Page 12 of 22
OG15.1 | Common Operative Obstetric Procedures — SDL Guide (Part 3)
Supervised Practice and Clinical Decision-Making
Clinical decision-making in operative obstetrics requires integrating the indication, the prerequisites, the skill level available, the setting's resources, and the patient's values and preferences — all within a compressed time frame. The decision is never purely technical; it is always contextual. A vacuum extraction that would be appropriate in a tertiary centre with a neonatologist present may be inappropriate in a rural district hospital where immediate CS capability is unreliable and there is no trained neonatologist. The right procedure in the wrong setting is still wrong. This contextual judgment — what is right here, now, with this patient, this team, and these resources — is what distinguishes a safe clinician from a technically competent but situationally unaware one. It is also what makes operative obstetrics inherently a team activity: the obstetrician, anaesthesiologist, midwife, theatre team, and neonatologist must all be notified, briefed, and ready before an instrument is picked up or a patient is positioned for LSCS. The pre-procedure communication is not a bureaucratic formality; it is itself a safety intervention that halves the chance of an avoidable error.
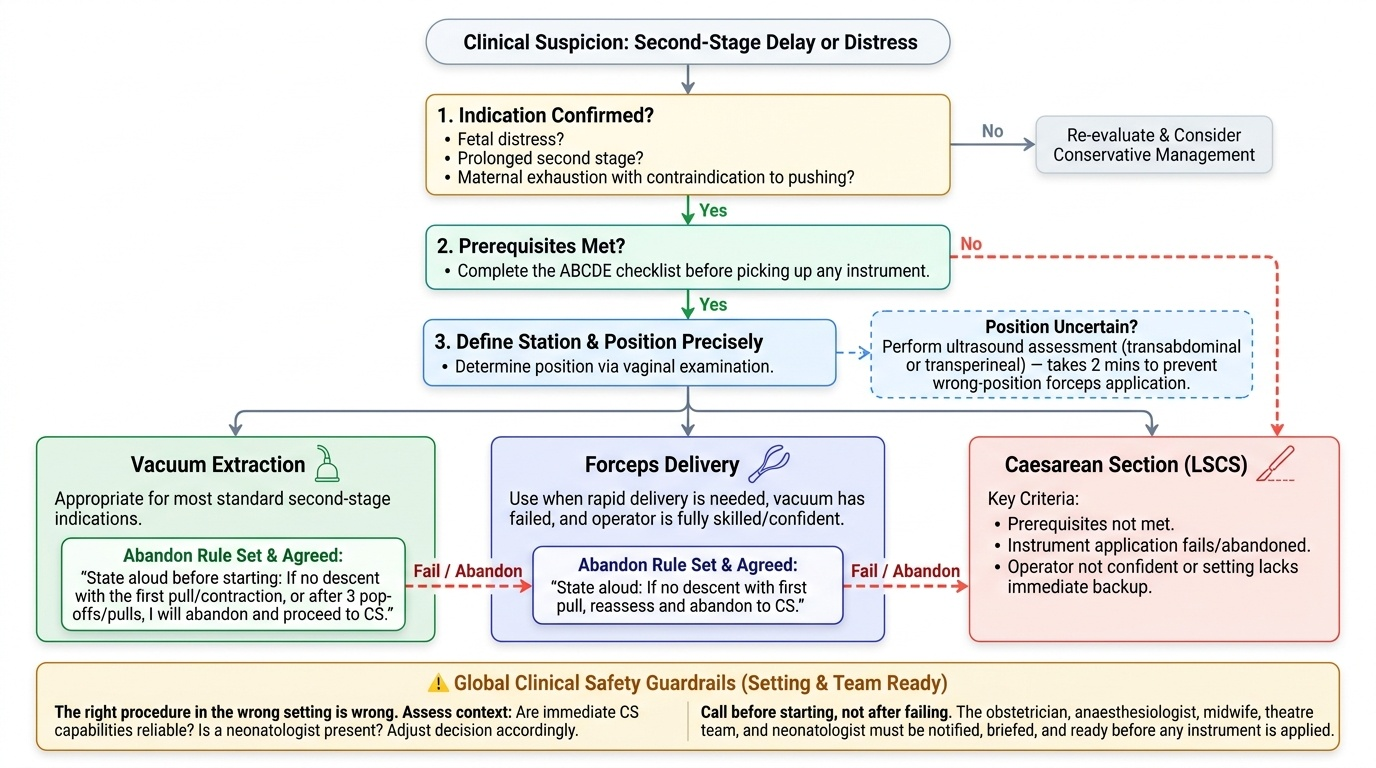
A structured decision framework for the second stage:
1. Indication confirmed? — fetal distress, prolonged second stage, maternal exhaustion with a contraindication to pushing?
2. All prerequisites met? — use the ABCDE checklist before picking up any instrument
3. Station and position defined precisely? — if position is uncertain on vaginal examination, ultrasound assessment of fetal position (transperineal or transabdominal) takes 2 minutes and prevents wrong-position forceps application
4. Right instrument for the situation? — vacuum for most second-stage indications; forceps when rapid delivery is needed or vacuum has failed; CS if prerequisites not met, instrument fails, or operator not confident
5. Abandon rule set and agreed? — before starting, the operator must state: 'If there is no descent with the first pull/contraction, I will reassess; after 3 pop-offs/pulls I will abandon and proceed to CS'
6. Theatre and neonatal team ready? — call before starting, not after failing
Provided image
The same structured reasoning applies to elective decisions — cerclage timing, ECV candidacy, planned CS for malpresentation. In each case the algorithm is: indication present → contraindications excluded → correct procedure identified → correct timing → perform with full consent and monitoring.
SELF-CHECK
You apply a Ventouse cup correctly at the flexion point. After three contractions with correct traction technique, the cup has popped off twice and the head has not descended. What is the most appropriate next step?
A. Apply a larger cup and continue vacuum extraction
B. Abandon vacuum extraction and proceed to emergency CS
C. Apply outlet forceps immediately since the head is engaged
D. Increase the suction pressure above 0.8 kg/cm² for the next pull
Reveal Answer
Answer: B. Abandon vacuum extraction and proceed to emergency CS
Two pop-offs with no descent indicates failed vacuum extraction. The RCOG guideline states that three pop-offs or 20 minutes total, or failure of head to descend with correct traction, mandates abandonment of vacuum. Proceeding directly to emergency CS is correct. Sequential use of vacuum then forceps in the same delivery increases maternal and neonatal trauma and is only considered in very specific circumstances by a senior operator. Increasing suction above recommended pressure risks scalp injury.
Self-Assessment
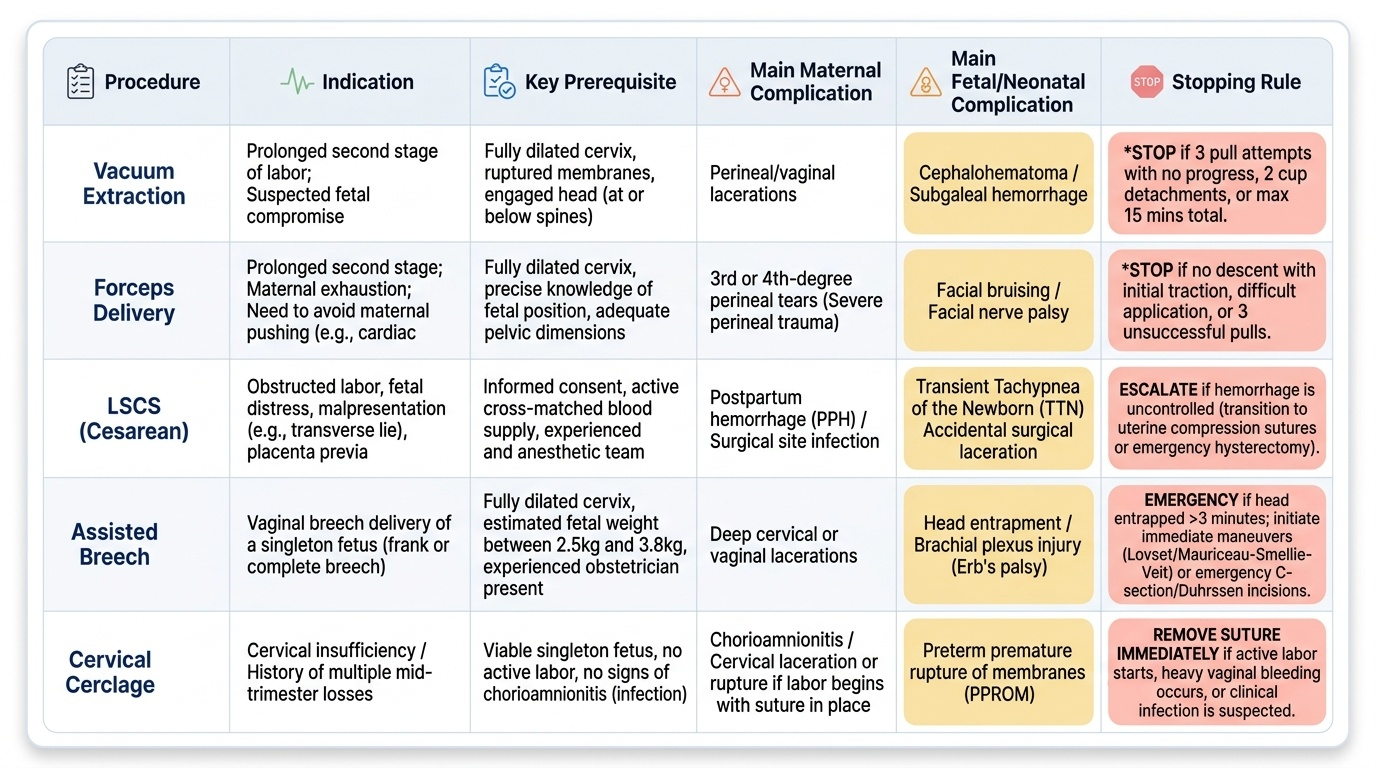
Operative obstetrics is a domain where knowledge and clinical judgment must translate into decisive, time-pressured action. The competency being assessed at your level is not operative skill but clinical reasoning: knowing when to intervene, which intervention is appropriate, what the stopping rules are, and when to escalate. This self-assessment section consolidates the key decision points across all the procedures covered.
For each procedure, mentally work through: What is the indication? What are the three most important prerequisites? What is the single most dangerous complication and how do you recognise it early? What is the stopping rule? Checking your answers against the content above will identify gaps. The micro-quiz questions in this SDL have been designed to test exactly these reasoning skills — scenario, decision, and justification — matching the format you will face in OSCE and viva assessments.
Provided image
Remember: the defining characteristic of a safe operative obstetrician is not technical dexterity alone — it is knowing when NOT to operate, and being willing to call for help, hand over, or change the plan when the clinical situation demands it.
SELF-CHECK
McDonald cerclage for cervical incompetence is typically removed at what gestation?
A. 28–30 weeks, before viability concerns arise
B. 34 weeks, as soon as the fetus is viable
C. 36–37 weeks, to allow spontaneous labour onset as a vertex
D. Only at the onset of established labour, whenever it occurs
Reveal Answer
Answer: C. 36–37 weeks, to allow spontaneous labour onset as a vertex
McDonald cerclage is electively removed at 36–37 weeks gestation to allow the cervix to efface and dilate normally for term labour. Removal before 34 weeks is not indicated unless infection or labour is present. Waiting for labour onset risks suture laceration or entrapment if the cervix dilates rapidly. Removal at 36–37 weeks is a simple outpatient procedure — cut and pull the suture.
SELF-CHECK
A neonate delivered by vacuum extraction develops a soft, fluctuant swelling of the entire scalp that crosses suture lines and is expanding over 4 hours post-delivery. What is the most likely diagnosis and the most important immediate concern?
A. Caput succedaneum — a benign finding that resolves within 24 hours
B. Cephalhaematoma — monitor for jaundice and allow spontaneous resolution
C. Subgaleal haemorrhage — risk of hypovolaemic shock requiring urgent resuscitation
D. Intracranial haemorrhage — immediate CT scan required
Reveal Answer
Answer: C. Subgaleal haemorrhage — risk of hypovolaemic shock requiring urgent resuscitation
Subgaleal haemorrhage is identified by a soft, diffuse, fluctuant swelling that crosses suture lines and enlarges over hours after birth. The subgaleal space can accumulate up to 260 mL of blood in a term neonate — sufficient to cause haemorrhagic shock and death. Urgent resuscitation (IV access, blood product transfusion, haematology referral) is required. Caput succedaneum is oedema that also crosses suture lines but is not fluctuant and resolves rapidly. Cephalhaematoma is firm, does NOT cross suture lines (subperiosteal), and is not acutely dangerous.
CLINICAL PEARL
The single most preventable error in instrumental delivery is proceeding without confirming the exact fetal head position. A forceps application with blades in the wrong planes will not advance the head and will cause cervical, vaginal, or fetal injury. If you are not 100% certain of the position on vaginal examination — particularly when the head is low in the pelvis with significant caput obscuring landmarks — take 90 seconds and perform a transperineal or transabdominal ultrasound to confirm. This small investment of time prevents the dangerous chain of events: wrong-position instrument → failed pull → abandonment under duress → delayed CS.