Page 7 of 22
OG14.3 | Malpresentation and Malposition — SDL Guide
Learning Objectives
- Classify malpresentations and describe the defining characteristics of each type
- Diagnose malpresentation by abdominal and vaginal examination
- Describe the management of breech, face, brow, transverse lie, and occipitoposterior position
- Explain the indications, contraindications, and technique of external cephalic version (ECV)
- Understand the mechanism of occipitoposterior position and its management
INSTRUCTIONS
Malpresentation — any presentation other than a vertex — complicates approximately 4–6% of deliveries and is a major contributor to obstructed labour, emergency operative delivery, cord prolapse, and perinatal morbidity. Recognising a malpresentation at antenatal visits or early in labour, and understanding which presentations permit vaginal delivery and which require caesarean section, is a fundamental obstetric competency. This module covers the full range of malpresentations and the occipitoposterior malposition, with attention to the evidence on ECV and assisted breech delivery.
References
- DC Dutta's Textbook of Obstetrics, 9th edition, Chapter 28 — Malpresentations and Malpositions (textbook)
- Williams Obstetrics, 25th edition, Chapter 28 — Abnormal Presentation, Position, and Fetal Development (textbook)
- RCOG Green-top Guideline No. 20a — External Cephalic Version and Reducing the Incidence of Term Breech Presentation, 2017 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 26-year-old primigravida at 37 weeks attends her antenatal clinic. On abdominal examination you feel a hard, round, ballotable mass at the fundus and a soft, irregular mass at the pelvic inlet. The fetal heart is auscultated loudest above the umbilicus. Vaginal examination confirms a soft, irregular presenting part. What is the presentation? What investigations and management steps will you initiate today, and what are the delivery implications if no action is taken?
WHY THIS MATTERS
Malpresentation accounts for a substantial proportion of emergency operative deliveries, cord prolapse events, and perinatal asphyxia. Breech presentation occurs in 3–4% of term pregnancies; face and brow are rarer but critically important because failure to recognise them in labour leads to obstructed labour and maternal morbidity. External cephalic version, when performed correctly and in the right setting, prevents a caesarean section in approximately 1 in 3 women with term breech — a significant benefit in a world where rising CS rates carry their own risks. The occipitoposterior position is encountered in ~5% of labours at onset and is a common cause of prolonged, painful labour and instrumental delivery requests. Mastery of malpresentation management directly reduces operative intervention and improves outcomes.
RECALL
Recall the mechanism of normal labour for a vertex presentation in the occipitoanterior (OA) position: engagement (head enters the pelvis with occiput anterior), flexion, descent, internal rotation (occiput rotates anteriorly to lie behind the pubic symphysis), extension, restitution, and external rotation. The denominator — the reference bony point used to describe fetal position — is the occiput in a vertex, the mentum (chin) in a face, the sinciput in a brow, and the sacrum in a breech. Also recall Leopold's manoeuvres: first (fundal), second (lateral), third (presenting part), and fourth (descent/engagement) — the systematic abdominal examination method for determining lie, presentation, position, and engagement.
Clinical Presentation and Diagnosis of Malpresentation
The diagnosis of malpresentation begins with systematic abdominal examination using Leopold's manoeuvres, supplemented by vaginal examination and confirmed by ultrasound. The clinical features of each malpresentation are distinctive enough that an experienced examiner can diagnose them reliably on abdominal palpation alone, though ultrasound confirmation should always be sought before any intervention.
In breech presentation, Leopold's first manoeuvre reveals a hard, round, smooth, ballotable mass (the head) at the fundus — the fetal head is at the top, not the bottom. The second manoeuvre identifies the fetal back on one side and irregular fetal limbs on the other. The third manoeuvre reveals a soft, broad, irregular mass (the buttocks) at the pelvic inlet that does not ballot as freely as the head. The fetal heart is loudest above the umbilicus in breech. On vaginal examination (in labour), the presenting part is soft, irregular, and may have palpable ischial tuberosities, the sacrum (smooth curved surface), or feet.
In transverse (shoulder) presentation, the uterus appears broader than tall (oblique or transverse ovoid), with neither a head nor buttocks in the pelvis. The head is palpable in one iliac fossa and the breech in the other. The fetal heart is loudest in the periumbilical region. Vaginal examination reveals a shoulder or arm as the presenting part. A cord prolapse risk is significant whenever the presenting part is not a smooth vertex firmly engaged in the pelvis — this applies to transverse lie, footling breech, and compound presentations.
In face presentation, the occiput is deeply extended posteriorly and the face presents. Abdominally the back is concave (a groove between the occiput and the back due to hyperextension), and the fetal head feels unusually large because it is extended. Vaginally, the face is distinguished from the breech by the triangular shape of the mouth, the gum pads (hard), and the facial bones; the anus (breech) is a firm sphincter with no hard bony landmarks, and meconium may be present.
Common Malpresentations in Labour
Brow presentation (sinciput presenting) feels like a very large, poorly fitting head with a palpable orbital ridge and nose but no chin reachable vaginally. It presents the largest head diameter (mentovertical ~13.5 cm) and almost always requires CS unless it converts to either vertex or face during labour.
Pathophysiology: Mechanisms and Classification
Malpresentation results from any factor that prevents the fetal head from engaging in the maternal pelvis or that allows the fetus to lie in a non-vertex position. Understanding these factors explains both why malpresentation occurs and why it tends to persist or recur in certain women.
Breech presentation at term (3–4%) represents a failure of the normal process of head-down version that occurs as the uterus and fetus grow — the fetus gravitates toward the vertex position in the expanding globular uterus. Factors that impair this process include: uterine anomalies (bicornuate or subseptate uterus — the narrow horn accommodates the small breech more than the large head); placenta praevia (the placenta in the lower segment occupies the space where the head should engage); polyhydramnios (excessive fluid allows the fetus to float freely without fixing in a vertex position); oligohydramnios (restricts movement, fixing a non-vertex lie); fetal anomalies (hydrocephalus, anencephaly — abnormal head shape prevents engagement); multiple pregnancy (the second twin has no room to turn after the first is born); and grand multiparity (lax uterine and abdominal wall muscles allow the fetus to lie in any position).
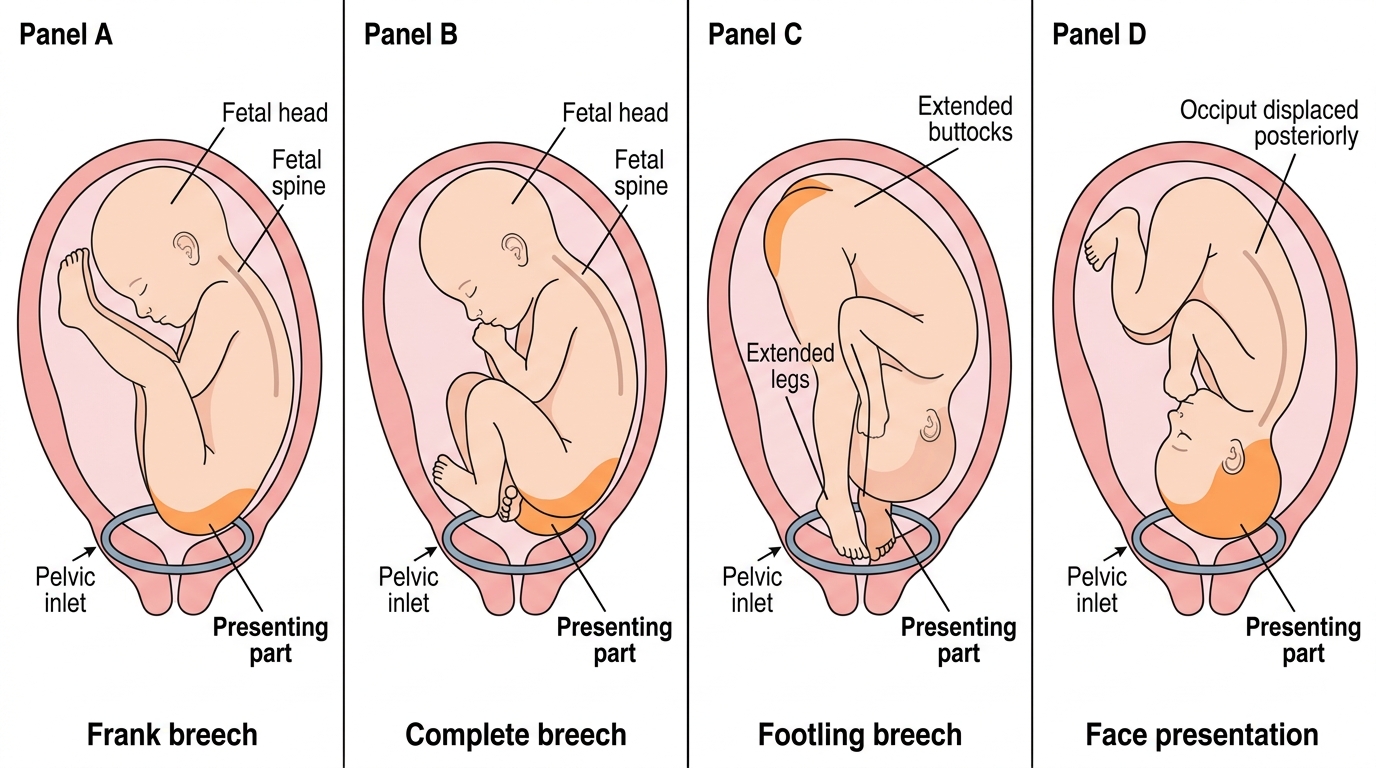
The types of breech and their relative frequencies are important:
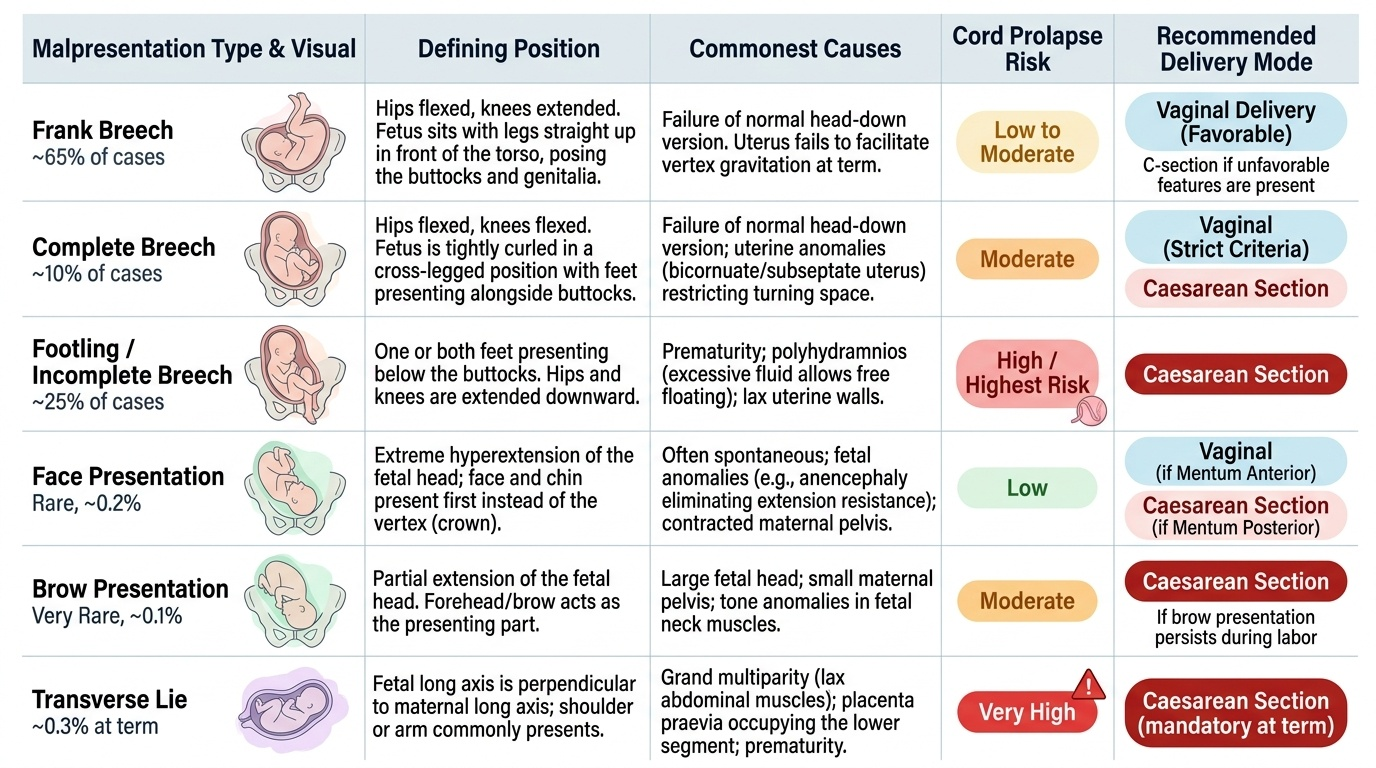
- Frank breech (~65%): hips flexed, knees extended — the fetus sits with legs straight up in front, presenting the buttocks and genitalia. Most common and most favourable for vaginal breech delivery if attempted.
- Complete breech (~10%): hips flexed, knees also flexed — the fetus is 'cannonball' positioned, with both feet alongside the buttocks.
- Footling/incomplete breech (~25%): one or both feet presenting below the buttocks. Highest risk of cord prolapse because the feet do not fill the pelvic inlet as firmly as the buttocks.
Provided image
Face presentation occurs from hyperextension of the fetal head, most often spontaneously without identifiable cause, though anencephaly (absent skull vault) eliminates the mechanical resistance to hyperextension. Brow presentation is an intermediate between vertex and face — if it persists, the presenting diameter is too large for most pelvic inlets. Transverse lie is associated with placenta praevia, polyhydramnios, pelvic tumour, multiparity, and contracted pelvis.
Investigation and Confirmation
Once malpresentation is clinically suspected from abdominal or vaginal examination, investigations are required to confirm the diagnosis precisely, exclude associated fetal anomalies, and gather the information needed to plan delivery safely. The two most important investigations are ultrasound and cardiotocography; clinical pelvic assessment is the third essential component, performed by the examining clinician. Ultrasound examination is the cornerstone: it confirms the exact presentation and position, identifies the type of breech (frank, complete, or footling), locates the placenta (critical before any planned version), measures amniotic fluid volume, assesses fetal anatomy for anomalies that might explain or complicate the malpresentation, and estimates fetal weight. These findings are not merely academic — they directly gate management decisions: a placenta praevia discovered on ultrasound means ECV is absolutely contraindicated; oligohydramnios is a relative contraindication; a hydrocephalic fetus requires a different delivery plan entirely.
Ultrasound findings to document for any malpresentation:
- Fetal presentation and position (confirm breech type — frank/complete/footling)
- Fetal biometry and estimated fetal weight (macrosomia increases CS preference)
- Amniotic fluid index or deepest vertical pool (oligohydramnios = ECV contraindicated; polyhydramnios = increased malpresentation risk and ECV failure risk)
- Placental location (anterior low-lying/praevia = ECV absolutely contraindicated)
- Fetal anatomy survey (hydrocephalus, anencephaly, nuchal cord if visible)
- Cardiotocography (CTG) before and after ECV to document fetal wellbeing
Clinical pelvic assessment is essential for any malpresentation managed towards vaginal delivery. Diagonal conjugate, bi-ischial diameter, and sacro-sciatic notch assessment guide the decision for VBAC breech delivery or assisted breech.
For occipitoposterior position, diagnosis is confirmed by vaginal examination in labour: the anterior fontanelle (larger, diamond-shaped, with four suture lines) is palpable anteriorly, and the posterior fontanelle (smaller, triangular, three sutures) is felt posteriorly or in the sacral region. Ultrasound can confirm the position if clinical examination is uncertain. An OP position should prompt assessment of whether the pelvis is adequate for the slightly larger presenting diameter and whether the contractions are driving efficient rotation.
SELF-CHECK
On vaginal examination in labour you feel a soft presenting part with a triangular opening containing hard ridges (gum pads), and the orbital ridge is palpable. What is the presentation, and what is the required condition for vaginal delivery?
A. Breech presentation — vaginal delivery is possible if the buttocks are at the perineum
B. Face presentation, mentum anterior — vaginal delivery is possible as the chin will deliver under the pubic symphysis
C. Face presentation, mentum posterior — vaginal delivery is impossible and CS is required
D. Brow presentation — vaginal delivery is possible with oxytocin augmentation
Reveal Answer
Answer: B. Face presentation, mentum anterior — vaginal delivery is possible as the chin will deliver under the pubic symphysis
The described findings (triangular mouth opening with hard gum pads, orbital ridge, no anus or sacrum) are consistent with face presentation. In mentum anterior position, the chin is under the pubic symphysis and the head can deliver by flexion; vaginal delivery is possible. In mentum posterior (chin facing sacrum), the head cannot flex further (it is already maximally extended) and CS is required. Brow presentation almost always requires CS due to the large presenting diameter.