes Thyroid Physiology — Pathophysiology
Pregnancy imposes profound and predictable changes on thyroid physiology that shift the biochemical parameters used to diagnose thyroid disorders. Applying non-pregnant reference ranges to pregnant women is one of the most common errors in antenatal thyroid management.
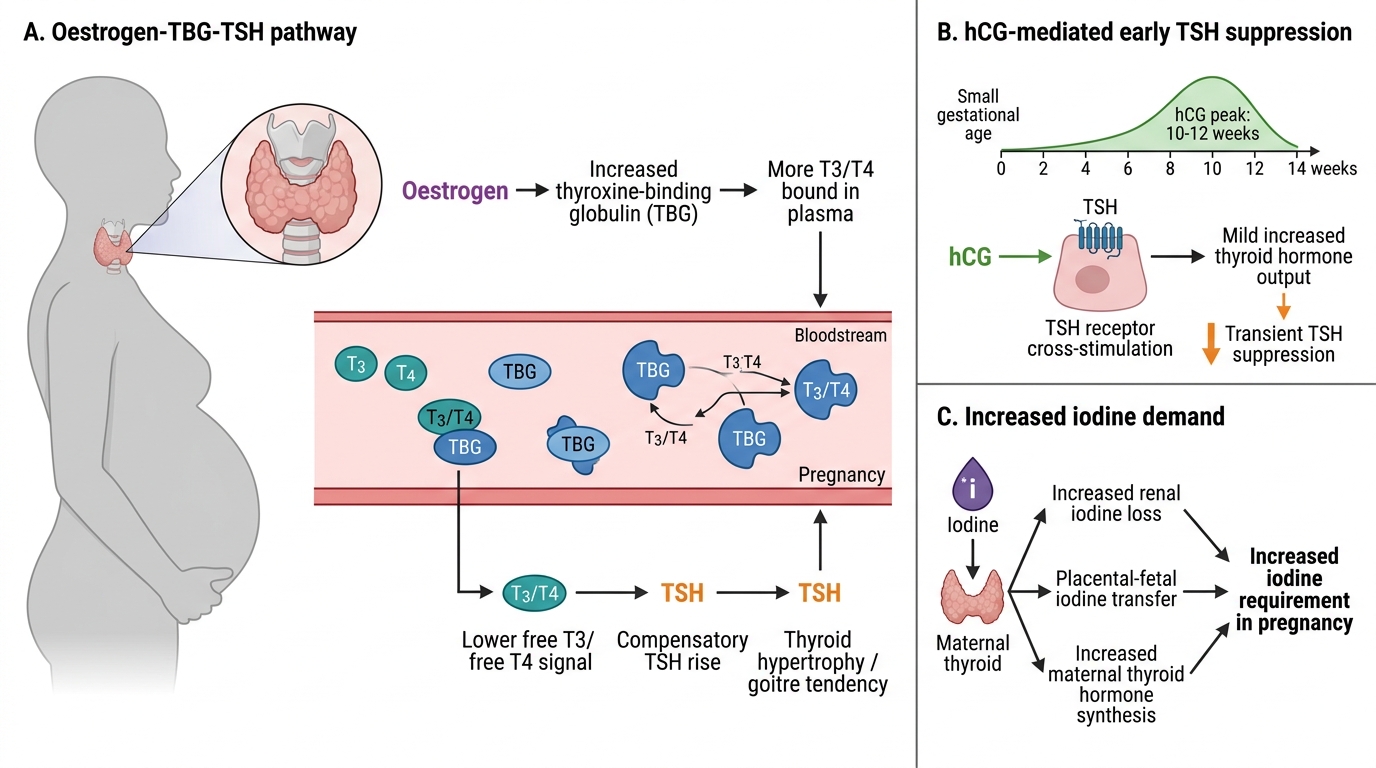
Mechanism 1 — Increased Thyroxine-Binding Globulin (TBG):
Oestrogen stimulates hepatic synthesis of TBG and reduces its clearance by increasing sialylation (a posttranslational modification that prolongs TBG half-life). TBG levels roughly double by the end of the first trimester. This increased TBG avidly binds circulating T4 and T3, reducing the free fractions. The pituitary senses reduced FT4 → increases TSH → stimulates the thyroid to produce more T3/T4 → total T4 rises by ~40% to compensate, restoring FT4 to normal. Practical implications: total T4 levels are unreliable in pregnancy because they reflect TBG-bound hormone; only FT4 and FT3 (free fractions) are interpretable. However, FT4 assays are also variably affected by the changed TBG milieu and immunoassay technique — interpretation requires trimester-specific reference values.
Mechanism 2 — hCG Cross-Reactivity with TSH Receptors:
Human chorionic gonadotrophin (hCG) has a heterodimeric structure — its alpha subunit is identical to that of TSH, LH, and FSH. At the high concentrations of hCG present in the first trimester (peak 50,000–100,000 IU/L at 10–12 weeks), hCG exerts weak agonist activity at the TSH receptor on thyroid follicular cells, directly stimulating T4/T3 production. This suppresses pituitary TSH via negative feedback. The result: TSH is physiologically lower in the first trimester than at any other time. The magnitude of suppression mirrors the hCG concentration — twin pregnancies (higher hCG) have even lower TSH; molar pregnancies (extreme hCG) can mimic florid hyperthyroidism.
Mechanism 3 — Increased Renal Iodine Clearance and Fetal Demand:
Glomerular filtration rate increases by 50% in pregnancy, increasing renal iodine excretion. Simultaneously, the fetus and placenta extract iodine from maternal circulation from approximately 10–12 weeks. The net effect is a relative iodine deficiency in the mother — if dietary iodine is inadequate (as in areas without iodised salt), the thyroid enlarges (goitre), attempts to concentrate more iodine, and may fail to maintain euthyroid status, leading to hypothyroidism.
Fetal thyroid development:
The fetal thyroid begins concentrating iodine at approximately 10–12 weeks gestation. Before this point, the fetal brain is entirely dependent on maternal T4 for its neurodevelopment. Maternal T4 crosses the placenta via specific transporters and is converted to T3 in fetal brain tissue. This explains why maternal hypothyroidism in the first trimester is particularly damaging to fetal neurodevelopment — the fetal thyroid cannot yet compensate, and the fetal brain cannot protect itself.
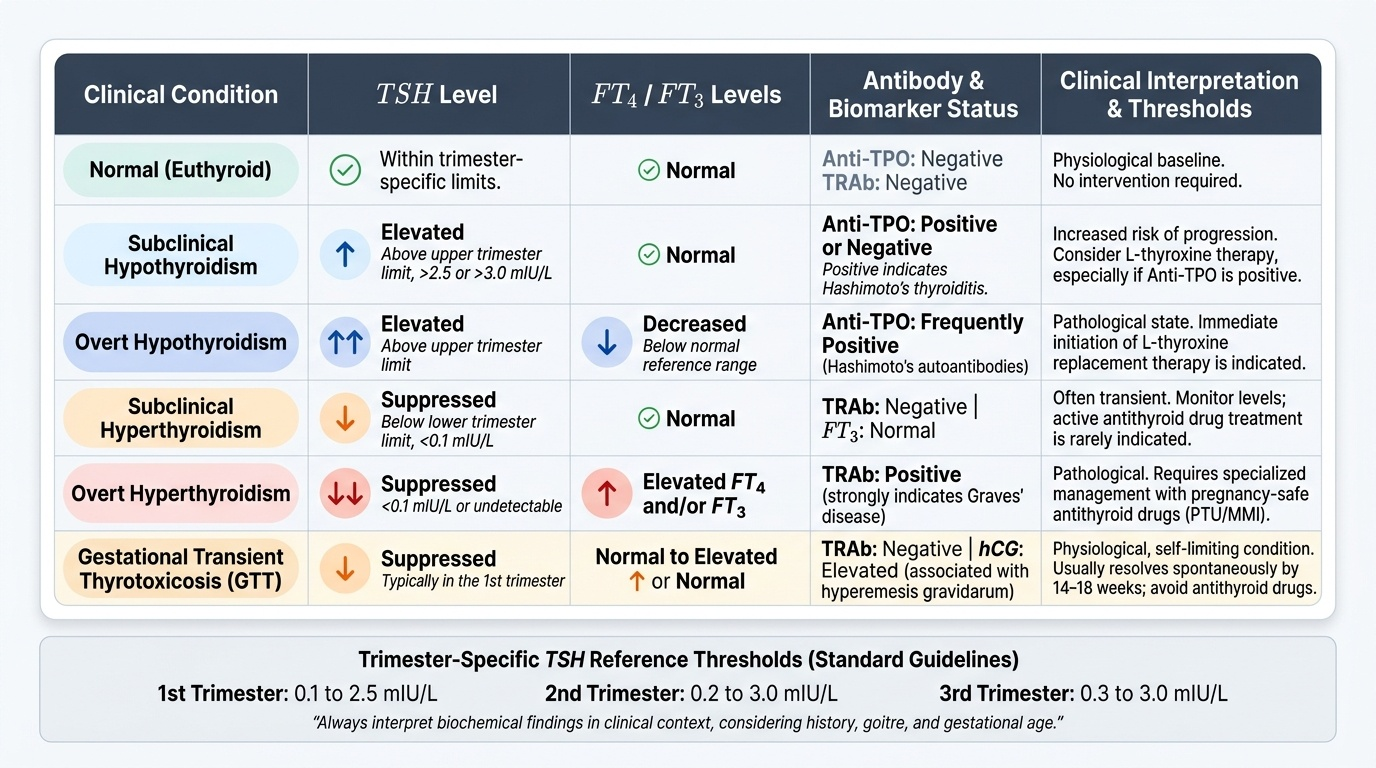
Trimester-specific TSH reference ranges (ATA 2017, approximate):
- First trimester: 0.1–2.5 mIU/L
- Second trimester: 0.2–3.0 mIU/L
- Third trimester: 0.3–3.0 mIU/L
These are lower than the non-pregnant normal (0.4–4.0 mIU/L) — the upper limit decreases in T1 (hCG-mediated TSH suppression) and the lower limit of normal is also lower in T1. Without trimester-specific ranges, T1 women with normal physiology are misdiagnosed as hyperthyroid, and women with early hypothyroidism (TSH 2.6–4.0) are missed.
Pregnancy-Induced Changes in Thyroid Physiology
Diagnosis and Investigations for Thyroid Disorders in Pregnancy
Biochemical screening forms the backbone of thyroid disorder diagnosis in pregnancy. The investigation strategy must use trimester-specific reference ranges and interpret results in their clinical context — particularly distinguishing the physiological TSH suppression of early pregnancy (driven by hCG and TBG changes) from true pathological hyper- or hypothyroidism. A structured approach — TSH first, then FT4 and specific antibodies — ensures that no case of clinically significant thyroid dysfunction is missed while avoiding unnecessary treatment of physiological variation. The history, examination findings (goitre, eye signs, cardiac rate, skin changes), and gestational age at which the result was obtained all inform interpretation.
TSH as the primary screening test:
Serum TSH is the most sensitive and specific single test for thyroid dysfunction; it is the recommended first-line investigation for any suspected thyroid disorder in pregnancy. A TSH outside the trimester-specific reference range is the trigger for further testing:
- TSH elevated (above upper trimester-specific limit) → proceed to FT4 to classify as subclinical (TSH↑, FT4 normal) vs overt (TSH↑, FT4↓) hypothyroidism; add anti-TPO antibody to identify Hashimoto's
- TSH suppressed (below lower trimester-specific limit) → proceed to FT4 and FT3 to classify as subclinical (TSH↓, FT4 normal) vs overt (TSH↓, FT4↑) hyperthyroidism; add TRAb to distinguish Graves' from GTT
Universal TSH screening at booking is not mandated in all Indian guidelines, but targeted case-finding (screen if: history of thyroid disease, goitre, family history, previous pregnancy loss, infertility, autoimmune disease, symptoms) is recommended. Some centres advocate universal screening given the high burden of hypothyroidism in India.
Anti-TPO antibody (anti-thyroid peroxidase):
Present in 80–90% of Hashimoto's thyroiditis; also elevated in many Graves' patients. A positive anti-TPO with elevated TSH confirms autoimmune hypothyroidism. Importantly, anti-TPO positivity with NORMAL TSH (euthyroid anti-TPO positive) is also significant: these women have a higher risk of pregnancy loss, preterm birth, and postpartum thyroiditis — some guidelines recommend levothyroxine if TSH >2.5 and anti-TPO positive.
TRAb (TSH-receptor antibody):
The defining antibody of Graves' disease. Positive TRAb confirms Graves' and excludes GTT. High maternal TRAb (>3× upper limit of normal at 36 weeks) indicates risk of neonatal Graves' disease (TRAb crosses the placenta and stimulates the neonatal thyroid gland for the first 3–12 weeks of life). Measuring TRAb at 36 weeks guides neonatal surveillance planning.
FT4 and FT3: used in conjunction with TSH for classification. FT4 is the primary free-hormone measurement; FT3 is elevated in T3-predominant hyperthyroidism and thyroid storm.
Thyroid ultrasound: used to identify goitre, nodules, and thyroid vascular flow (Doppler — increased vascularity in Graves'). Not used to diagnose function.
Fetal surveillance in hyperthyroid pregnancies:
Fetal tachycardia (>160 bpm on CTG), fetal goitre (on USS), intrauterine growth restriction, and advanced bone maturation are signs of fetal thyrotoxicosis from transplacental TRAb. If fetal goitre is detected, cordocentesis to measure fetal TSH/FT4 may be needed in specialist centres.
Provided image
SELF-CHECK
A woman at 16 weeks gestation (second trimester) has TSH 3.6 mIU/L, FT4 normal, anti-TPO POSITIVE. Using the ATA trimester-specific upper limit for T2 (3.0 mIU/L), how should she be managed?
A. No treatment needed — TSH 3.6 is within non-pregnant normal range (0.4–4.0)
B. Start levothyroxine — TSH 3.6 exceeds the second-trimester upper limit of 3.0 mIU/L
C. Refer for thyroid surgery — anti-TPO positivity indicates a surgical condition
D. Start antithyroid drugs — anti-TPO positivity means Graves' disease
Reveal Answer
Answer: B. Start levothyroxine — TSH 3.6 exceeds the second-trimester upper limit of 3.0 mIU/L
The second-trimester TSH upper limit is approximately 3.0 mIU/L (ATA 2017) — TSH of 3.6 exceeds this. With positive anti-TPO (confirming autoimmune hypothyroidism/Hashimoto's), this is subclinical hypothyroidism in pregnancy and warrants levothyroxine treatment. Using the non-pregnant upper limit of 4.0 would miss this diagnosis. Anti-TPO is a marker of autoimmune hypothyroidism — not Graves' disease (which requires TRAb), and not a surgical indication.