Page 14 of 38
OG12.5 | Urinary Tract Infection in Pregnancy — SDL Guide (Part 2)
Impact of UTI on Pregnancy and Adverse Effects
The significance of UTI in pregnancy — particularly when untreated or inadequately treated — extends well beyond the urinary tract, creating a cascade of maternal and foetal complications that illustrate why this apparently localised infection is classified as a major obstetric risk. The pathophysiological connections between bacteriuria and preterm birth, between pyelonephritis and acute kidney injury, and between endotoxaemia and ARDS are not theoretical associations — they represent well-documented clinical consequences documented in prospective cohort studies and Cochrane systematic reviews. The most striking finding from these studies is the dose-response relationship between the severity of infection and the severity of outcomes: women with treated ASB have perinatal outcomes approaching those of uninfected women; women with untreated ASB have significantly elevated rates of pyelonephritis, preterm birth, and LBW; and women with complicated pyelonephritis (sepsis, AKI, ARDS) face maternal and perinatal mortality risks that rival those of major obstetric emergencies. This gradient demonstrates unambiguously that the clinical effort invested in screening and treating even asymptomatic bacteriuria is effort well spent. — particularly when untreated or inadequately treated — extends well beyond the urinary tract, affecting both maternal systemic health and foetal wellbeing through distinct but interconnected pathophysiological pathways. Appreciation of these consequences is what drives the clinical urgency behind the seemingly straightforward recommendation to screen and treat all pregnant women for asymptomatic bacteriuria.
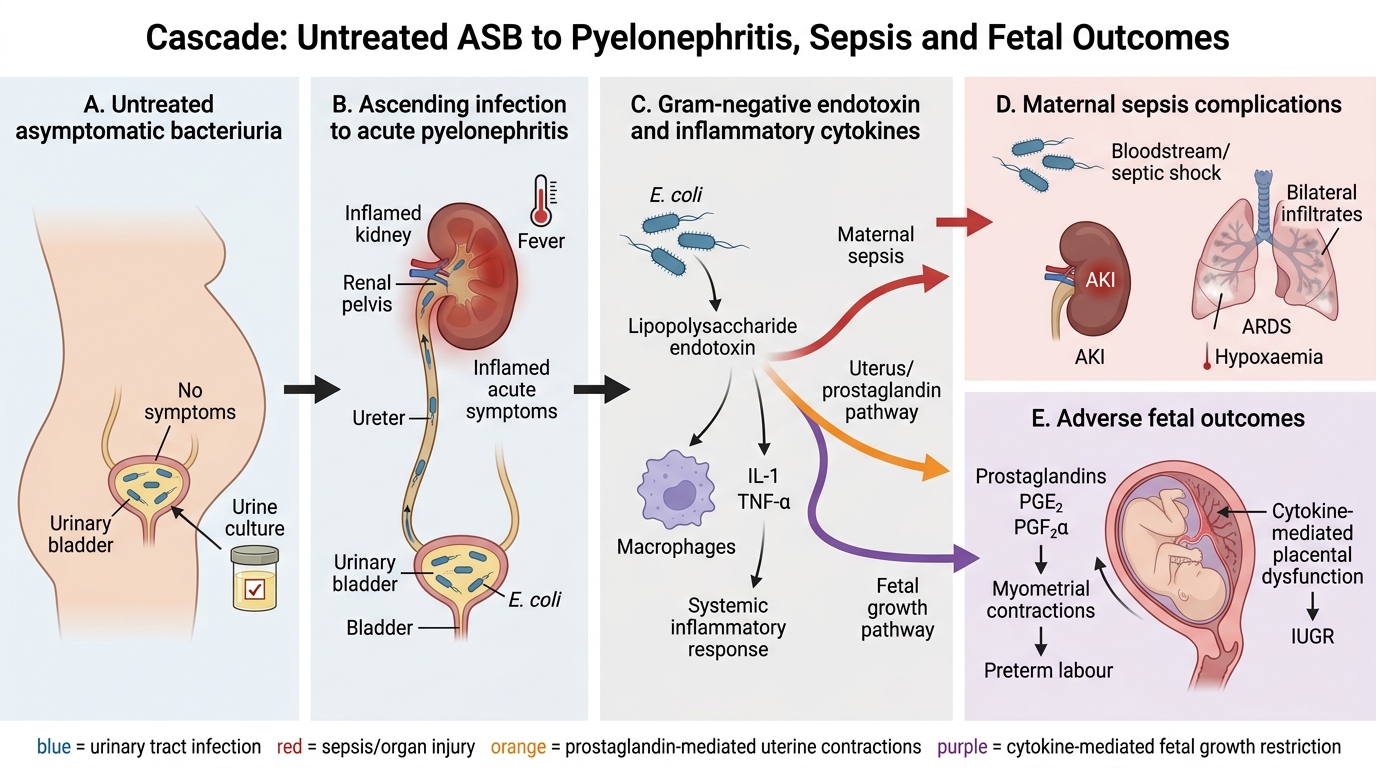
Cascade from Asymptomatic Bacteriuria to Maternal and Fetal Complications
Maternal adverse effects:
Acute pyelonephritis and its complications:
- Gram-negative sepsis (urosepsis): E. coli bacteraemia occurs in approximately 20% of pyelonephritis cases; lipopolysaccharide (endotoxin) from Gram-negative bacteria triggers systemic inflammatory response syndrome (SIRS), with risk of septic shock
- Acute kidney injury (AKI): endotoxin-mediated renal vasoconstriction and tubular toxicity; occurs in up to 20% of acute pyelonephritis in pregnancy; usually reversible with treatment but can require dialysis in severe cases
- Acute respiratory distress syndrome (ARDS): pulmonary capillary endothelial injury mediated by endotoxin and inflammatory cytokines; complicates 2–8% of pyelonephritis in pregnancy; characterised by bilateral pulmonary infiltrates, hypoxaemia, and respiratory failure; carries significant maternal mortality if not recognised early
- Preterm labour: endotoxin and inflammatory cytokines (especially interleukin-1, TNF-alpha) directly stimulate uterine prostaglandin production (prostaglandins PGE₂ and PGF₂α trigger myometrial contractions), precipitating preterm labour — this is the most common adverse outcome
- Recurrent UTI: once colonised, the bacteriuric woman is at high risk of reinfection; surveillance cultures and suppressive therapy may be required
- Maternal anaemia: haemolysis mediated by bacterial toxins can worsen pregnancy anaemia
Foetal and neonatal adverse effects:
- Preterm birth: the leading foetal complication of pyelonephritis and untreated bacteriuria; prostaglandin-driven contractions and cervical change can result in delivery before 37 weeks
- Low birth weight (LBW): both preterm delivery and IUGR contribute
- IUGR: impaired uteroplacental perfusion during maternal sepsis and the catabolic/inflammatory state of pyelonephritis reduce foetal oxygen and nutrient supply
- Perinatal mortality: severe, complicated pyelonephritis with septic shock carries risk of foetal death from maternal haemodynamic instability
- Neonatal UTI and sepsis: rare but described in neonates born to mothers with bacteraemia from UTI
The risk gradient is important: women with treated ASB have perinatal outcomes approaching those of women without bacteriuria; the adverse outcomes are concentrated in the untreated or incompletely treated group. This is the evidence base for universal screening and mandatory treatment of ASB in pregnancy.
Management During Pregnancy and Labour
The management of UTI in pregnancy is guided by two fundamental principles: firstly, that any degree of bacteriuria — including the completely asymptomatic variety — carries sufficient risk of serious harm to the mother and foetus that treatment is mandatory; and secondly, that antibiotic selection in pregnancy must be guided by culture sensitivities AND by each antibiotic's safety profile across the trimesters of pregnancy, because several agents that are routinely used for UTI outside pregnancy are either contraindicated or require specific gestational restrictions. The cost of prescribing the wrong antibiotic in pregnancy — whether fluoroquinolones causing cartilage damage, tetracyclines causing tooth and bone dysplasia, trimethoprim causing antifolate teratogenicity in the first trimester, or nitrofurantoin causing neonatal haemolysis at term — is borne by the foetus, not the prescriber. These restrictions are not academic: they appear in every major examination on obstetric medicine and are applied daily in antenatal clinics. Master them, and you will both prescribe safely and pass examinations.: firstly, that any degree of bacteriuria (including asymptomatic) carries a risk of serious maternal and foetal harm, and must therefore be treated; and secondly, that antibiotic selection in pregnancy must balance efficacy against the potential for foetal harm — several antibiotics that are routinely used for UTI outside pregnancy are contraindicated at specific trimesters or throughout pregnancy. The following management framework covers all three clinical presentations, from ASB to pyelonephritis.
A. Antibiotic Safety Considerations in Pregnancy
Not all antibiotics safe for non-pregnant adults are safe in pregnancy:
⚑ AI image — pending faculty review (auto-QA score 4/10; best of 3 attempts)
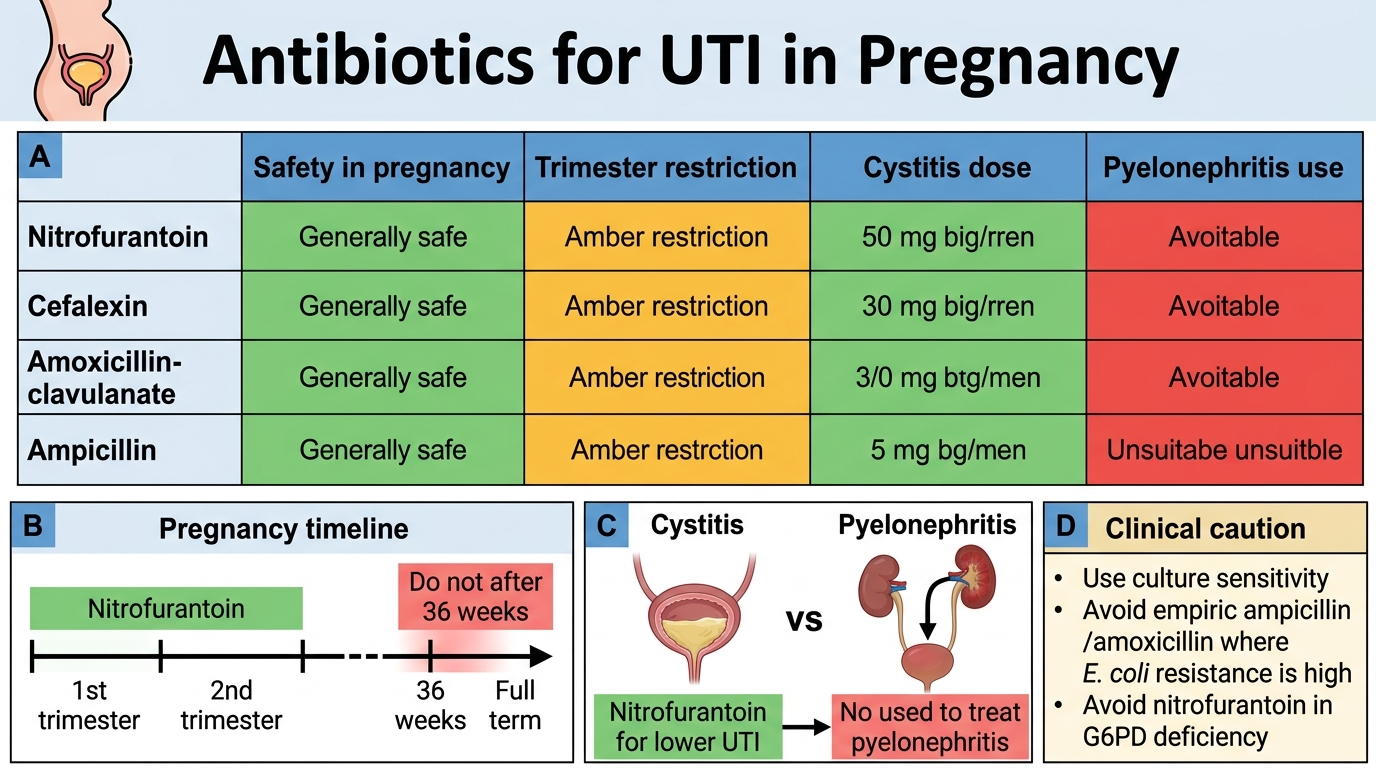
Antibiotics for UTI in Pregnancy
| Antibiotic | Safety in pregnancy | Key restriction |
|---|---|---|
| Cefalexin (cephalosporin) | Safe throughout | First choice if sensitivities allow |
| Nitrofurantoin | Safe 1st and 2nd trimester | Avoid at term (after 36 weeks): risk of neonatal haemolytic anaemia (immature erythrocyte glutathione instability); also avoid if G6PD deficiency |
| Amoxicillin | Safe throughout (if organism sensitive) | High rates of E. coli resistance in India — always check sensitivity |
| Amoxicillin-clavulanate | Safe throughout | Broader spectrum; useful for resistant organisms |
| Trimethoprim | AVOID in first trimester: antifolate — inhibits dihydrofolate reductase → risk of neural tube defects; can be used in 2nd/3rd trimester with caution | |
| Fluoroquinolones (ciprofloxacin, norfloxacin) | AVOID in pregnancy: arthropathy risk to foetal cartilage (animal data); avoid throughout | |
| Tetracyclines | CONTRAINDICATED: foetal bone/tooth discolouration, hepatotoxicity | |
| Aminoglycosides | Used IV for pyelonephritis under close monitoring | Ototoxicity/nephrotoxicity risk; use only when benefit outweighs risk for serious infection |
B. Treatment of Asymptomatic Bacteriuria (ASB)
- Antibiotic choice based on culture sensitivity: cefalexin (first line in most Indian centres), nitrofurantoin (avoid at term), or amoxicillin
- Duration: 7-day course (shorter 3–5 day courses in clinical guidelines; practice varies; 7-day courses have better cure rates in pregnancy)
- Test-of-cure culture at 1–2 weeks post-treatment to confirm eradication
- If recurrent bacteriuria (>2 episodes in pregnancy): consider suppressive therapy with nitrofurantoin 50–100 mg nocte until delivery (avoiding term) to prevent recurrence
C. Treatment of Acute Cystitis
- Same antibiotic approach as ASB (guided by sensitivities)
- 7-day course standard in pregnancy
- Encourage adequate hydration; paracetamol for discomfort
- Follow-up urine culture at 2 weeks post-treatment
D. Treatment of Acute Pyelonephritis — INPATIENT MANAGEMENT
Acute pyelonephritis in pregnancy requires hospital admission in nearly all cases:
- IV antibiotics (empirical, pending cultures and sensitivities):
- Ceftriaxone 1–2 g IV once daily (first-line empirical therapy in most guidelines)
- OR ampicillin + gentamicin (classic regime; gentamicin carries ototoxicity risk — monitor levels and limit duration)
- Switch to oral antibiotic once afebrile for 24–48 hours and tolerating oral intake
- Supportive care: IV fluids for hydration and to maintain urine output; paracetamol for fever control; analgesia for loin pain; anti-emetics for nausea
- Foetal monitoring: CTG; serial growth assessments if episode occurs in third trimester; watch for preterm contractions — consider tocolysis if contractions develop (with attention to drug interactions with antibiotics)
- Blood cultures: drawn before first antibiotic dose; repeat if clinically deteriorating
- Monitor for complications: AKI (serum creatinine, urine output), ARDS (SpO₂, respiratory rate), septic shock (HR, BP, lactate)
- Duration: IV antibiotics until afebrile for 24–48 h, then oral completion to 14 days total
E. Suppressive Therapy After Pyelonephritis
After a first episode of pyelonephritis in pregnancy:
- High risk of recurrence: suppressive antibiotics (nitrofurantoin 50–100 mg nocte, avoiding term; or cefalexin 500 mg nocte) for the remainder of the pregnancy
- Monthly MSU cultures for surveillance
- Postpartum urological review to exclude structural anomaly (VUR, calculi) that predisposed to infection
F. Intrapartum Management
- Women with ongoing or recent UTI should have a urine culture result available at the time of labour
- Adequate hydration and good bladder emptying during labour (minimise catheterisation if possible to reduce nosocomial infection risk)
- Prophylactic antibiotics for any instrumental delivery or caesarean section cover urinary pathogens
- Neonatal team alert if maternal pyelonephritis is active within 48 hours of delivery
CLINICAL PEARL
The two most important clinical rules to carry from this module are: (1) Asymptomatic bacteriuria MUST be treated in pregnancy — the absence of symptoms does not make it safe to observe; the 20–40% risk of pyelonephritis in untreated ASB is the evidence that makes treatment mandatory. Screen at booking. (2) Nitrofurantoin must NOT be given at term (after 36 weeks) — it can cause neonatal haemolytic anaemia due to immature erythrocyte glutathione. This is the antibiotic trap in UTI-in-pregnancy questions: nitrofurantoin is safe and widely used in the first and second trimesters but is contraindicated in the third trimester near delivery. Switch to cefalexin in the final weeks.
SELF-CHECK
A 37-week primigravida has an MSU culture showing Klebsiella pneumoniae sensitive to nitrofurantoin and cefalexin. Which antibiotic is the correct choice?
A. Nitrofurantoin, as it is the first-line antibiotic for UTI in pregnancy
B. Cefalexin, because nitrofurantoin is contraindicated after 36 weeks (risk of neonatal haemolytic anaemia)
C. Ciprofloxacin, as it is highly effective against Klebsiella
D. Trimethoprim-sulphamethoxazole (co-trimoxazole) as it is the standard UTI treatment
Reveal Answer
Answer: B. Cefalexin, because nitrofurantoin is contraindicated after 36 weeks (risk of neonatal haemolytic anaemia)
Nitrofurantoin is contraindicated in the third trimester (specifically after 36 weeks) because it can cause haemolytic anaemia in the neonate — the immature erythrocytes lack the glutathione stability required to handle the oxidative stress from nitrofurantoin metabolites. At 37 weeks, cefalexin (or another sensitive antibiotic) should be used. Fluoroquinolones (ciprofloxacin) are contraindicated throughout pregnancy. Trimethoprim is an antifolate contraindicated in the first trimester and used with caution only in the second and third trimesters.
Self-Assessment
Having completed this module, you should now be able to distinguish the three clinical presentations of UTI in pregnancy, explain the pathophysiological mechanisms that make pregnancy uniquely susceptible to ascending urinary infection, select appropriate antibiotics for each trimester including the critical restrictions at term and in the first trimester, and recognise the warning features of pyelonephritis that require inpatient management. These competencies are tested both in written examinations (classification questions, management vignettes) and in clinical skills assessments (counselling patients on MSU collection, explaining why treatment is needed when the patient feels well). The most frequent examination error is prescribing nitrofurantoin at term or fluoroquinolones in pregnancy — errors that, in a clinical setting, could harm a neonate or a developing foetal skeleton. Internalising the antibiotic safety profiles — not just memorising a list — will enable you to reason through novel vignettes correctly even when the specific antibiotic mentioned is not one you have previously encountered. asymptomatic bacteriuria from acute cystitis and acute pyelonephritis, understand the pathophysiological reasons why pregnancy dramatically increases the risk of upper UTI from untreated lower bacteriuria, and select appropriate antibiotics for each trimester — including the critical restriction on nitrofurantoin at term and the absolute contraindications (fluoroquinolones, tetracyclines, first-trimester trimethoprim). The key facts that appear most frequently in clinical examinations and practice scenarios are: the diagnostic threshold for ASB (≥100,000 CFU/mL), the mandatory treatment of ASB in pregnancy, the risk of pyelonephritis from untreated ASB (20–40%), and the antibiotic safety profiles across trimesters.
Key clinical rules for UTI in pregnancy:
• Diagnostic threshold for significant bacteriuria: ≥100,000 CFU/mL on MSU culture
• ASB: treat in pregnancy — 20–40% progress to pyelonephritis if untreated
• First-line antibiotics: cefalexin (safe throughout); nitrofurantoin (avoid at term ≥36 weeks)
• Avoid throughout pregnancy: fluoroquinolones (cartilage), tetracyclines (bone/tooth), high-dose trimethoprim (1st trimester — antifolate)
• Pyelonephritis: inpatient management with IV ceftriaxone or ampicillin + gentamicin; switch to oral when afebrile 24–48 h
• Suppressive therapy after recurrent bacteriuria or pyelonephritis: nitrofurantoin nocte (avoiding term)