Page 4 of 22
OG14.2 | Rupture Uterus — SDL Guide
Learning Objectives
- Classify uterine rupture as complete or incomplete, and by cause (scarred vs unscarred uterus)
- Describe the clinical features that distinguish impending rupture from established rupture
- Outline the immediate management including resuscitation and surgical options
- Discuss prevention strategies including VBAC counselling and antenatal risk stratification
INSTRUCTIONS
Uterine rupture is one of the most catastrophic obstetric emergencies — it carries a maternal mortality risk of up to 10% and a perinatal mortality of up to 80% in many settings if not managed within minutes. As obstetric practice increasingly involves women with previous caesarean section scars, understanding scar rupture — its subtle presentation, risk factors, and the evidence on trial of labour after CS — is a core clinical competency for every graduating doctor.
References
- DC Dutta's Textbook of Obstetrics, 9th edition, Chapter 36 — Rupture of the Uterus (textbook)
- Williams Obstetrics, 25th edition, Chapter 27 — Uterine Rupture (textbook)
- RCOG Green-top Guideline No. 45 — Birth After Previous Caesarean Birth (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 30-year-old G2P1 woman at 38 weeks gestation, with one previous lower-segment caesarean section, is admitted in active labour at a district hospital. She was progressing well at 6 cm an hour ago. Suddenly she screams, then goes silent. The contractions stop. The abdomen is no longer taut. The fetal heart cannot be found. On examination, the abdomen is diffusely tender, you can feel fetal parts that seem to have changed position, and her blood pressure is 80/50 with a pulse of 130/min. What has happened? What do you do in the next 60 seconds?
WHY THIS MATTERS
Uterine rupture is a true obstetric emergency measured in minutes. In well-resourced settings it occurs at a rate of about 1 in 200 trial-of-labour-after-caesarean (TOLAC) cases; in low-resource settings with neglected obstructed labour on an unscarred uterus, rates are higher and outcomes far worse. The trend of increasing caesarean section rates worldwide means that an increasing proportion of deliveries involve women with uterine scars, and every clinician who manages labour must understand when a VBAC is safe, what scar rupture looks and feels like, and how to respond surgically. This SDL will equip you with exactly that knowledge.
RECALL
Before working through this module, recall the anatomy of the uterus in labour. The upper uterine segment contracts and retracts actively — it thickens progressively. The lower uterine segment (LUS) is the passive, thin zone between the internal os and the anatomical lower segment — it stretches and thins to accommodate the descending fetus. The Bandl's pathological retraction ring, which you studied in the obstructed labour module, marks the junction between these two zones and rises as the LUS is progressively stretched. The LUS is also where the transverse incision of a lower-segment caesarean section is placed, creating the scar that is the most common origin of uterine rupture in modern practice. A previous classical (vertical) caesarean section creates a body scar in the thick, actively contracting upper segment — this has a much higher rupture risk than a lower-segment scar.
Clinical Presentation of Uterine Rupture
Uterine rupture is the tearing of the uterine wall, partial or complete, occurring before or during labour. Its presentation depends on whether the rupture is complete (all layers, including visceral peritoneum) or incomplete (myometrium torn but serosa intact — also called dehiscence), and on whether it occurs on a scarred or unscarred uterus.
The classical presentation of complete rupture of an unscarred uterus — most often following neglected obstructed labour — is dramatic and unmistakable. There is sudden, acute, tearing abdominal pain at the height of a contraction, followed by an abrupt cessation of contractions as the uterine pressure is lost. The woman's condition rapidly deteriorates: she becomes pale, sweaty, tachycardic, and hypotensive as blood fills the peritoneal cavity. On abdominal examination, the uterine contour is lost — the fetus is no longer confined within a tense uterine globe but seems to lie freely under the abdominal wall. Fetal parts may be more superficially palpable than before. The fetal heart is absent in most complete ruptures because fetal exsanguination or placental separation is rapid. The previously noted Bandl's ring may have disappeared as the uterus relaxes after tearing.
By contrast, scar dehiscence of a lower-segment CS scar is frequently silent. The scar separates gradually and may only be discovered at the time of repeat CS as a window or thinned area. There is little or no haemorrhage (the visceral peritoneum contains the bleed), the fetal heart remains reassuring, and the clinical picture is much less dramatic. Between these extremes, incomplete scar rupture may present with scar tenderness (pain localised to the lower uterine segment just above the pubic symphysis), non-reassuring CTG patterns (variable or late decelerations), and haematuria from bladder involvement.
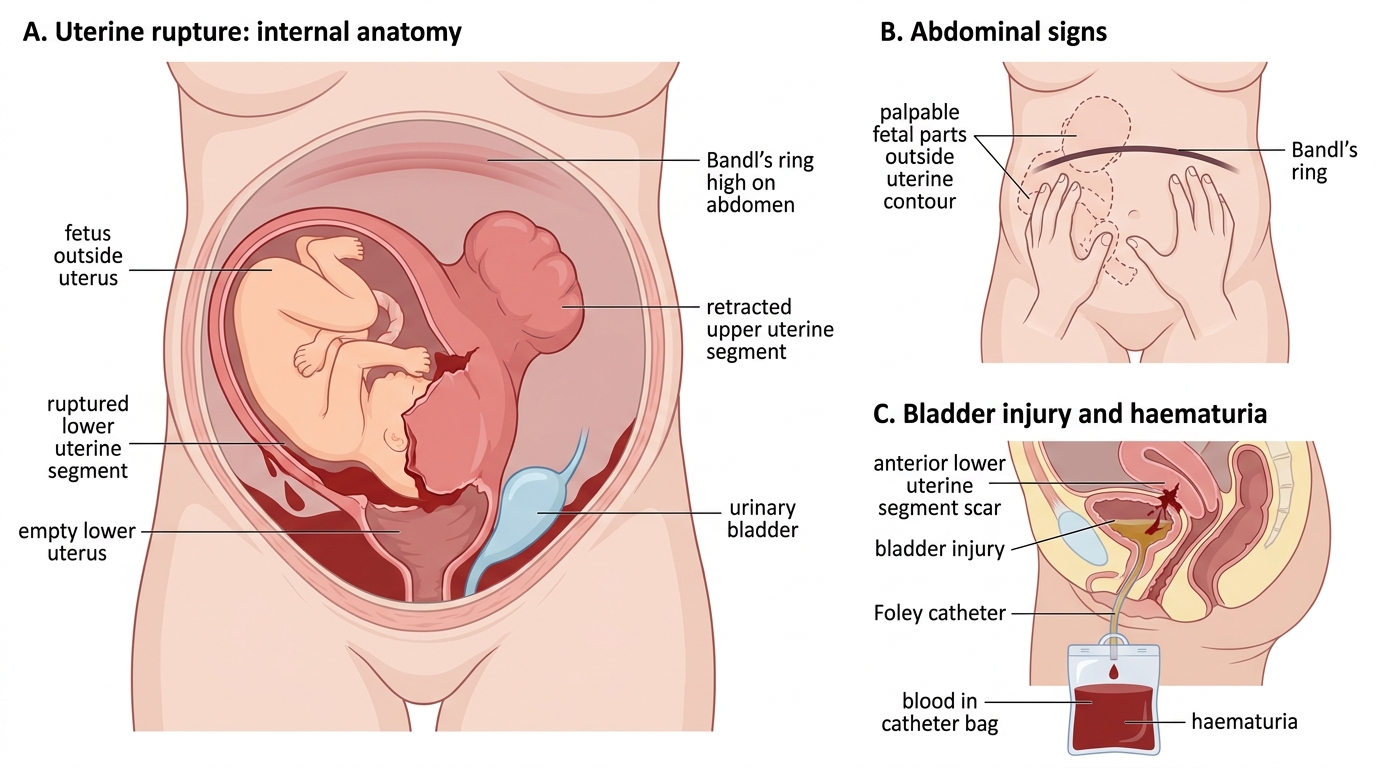
Clinical Signs of Uterine Rupture
Haematuria is a particularly important clinical sign: the urinary bladder lies immediately anterior to the lower uterine segment and is frequently injured during rupture of an anterior LUS scar, producing blood in the catheter bag. In any woman in labour with haematuria, scar tenderness, and a non-reassuring CTG, scar rupture must be the primary diagnosis until proven otherwise.
Pathophysiology and Causes
The pathophysiology of uterine rupture centres on the relationship between myometrial tensile strength and the forces acting upon it during labour. When the force exceeds the strength — whether because the wall is weakened by a scar, the force is pathologically elevated by obstruction or injudicious oxytocin, or the uterus is abnormally thin from grand multiparity — the wall tears.
In scarred-uterus rupture, the scar tissue that replaces normal myometrium after a previous CS lacks the elasticity of intact muscle. Under the mechanical stress of uterine contractions in labour, particularly at the transition from latent to active phase when intrauterine pressure rises sharply, the scar may separate. The lower-segment transverse scar generally gives way gradually and bleeds relatively slowly (the LUS is poorly vascularised); the classical vertical scar involves the vascular upper segment and bleeds rapidly. A previous myomectomy scar, especially if the uterine cavity was entered, carries a rupture risk comparable to a classical CS.
Unscarred-uterus rupture is almost invariably caused by neglected obstructed labour. The pathophysiology mirrors what was described in the obstructed labour module: the LUS is progressively stretched thinner until it tears, often at a point already weakened by ischaemia from prolonged head pressure. Grand multiparity contributes by causing myometrial thinning from repeated stretching. Injudicious use of oxytocin — particularly high-dose infusions in a multipara or in the presence of malpresentation or CPD — can drive the uterus to rupture by generating intrauterine pressures beyond what the myometrium can bear. Traumatic rupture (road traffic accidents, external version, difficult instrumental delivery) is less common.
Provided image
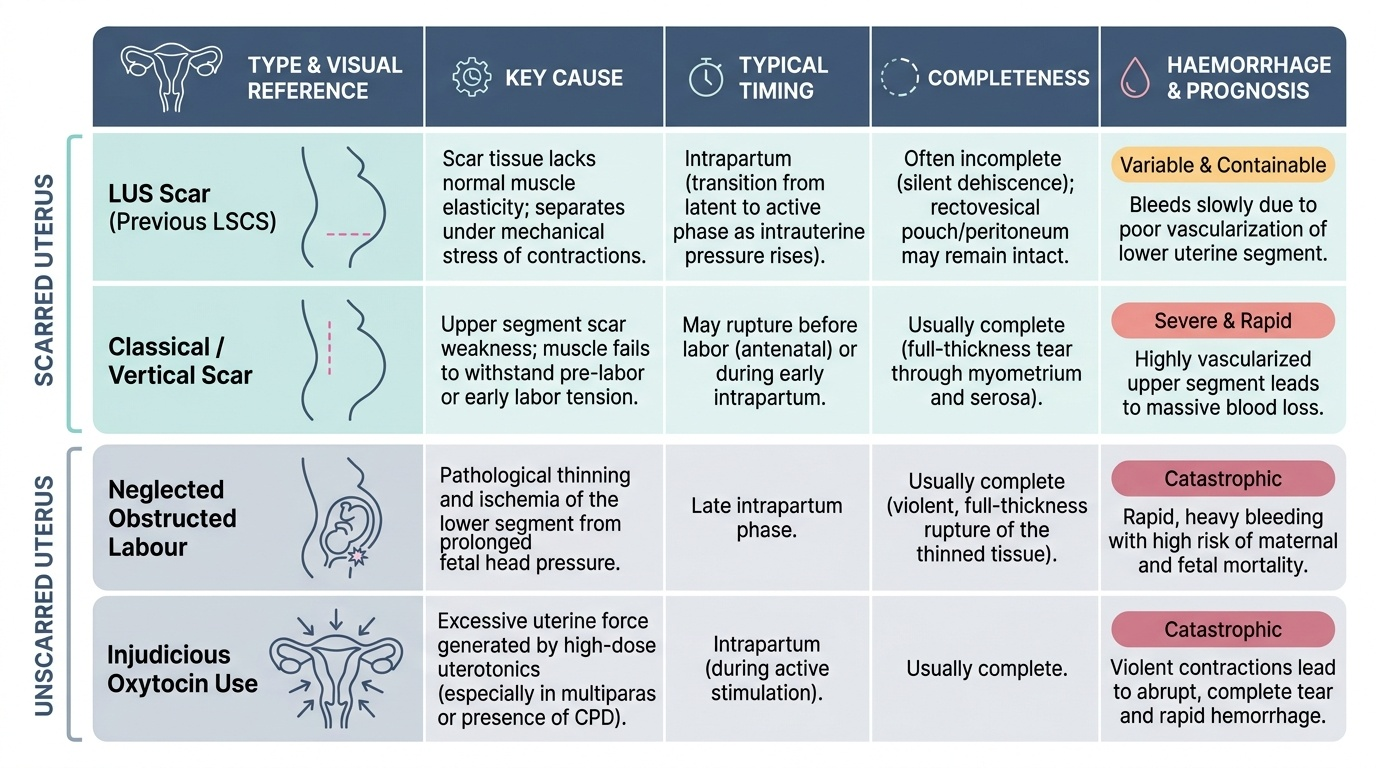
| Type | Key cause | Typical timing | Completeness | Haemorrhage |
|---|---|---|---|---|
| LUS scar (previous LSCS) | Scar weakness under labour | Intrapartum, active phase | Often incomplete (dehiscence) | Variable — can be contained |
| Classical/vertical scar | Upper segment scar weakness | May rupture before labour | Usually complete | Severe — upper segment is vascular |
| Unscarred uterus | Neglected obstructed labour | Late intrapartum | Usually complete | Catastrophic |
| Injudicious oxytocin | Excessive uterine force | Intrapartum | Complete | Severe |
| Traumatic | External force / operative | Any time | Variable | Variable |
Diagnosis
Uterine rupture is a clinical diagnosis — in the acute setting, there is neither time nor need for imaging. The diagnosis must be made on the history and examination within seconds to minutes, because the window for saving the mother and fetus is extremely narrow. Every clinician who manages labour must carry a mental checklist of the diagnostic features of rupture and run through it instantaneously whenever a woman in labour deteriorates acutely.
The diagnostic criteria that together establish the diagnosis are: (1) acute onset of abdominal pain that differs from contractions in character and persistence; (2) sudden cessation of contractions (the uterus can no longer generate pressure once its wall is breached); (3) maternal haemodynamic deterioration (tachycardia, hypotension, pallor) disproportionate to any visible bleeding — most haemorrhage is intraperitoneal; (4) change in uterine contour or palpation of fetal parts outside the expected uterine outline; (5) fetal heart rate changes (sudden severe bradycardia, absent FHR) as fetal compromise follows rupture rapidly; (6) haematuria, particularly in LUS scar rupture.
The most important differential is placental abruption — also causing sudden abdominal pain and fetal distress. Distinguishing features: in abruption, the uterus is typically woody-hard and contracted (haemorrhage is concealed within the uterus or decidua), not soft and relaxed as in rupture; contractions continue in abruption; the fetal outline remains within the uterine contour; and haemodynamic shock in abruption may be accompanied by vaginal bleeding. However, in practice the two emergencies can coexist, and laparotomy may be needed to determine the diagnosis definitively.
For scar surveillance in VBAC labour, the early warning signs are more subtle: uterine scar tenderness (pain on palpation over the LUS scar site, between contractions), non-reassuring CTG patterns — particularly variable decelerations or a prolonged bradycardia — and haematuria. Any one of these in a VBAC labour should prompt urgent clinical review and a low threshold to proceed to emergency CS.
SELF-CHECK
A woman with a previous LSCS is in VBAC labour at 8 cm. The CTG shows a sudden prolonged bradycardia to 80 bpm lasting 3 minutes, and the attending nurse notes blood in the urinary catheter bag. What is the most urgent next step?
A. Repeat vaginal examination to assess progress
B. Increase the oxytocin infusion to expedite delivery
C. Activate the emergency team and prepare for immediate laparotomy
D. Wait for 10 more minutes to see if the bradycardia resolves
Reveal Answer
Answer: C. Activate the emergency team and prepare for immediate laparotomy
Prolonged fetal bradycardia with haematuria in a VBAC labour is scar rupture until proven otherwise. The correct response is immediate activation of the surgical team and emergency laparotomy. Increasing oxytocin in suspected scar rupture is dangerous. Vaginal examination will not diagnose rupture and wastes time. Waiting risks maternal and fetal death.