Page 14 of 22
OG15.2 | Episiotomy and Operative Obstetric Assistance — SDL Guide
Learning Objectives
- State the clinical indications for episiotomy and operative vaginal delivery
- Describe the relevant perineal anatomy including muscular layers and the anal sphincter complex
- Compare mediolateral and midline episiotomy in terms of technique, complications, and extension risk
- Outline the layer-by-layer episiotomy repair sequence including appropriate suture materials
- List the prerequisites for forceps and vacuum-assisted delivery and describe the assistant's role
- Describe the assistant's duties during a lower-segment Caesarean section
- Perform episiotomy repair on a perineal simulation model under supervision
- Recognise immediate post-procedure complications including perineal haematoma and sphincter injury
INSTRUCTIONS
Perineal trauma management and operative obstetrics represent a core set of skills every graduate must be competent to assist with and to perform under supervision. This module walks you through the clinical decision to intervene, the anatomy that governs safe incision and repair, and the practical tasks expected of a junior assistant at a forceps delivery, vacuum extraction, or Caesarean section. You will encounter these procedures in your internship from day one; the decisions about when and how to act carry direct consequences for both mother and baby.
References
- DC Dutta's Textbook of Obstetrics, 10th ed., Ch 16, 17, 18 (textbook)
- Williams Obstetrics, 26th ed., Ch 27 (operative vaginal delivery), Ch 30 (CS) (textbook)
- RCOG Green-top Guideline No. 26 — Operative Vaginal Delivery, 2011 (updated) (guideline)
- WHO Recommendations: Intrapartum Care for a Positive Childbirth Experience, 2018 (guideline)
- RCOG Green-top Guideline No. 29 — The Management of Third- and Fourth-Degree Perineal Tears, 2015 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
It is 0300 hours. A 24-year-old primigravida at 39 weeks has been in the second stage for 90 minutes. The fetal heart shows late decelerations to 90 bpm following each contraction. The presenting part is at the perineum, visible with pushing, but the perineum is thick and unyielding. The registrar turns to you: 'Prep for an episiotomy and get the Neville-Barnes forceps.' You have rehearsed this on the perineal model — you know the anatomy, you know where to cut, and you know how to repair. What do you do first?
WHY THIS MATTERS
Perineal trauma and operative delivery are among the most common intrapartum interventions worldwide. In India, episiotomy rates in institutional deliveries remain high, and forceps and vacuum extractions are performed daily at tertiary centres. As a Phase III student and soon an intern, you will assist at these procedures before you perform them independently. Understanding the indications, technique, and repair is not academic — a missed sphincter injury or a poorly repaired episiotomy leads to long-term anal incontinence, dyspareunia, and psychological harm to the mother. Mastery of this skill set is a NMC CBME competency (OG15.2) assessed by DOAP and skill assessment.
RECALL
Before continuing, activate your prior learning: From Anatomy, recall the perineal body (the fibromuscular structure at the centre of the perineum), the muscles of the superficial perineal pouch (bulbospongiosus, superficial transverse perinei, external anal sphincter), and the levator ani (pubococcygeus, iliococcygeus). From Physiology, recall how the second stage of labour involves uterine contractions stretching the perineum progressively — the mechanism of crowning. From your Obstetrics lectures, recall the definition of the second stage of labour (full dilatation to delivery), normal duration limits (primipara ≤2 hours active pushing; multipara ≤1 hour), and the distinction between a prolonged second stage and an obstructed labour. These form the foundation on which clinical decision-making about operative intervention rests.
When and Why: Indications for Episiotomy and Operative Delivery
The decision to perform an episiotomy or to proceed to operative delivery is a surgical judgment, not a reflex, and it must be made with clear clinical reasoning. The WHO 2018 recommendations explicitly state that episiotomy should not be performed routinely — it is a selective procedure justified only when the clinical situation demands it. Understanding why this matters is the starting point for competent practice. When you encounter the pressure of a distressed fetal heart trace or a stalled second stage, you will need to distinguish, without hesitation, between the situations that call for each intervention: a perineal incision, an instrument delivery, or an emergency abdominal operation. These are not interchangeable responses — each carries distinct risks and benefits, and choosing the wrong one, or delaying the right one, harms the mother or the baby.
Indications for episiotomy arise whenever the risk of an uncontrolled perineal tear or fetal compromise outweighs the harm of a deliberate, controlled incision. The key indications are:
- Fetal distress in the second stage (abnormal CTG, meconium-stained liquor with acidosis risk) where immediate delivery is needed but the perineum is the limiting factor
- Prolonged second stage where delay risks fetal or maternal exhaustion
- Operative vaginal delivery (forceps or vacuum) — episiotomy is performed in most forceps deliveries to accommodate the instrument blades and reduce uncontrolled perineal tearing; with vacuum it is selective, not mandatory
- Shoulder dystocia where additional manipulation space is urgently needed
- Preterm delivery where an unyielding perineum increases compressive force on a fragile fetal skull
- Rigid perineum that does not stretch despite adequate pushing — particularly in older primigravidae or those with previous perineal scarring
- Breech delivery where the aftercoming head may need additional space
Episiotomy is not indicated for: routine vaginal delivery, previous third-/fourth-degree tear (risk of re-extension), or purely for speed of delivery without another clinical reason.
Indications for operative vaginal delivery (forceps or vacuum) include: prolonged second stage unresponsive to adequate contractions and pushing; fetal distress in the second stage; maternal conditions requiring avoidance of Valsalva (cardiac disease, hypertensive crisis, raised intracranial pressure); and malrotation (occipito-posterior or deep transverse arrest) where rotational forceps or ventouse traction can complete delivery.
Indications for Caesarean section span an urgency spectrum. The NICE four-category classification organises CS by urgency: Category 1 (immediate life threat to mother or fetus — cord prolapse, placental abruption with acute fetal compromise, uterine rupture); Category 2 (maternal or fetal compromise not immediately life-threatening — prolonged second stage with failure to progress, suspected fetal compromise with reassuring reserve); Category 3 (early delivery needed, no immediate compromise — pre-labour rupture of membranes with planned CS, poorly controlled maternal disease); Category 4 (elective, patient/clinician decision — previous CS on patient request, placenta praevia, breech at term declining external cephalic version).
Cross-reference: for obstructed labour leading to emergency CS, see the og8-obstructed-labour SDL; for malpresentation as indication for assisted delivery, see og8-malpresentation.
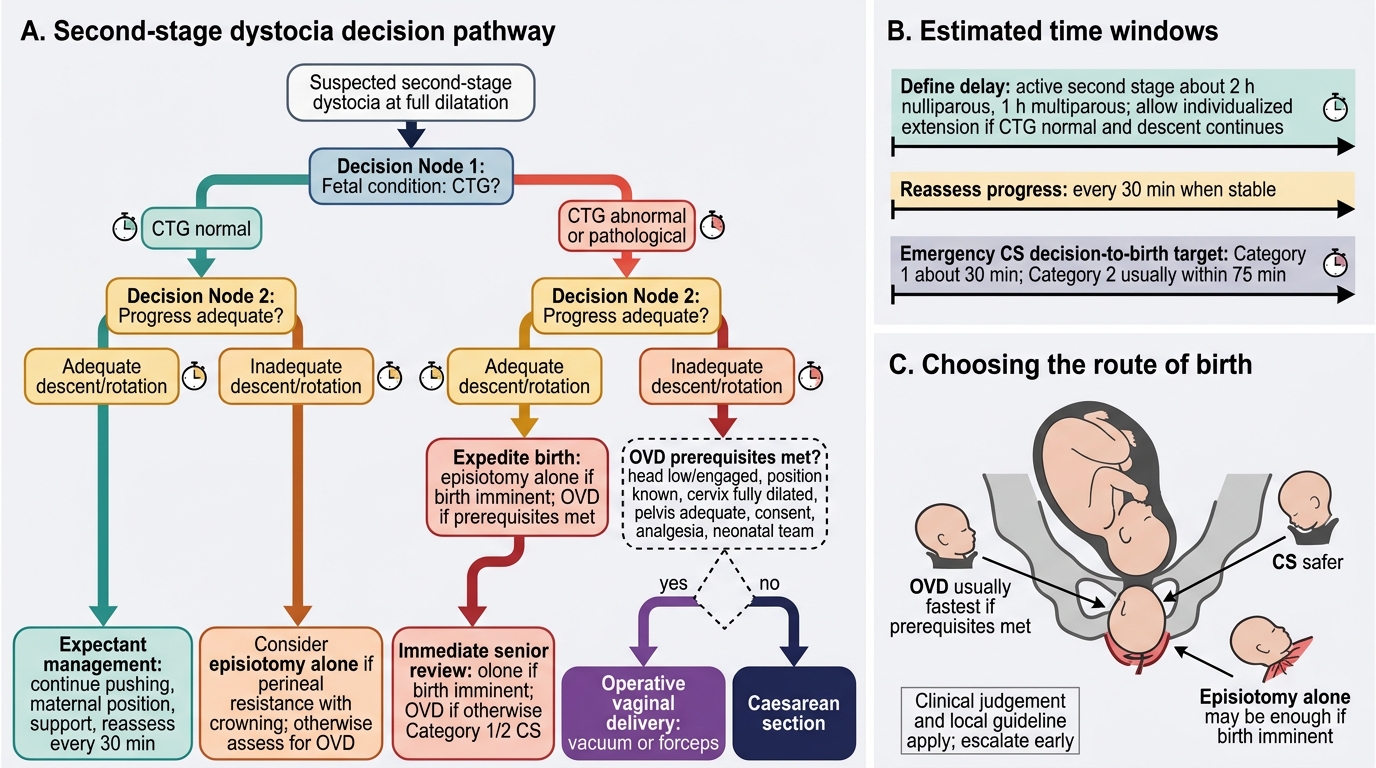
Decision Pathway for Second-Stage Dystocia
Perineal and Pelvic Floor Anatomy for the Operator
Safe episiotomy and repair depend entirely on knowing exactly what you are cutting through and what you must reconstitute layer by layer. The perineum in the obstetric context consists of three functionally distinct compartments, and the anal sphincter complex sits immediately behind the posterior fourchette — a fact with enormous clinical significance.
The superficial perineal pouch (between the perineal membrane and the skin) contains the muscles most relevant to episiotomy: the bulbospongiosus (encircles the vaginal introitus, contributes to perineal body), the superficial transverse perinei (runs transversely from ischial tuberosity to perineal body), and the ischiocavernosus (lateral, less relevant to midline repair). These muscles converge at the perineal body — a pyramidal fibromuscular mass at the centre of the perineum that anchors the vagina, uterus, and rectum and is the key structure to reconstruct during repair.
The deep perineal pouch contains the deep transverse perinei and the external urethral sphincter; it is bounded above by the levator ani (pubococcygeus + iliococcygeus + puborectalis), which forms the pelvic floor. In a second-degree tear or mediolateral episiotomy, the incision transects the bulbospongiosus and superficial transverse perinei at a minimum; deeper incisions or extensions involve the deep transverse perinei and, if extended posteriorly, the external anal sphincter (EAS).
The anal sphincter complex comprises: the EAS (voluntary, external, elliptical striated muscle encircling the anal canal; subclassified into 3a = partial EAS <50%, 3b = complete EAS >50% or completely through, 3c = EAS + internal anal sphincter) and the internal anal sphincter (IAS) (involuntary smooth muscle, thickened continuation of circular rectal wall; responsible for ~80% of resting anal tone). A fourth-degree tear additionally involves the rectal mucosa. Distinguishing EAS from IAS is critical at repair — the EAS is striated and pale/glistening; the IAS is smooth, whiter, and medial to the EAS.
Neurovascular supply: the pudendal nerve (S2–S4) supplies the external genitalia, EAS, and perineal skin; the pudendal artery runs with it through Alcock's canal. A pudendal nerve block (1% lignocaine 10 mL per side, injected just medial to the ischial spine via transvaginal or transperineal route) provides analgesia for perineal repair when regional anaesthesia is not in place.
For forceps design: the two blades have a cephalic curve (to fit the fetal head), a pelvic curve (to match the birth canal), a heel-lock mechanism, and a traction handle. Neville-Barnes (and Simpson) forceps have parallel shanks and are used for outlet/low-cavity traction without rotation. Kielland's forceps have a minimal pelvic curve and a sliding lock to allow asynclitism correction — used specifically for rotational delivery in malrotation. For vacuum extractors: the soft or rigid cup is placed over the flexion point (3 cm anterior to the posterior fontanelle on the sagittal suture) to flex and pull optimally; the traction force must be synchronised with maternal effort.
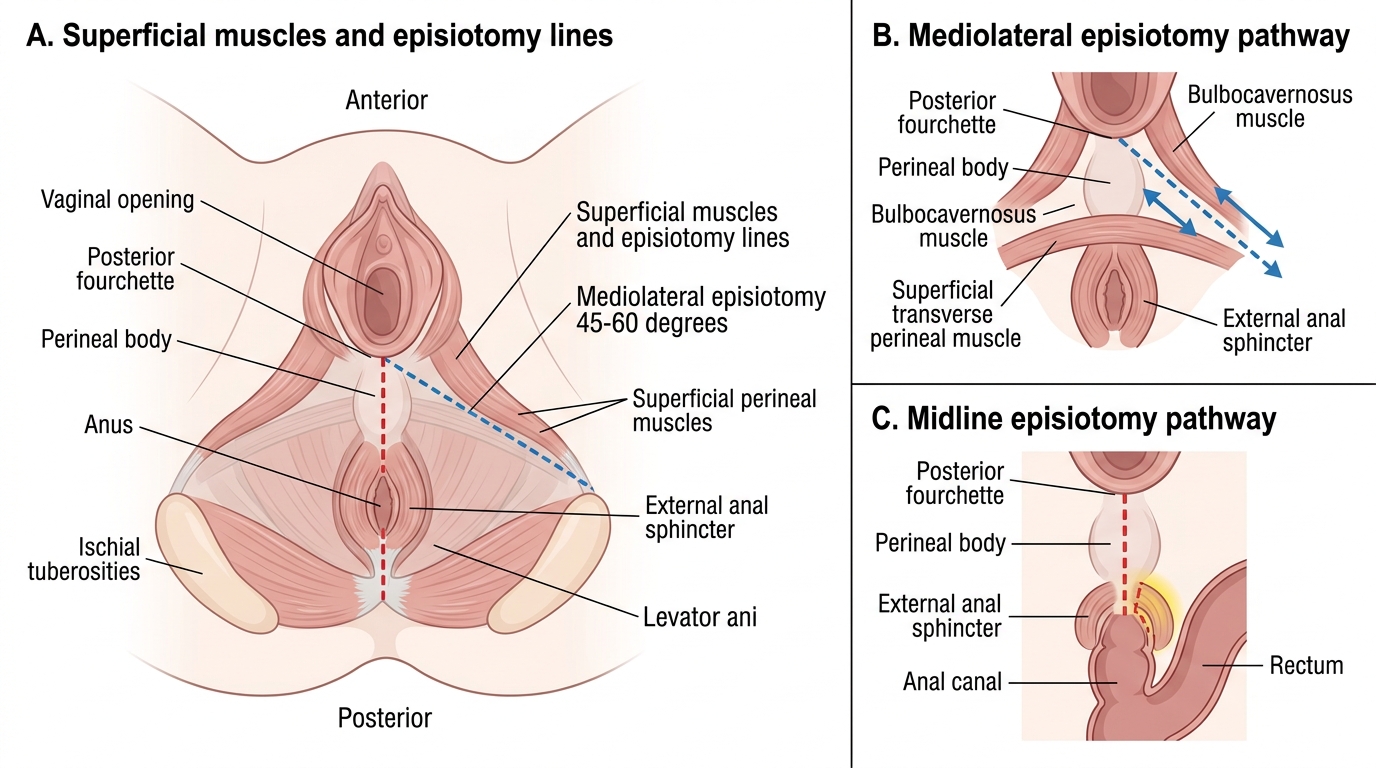
Female Perineum and Episiotomy Incision Lines
Episiotomy: Types, Timing, and Technique
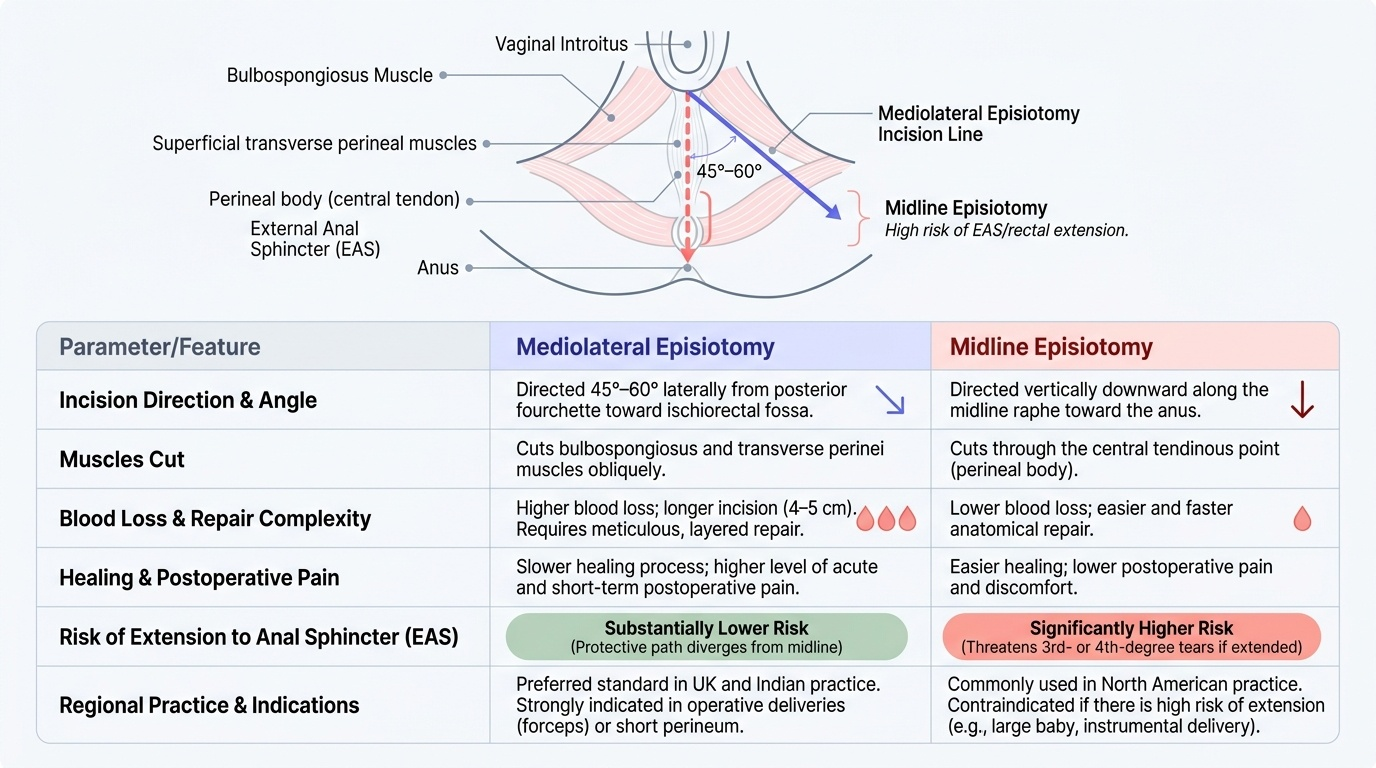
An episiotomy is a surgical incision of the perineum and posterior vaginal wall performed in the second stage of labour to enlarge the vaginal outlet. Two types are performed in practice: the mediolateral and the midline (median) episiotomy. Each has distinct anatomical, mechanical, and complication profiles that determine when each is preferred.
Mediolateral episiotomy is directed 45–60° to the right of the midline (in right-handed operators) from the posterior fourchette toward the right ischiorectal fossa. It cuts through the bulbospongiosus and transverse perinei muscles obliquely, and its direction intentionally diverges from the midline to reduce the risk of extension to the EAS and rectum. The incision is longer (4–5 cm), bleeds more, and requires more careful layer repair — but the extension rate to third- or fourth-degree tears is substantially lower than midline. Mediolateral is the preferred technique in most Indian and UK practice.
Midline episiotomy is directed vertically downward along the midline raphe from the fourchette toward the anus. It cuts through the central tendinous point and, if extended, directly threatens the EAS. The advantages are less blood loss, easier healing, and less postoperative pain — but the risk of extension to a complete sphincter tear (third-/fourth-degree) is significantly higher. Midline is more commonly used in North American practice; it is not recommended where there is a risk of the incision extending (large baby, forceps delivery, short perineum).
Provided image
Timing of episiotomy is as important as type. The incision should be made at full crowning — when 3–4 cm of the presenting part is visible at the introitus and the perineum is maximally stretched and thinned. Cutting too early (before crowning) leads to unnecessary muscle injury and more bleeding without the benefit of thinned tissue; cutting too late allows uncontrolled tearing. A single decisive cut with sharp Mayo scissors or episiotomy scissors is correct — a sawing motion creates a ragged wound and bleeds more.
Episiotomy technique:
1. Apply local anaesthesia if regional block is absent (1% lignocaine 5–10 mL infiltrated into the perineal tissue along the line of proposed incision, or pudendal block).
2. Two fingers of the left hand are inserted between the fetal presenting part and the perineum to protect the fetus.
3. The scissors are placed at the fourchette, angled 45–60° from midline (mediolateral), and a single firm cut of 4–5 cm is made through skin, subcutaneous tissue, bulbospongiosus, and transverse perinei.
4. The cut is made between contractions when the tissue is thinnest and least vascular, OR at the peak of a contraction if immediate delivery is required.
Episiotomy repair must reconstitute every anatomical layer precisely. Haemostasis throughout is mandatory. Use absorbable suture — polyglactin 910 (Vicryl) or polyglycolic acid (Dexon), 2/0 or 3/0 — on a curved needle.
Layer sequence:
1. Vaginal mucosa: identify the apex of the vaginal incision (often higher than expected — check carefully for bleeding points above the visible cut). Close with a continuous locking or continuous non-locking suture from the apex down to the hymeneal ring, ensuring mucosal edges are opposed without gaps.
2. Deep perineal muscles (transverse perinei, bulbospongiosus): one or two interrupted sutures to appose the perineal body. Correct apposition here is the key to long-term perineal integrity.
3. Superficial perineal fascia and muscles: interrupted or continuous sutures to close the remaining muscle.
4. Skin: subcuticular continuous suture (preferred over interrupted sutures for comfort and cosmesis) from the perineal body to the posterior fourchette.
After repair: perform a rectal examination to confirm no sutures have inadvertently penetrated the rectal mucosa, and ensure no missing swabs/instruments.
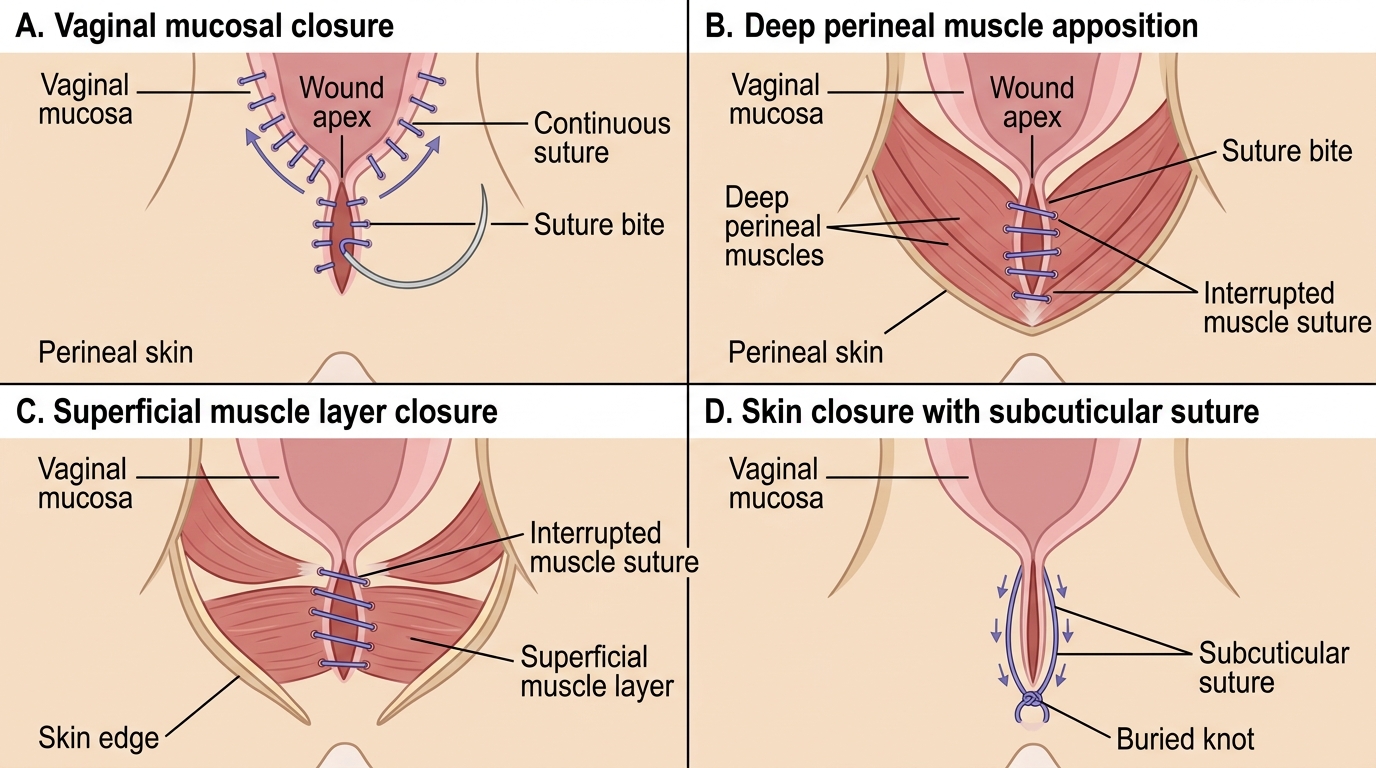
Stepwise Episiotomy Repair